Translate this page into:
Relationship between VKORC1 single nucleotide polymorphism 1173C>T, bone mineral density & carotid intima-media thickness
Reprint requests: Dr Laura Poanta, Nicolae Pascaly 9/16 str, 400431, Cluj Napoca, Romania e-mail: laurapoanta@yahoo.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The effects of vitamin K-dependent proteins in bone mineralization and vascular calcification and the implication of vitamin K epoxide reductase gene (VKORC1) 1173C>T polymorphism in warfarin sensitivity are well known. The main objective of the study was to investigate the relationship between VKORC1 1173C>T polymorphism, bone mineral density (BMD), and atherosclerosis (evaluated by intima-media thickness of the carotid artery and the presence of calcified plaques) in patients suspected to have osteoporosis or osteopenia and referred for BMD determination.
Methods:
VKORC1 1173C>T polymorphism was evaluated in 239 consecutive patients referred by their physicians for BMD measurement (dual energy X-ray absorptiometry at L2-L4 lumbar spine, femoral neck and total hip). Ultrasonography of the carotid arteries was performed, intima-media thickness (IMT) was measured and the presence of atherosclerotic calcified plaques was recorded.
Results:
In the patients with osteoporosis and osteopenia there was a higher frequency of TT genotype of VKORC1 1173C>T (P=0.04). The TT genotype was significantly more frequent in the osteoporotic group compared to the osteopenic group (P=0.01). The mean age and body mass index were lower in the patients with normal BMD and TT genotype (P=0.02, P=0.03). There was no correlation between the IMT and VKORC1 1173C>T genotype but the TT genotype had a significant association with the presence of calcified atherosclerotic plaques (P=0.05). This finding was not correlated with normal or pathologic BMD.
Interpretation & conclusions:
VKORC1 1173C>T polymorphism (TT genotype) was associated with osteoporosis and calcified plaques in the carotid artery in patients referred for BMD measurement. Different mechanisms are probably involved in these associations. TT genotype may serve as a potential genetic marker for the risk of OP and ATS.
Keywords
Atherosclerotic plaque
bone mineral density
carotid intima-media thickness
gene
osteoporosis
vitamin K epoxide
reductase
VKORC1

Osteoporosis (OP) and atherosclerosis (ATS) have a higher prevalence in the ageing population causing serious morbidity and mortality. The common mechanisms in the pathogenesis of OP and vascular calcification suggested are age-related, chronic inflammation, cigarette smoking, diabetes mellitus, estrogen deficiency, hypovitaminosis C, D, and K, oxidized lipids and free radical, or renal failure1234. Many studies have demonstrated the association between OP and ATS: bone mineral density (BMD) and the number of carotid and femoral atherosclerotic plaques5, BMD and the risk for subclinical coronary atherosclerosis6, BMD and carotid intima-media thickness (IMT) in postmenopausal women7, BMD and coronary calcification8, or calcification of the atherosclerotic plaques and low BMD910.
The role of vitamin K in bone metabolism and vascular health has been demonstrated. The characterization of vitamin K-dependent proteins has demonstrated the implication of vitamin K not only in the blood coagulation but also in the bone metabolism, atherosclerosis and in inflammation, oxidative stress, nerve signaling and even kidney stones11. Vitamin K acts as a cofactor for gamma-glutamyl carboxylase, being an electron donor for the conversion of some post-translational glutamyl residues, thus producing the gamma-carboxyglutamate (Gla). The main function of these Gla residues is to actively bind calcium, which is essential for the biological activity of the Gla containing proteins (named Gla-proteins)12. The mediator in the recycle process of vitamin K 2,3 epoxide to the vitamin K hydroquinone is vitamin K epoxide reductase (VKOR). The vitamin K epoxide reductase gene (VKORC1) is situated on human chromosome 16p11.2 and encodes a protein of 163 amino acids with a mass of 18.2 kD13. Numerous single nucleotide polymorphisms (SNPs) were identified, the VKORC1 gene being highly polymorphic. One of these SNPs, rs 993448 or VKORC1 1173C>T was studied especially in relation to coumarin sensitivity. D’Andrea et al14 found that patients with TT genotype of SNP rs 9934438 (SNP 1173) require a lower dose of warfarin for a safe anticoagulation. This is indicative for a lower activity of the coagulation system partly due to a lower activity of VKORC1 gene which leads to a less conversion of vitamin K epoxide to its reduced form and so to less carboxylation of the vitamin K-dependent proteins14. On the same haplotype with SNP 1173C>T is situated another SNP +2255C>T (rs 2359612) and for this SNP the presence of C allele is associated with almost double the risk for vascular diseases and lower levels of undercarboxylated osteocalcin15.
Recently a significant association between AA genotype of 9041G>A SNP and a higher mean BMD was found16 and in VKORC1-deficient mice a reduced length of bone calcification relative to wild-type control mice was demonstrated17. From six VKORC1 SNPs genotyped and compared with BMD, rs7292 was found to be associated with OP in non-hispanic white males18.
It remains undecided whether there is a common VKORC1 SNPs that can be considered a risk factor for both OP and ATS, and if there is a common pathway for the intervention in this polymorphism. Thus, the objective of the study was to evaluate the relationship between BMD, carotid IMT and calcific atherosclerotic plaques (as the risk factor for cardiovascular events due to atherosclerosis)19, and the VKORC1 SNPs rs 993448 (VKORC1 1173C>T) in patients referred for BMD determination.
Material & Methods
Between September 2009 and September 2010, 239 patients were consecutively enrolled from patients referred by their physicians for BMD measurement in the Rheumatology Clinic of the “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania. Patients with hormonal replacement therapy or medication affecting the bone metabolism (oral anticoagulants, corticosteroids, or anticonvulsants) were excluded. Subjects with any condition that might interfere with the bone metabolism, such as thyroid disorders, malabsortion, chronic renal and liver diseases or alcoholism were also excluded. Women were eligible if menopause had occurred at least two years prior to their visit. None of the subjects had diseases (fractures, etc.) that interfered with the activities of normal daily life. In this group 151 patients had hypertension and 60 patients had non-insulin-dependent diabetes (with 46 having both diseases).
Written, informed consent for participation was obtained from each subject prior to enrolment. The Ethics Committee of University approved the study protocol (ANCS 42107/2008 PNII Grant). All the measurements were performed in the same day.
For each patient demographic and clinical variable were recorded: age, weight, height, body mass index (BMI = weight/height2, kg/m2), time since menopause had installed, smoking status. The patients’ medication history and associated diseases including hypertension and diabetes were also recorded. Their blood pressure was measured after a 10 min rest in the supine position using a sphygmomanometer on the right arm of the subject.
Blood samples were drawn from the antecubital vein in the morning after the subject had fasted for 12 h. One sample (7 ml) was used for serum concentration of total cholesterol, triglycerides, and glucose determination by standard laboratory techniques (Cobas Mira Plus analyzer) on the same day. The second sample (5 ml) was used for DNA extraction. The samples obtained were kept frozen at -80°C until use.
BMD measurement: BMD was measured at the lumbar spine (L2-L4) and at the femoral neck by dual energy X-ray absorptiometry (DXA), using a Lunar Prodigy Advance (GE Healthcare, USA) for all BMD measurements. Results were expressed as a T-score (standard deviation from peak adult BMD). Patients were classified as having normal BMD, osteopenia or low bone mass (a value for BMD that was 1-2.5 SD below the mean value for young adults), and osteoporosis (more than 2.5 SD below the mean value for young adults according to the World Health Organization's criteria for diagnosing osteoporosis)20. Three sites for assessment of the BMD were considered: L2-L4 at the lumbar spine, femoral neck and total hip and the lower value of these three were used in the statistical analysis21. All the measurements were performed by two operators. The inter- and intra-operator coefficient of variation was less than 1.3 per cent.
Measurement of carotid IMT: The wall thickness of the carotid artery was measured bilaterally with Aloka Prosound alpha 10, Tokyo, Japan machine, using 7.5 to 13 MHz linear probe by the same examiner with the patient in supine position. The common carotid arteries were scanned longitudinally. The image was focused on the posterior (far) wall. The perpendicularity between the ultrasound beam and the far wall assured good visualization of the IMT as two parallel echoic lines (the lumen-intima interface and media-adventitia interface). In all cases, three measurements of the common carotid artery far wall were taken 10 mm proximal to the bifurcation. For each subject the mean value of the three measurements was considered to be the current wall thickness of the distal carotid common artery. The mean value taken into account for the study was between the right and left carotid artery IMT. The variability of ultrasonographic measurement was assessed by performing two measurements in a 15 volunteers group over a one week period. The coefficient of variation between the two IMT measurements was of 10 per cent.
The calcified atherosclerotic plaque was defined as a high echogenic focal widening of the carotid wall with the protrusion into the lumen, associated with posterior shadow. The plaques were recorded as present or absent on the common, internal and external carotid arteries walls.
DNA isolation and genotyping: DNA was obtained by extraction and purification from 300 μl of peripheral blood, using a comercial extraction kit (Wizard Genomic DNA Purification Kit, Promega, USA).
VKORC1 1173C>T polymorphism genotyping protocol used PCR-RFLP (Restriction fragment lenght polymorphism, based PCR), using a modified protocol described by Kimmel et al22. Briefly, a 195 bp fragment from the gene that encodes VKORC1, was amplified by PCR, following the amplification programme: initial denaturation of 7 min at 95°C, followed by 45 cycles, each of 40 sec denaturation at 95°C, annealing 50 sec at 59°C and elongation 40 sec at 72°C, with a final elongation of 7 min at 72°C. DNA primer sequences were: Fw_5’- AAGATGAAAAGCAGGGCCTAC- 3’ and Rev_5’- CCGAGAAAGGTGATTTCCAA- 3’. DNA samples were amplified by PCR in a final volume of 25 μl, with: MgCl2, 1.5 mM, dNTPmix 0.2 mM each, BSA (Bovine serum AlbumineR, Fermentas MBI, Lituania) 2 mg/ml, 1.25 U of TrueStart DNA polymerase (Fermentas MBI, Vilnius, Lituania), 10 pmoles of each primers (forward and reverse), approximately 150 ng of genomic DNA and nuclease free water up to the final volume of 25 μl. From the obtained amplicon 12 μl was digested overnight, at 37°C with 5U of Eco130I (StyI) (Fermentas MBI, Vilnius, Lituania) restriction enzyme. Digested fragments were migrated in electrophoresis gel, 3 per cent using high resolution MetaPhor agarose (Lonza, Belgium), stained with ethidium bromide. In the presence of T allele, the amplicon is digested by the enzyme in two fragments of 125 and 70 bp. The homozygous genotypes for C allele, present a single fragment of 195 bp, resistant to digestion. The homozygous genotypes for T allele, present 2 fragments, one of 125 bp and the other of 70 bp.
Statistical analysis: For testing normal distribution in the case of a continuous variable Kolmogorov-Smirnov test or Shapiro-Wilk test (for small samples) was applied. If the variables were normally distributed, the means were compared by t test (in case of two samples) or ANOVA test followed by post-hoc Scheffe analysis (in the case of three samples). If the variables were not normal distributed, the means were compared using Mann-Whitney test (in case of two samples) or Kruskal-Wallis test (in case of three samples) followed by Mann-Whitney test for multiple comparisons with Bonferroni manual adjustment. For testing proportions Chi-square test was used. For multiple comparisons Bonferroni manual adjustment of type 1 error were made.
In the absence of a cut-off value for the mean IMT, the association between mean IMT, BMD and 1173C>T polymorphism were analysed using the ANOVA two-way analysis. The study was made using genotype model (TT, CT, and CC), recessive model (TT versus CT plus CC), and dominant model (TT plus CT versus CC). For the association between a dependent dichotomous variable and multiple nominal or continuous independent variables a multivariate logistic regression was used. Multiple logistic regression analysis was performed with BMD (normal vs. osteopenia or osteoporosis) as a dependent variable and age, BMI, hypertension, diabetes mellitus, the VKORC1 genotype, and mean IMT as independent variables. Statistical calculations were performed with SPSS 13.0 (Chicago, IL, USA).
Results
The study group consisted of 204 women and 35 men. The characteristics of the study group are summarized in Table I.
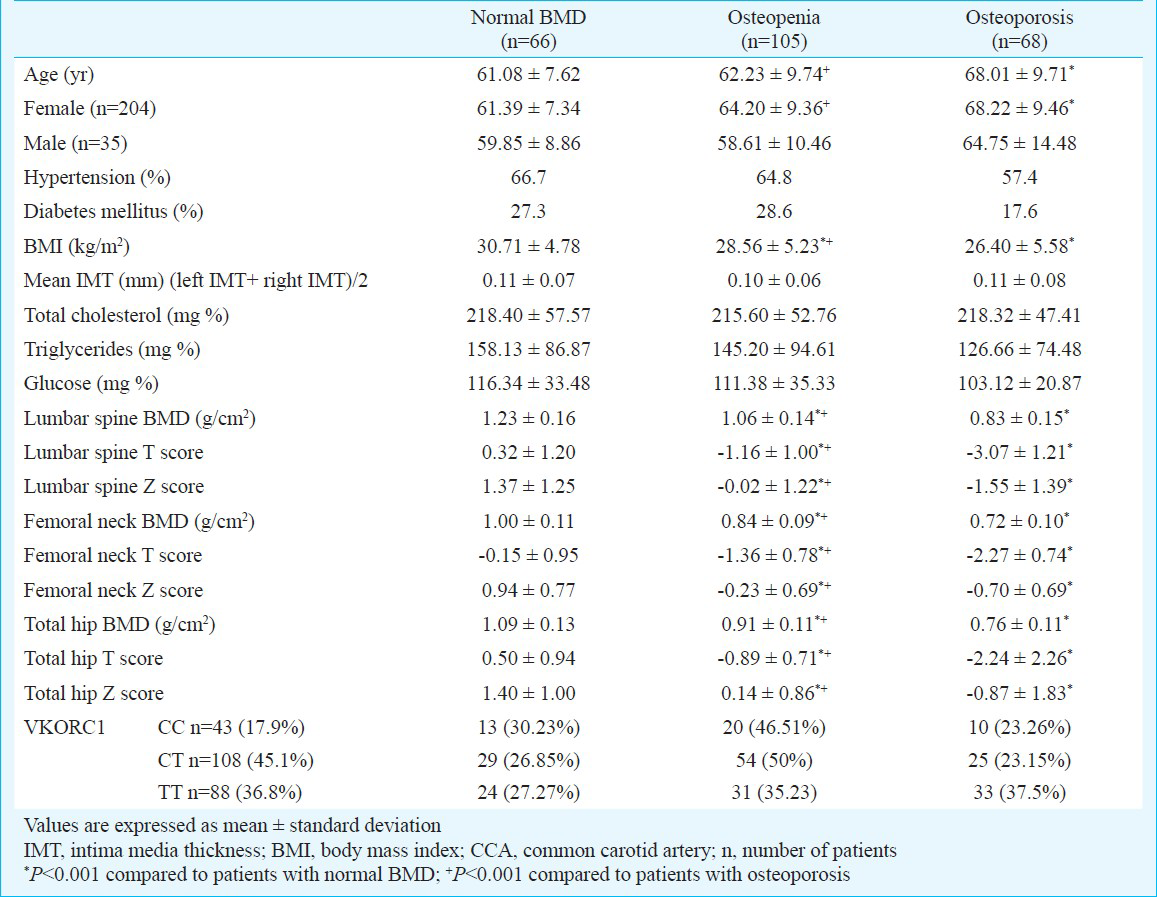
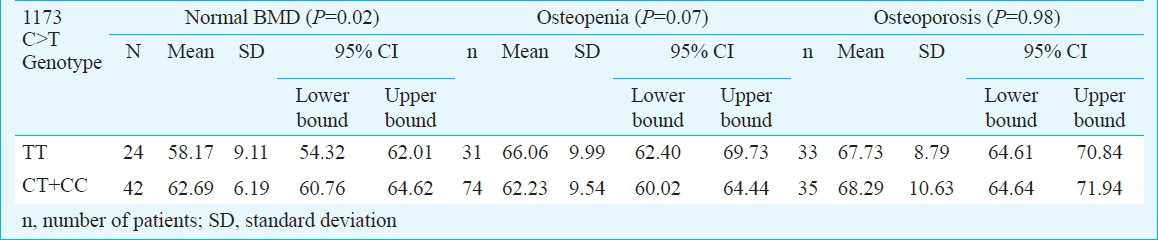
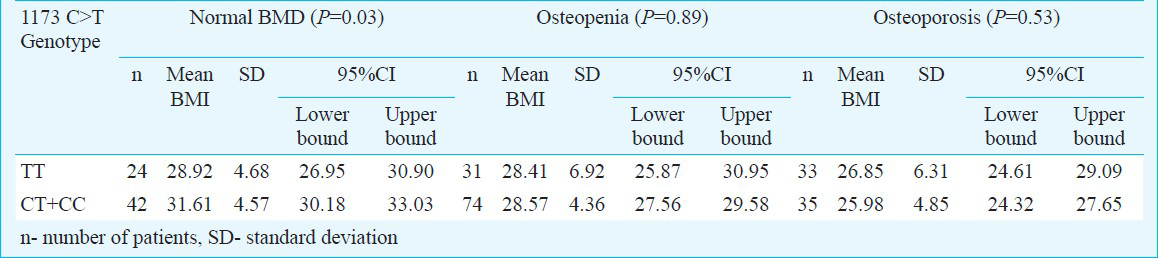
Analyzing the relation between BMD and 1173C>T polymorphism, no significant differences were obtained between normal, osteopenic, and ostoeporotic BMD and TT, CT, or CC genotypes (Table II). No significant statistical differences were found when the comparison was made between TT+CT and CC genotypes (TT+CT: 80.30% normal BMD, 80.95% osteopenic patients, 74.36% osteoporotic patients, P=0.70) but when the comparison was made between CC+CT and TT genotypes, a significance was obtained (CC+CT: 63.64% normal BMD, 70.48% osteopenic patients, 53.03% osteoporotic patients, P=0.04). This came from the significant differences obtained by comparing osteopenic and osteoporotic groups and CC+CT and TT genotypes (CC+CT: 70.48% osteopenic patients, 53.03% osteoporotic patients, P=0.03). The association between osteopenic and osteoporotic groups and CC+CT and TT genotypes was more powerful for the T-score of lumbar spine (P=0.002) than for the T-score of femoral neck (P=0.01). The mean age and mean BMI were lower in the group of patients with TT genotype and normal BMD compared to CC+CT genotype and normal BMD group (P=0.02 and P=0.03, t test) (Tables III and IV).
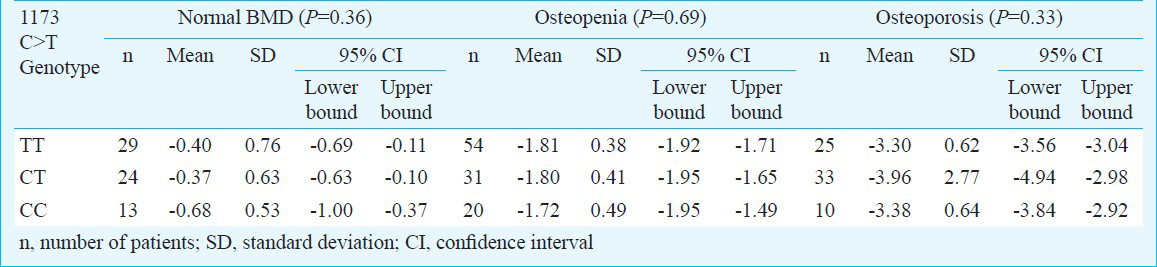
The relationship between IMT and VKORC1 1173C>T genotype did not show any significance when the analysis was made by genotype (Table V), Kruskal-Wallis test) or associations (TT+CT P=0.15, Mann-Whitney test, and CC+CT P=0.22, Mann-Whitney test). As a matter of concern regarding the presence of calcified atherosclerotic plaques, a statistical significance was obtained only to the CC+CT association compared to the TT genotype (P=0.05).

When analyzing the influence of BMD and VKORC1 1173 C>T genotype on mean IMT (two-way ANOVA, dependent variable means IMT), none of the following factors had a significant influence on IMT: VKORC1 P=0.81, BMD P=0.32 or the composed factor VKORC1 - BMD P=0.42.
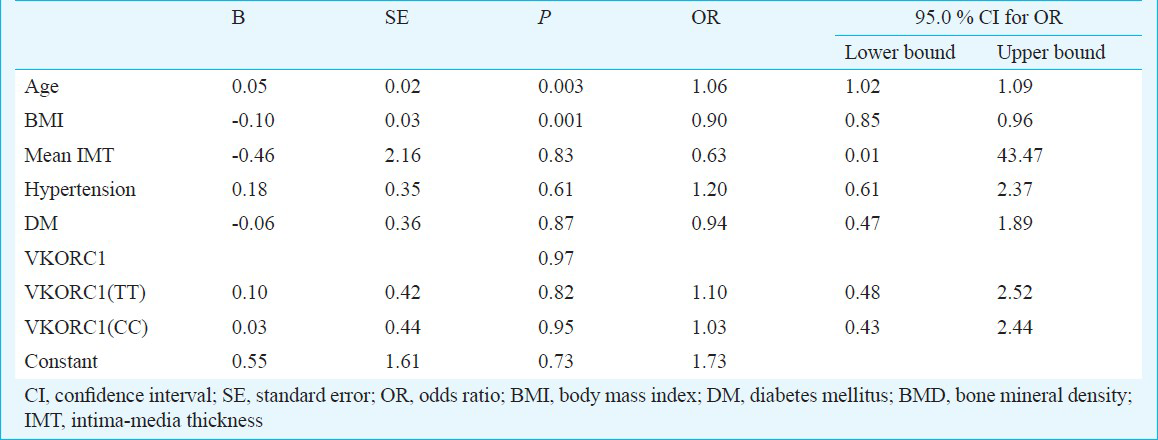
The association between BMD and age, BMI, hypertension, diabetes mellitus, the VKORC1 genotype, mean IMT analyzed with multivariate logistic regression (Enter method) revealed that only age (OR 1.06 95% CI 1.02 to 1.09, P=0.003) and BMI (OR 0.90, 95% CI 0.85 to 0.96, P=0.001) had significant influence on BMD (Table VI).
Discussion
In this cross-sectional study we used a recessive model (TT versus CT or CC genotype for the VKORC1 1173C>T genetic polymorphism) and showed that in patients with osteoporosis and osteopenia there was a more frequent TT genotype of VKORC1 1173C>T. Further, the TT genotype was significantly more frequently found in the osteoporotic group compared to the osteopenic group. For the whole group of patients no correlation could be established between the IMT and VKORC1 1173C>T genotype but, when we analyzed the presence of calcified atherosclerotic plaques, there was a significant association with the TT genotype (P=0.05). This finding was not associated with normal or pathologic BMD.
Teichert et al23 found that the T-allele of the VKORC1 1173C>T polymorphism was associated with a small but significantly increased risk of aortic calcification, explaining this situation by the dominant effect of the T-allele. When they analyzed the presence of 4 to 6 calcified plaques in the carotid artery, no association with the T-allele was found. In our study the aortic calcifications had not been recorded and so a correlation with the carotid calcifications has not been searched for. We took in consideration the presence of calcified plaques in the carotid arteries, regardless of their number. The association of calcified plaques to VKORC1 genotype was established only in the presence of TT genotype suggesting that T allele had a recessive effect.
D’ Andrea et al14 stated that the TT genotype was associated with a less carboxylation of vitamin K-dependent proteins. Osteocalcin and matrix Gla protein, two members of Gla-proteins family for which vitamin K acts as a cofactor for gamma-glutamyl carboxylase (involved in the bone turnover and the prevention of arterial calcification)12, should be, in this condition, at a lower level of carboxylation. The higher prevalence of TT genotype that was found in the osteoporotic group could be explained by this mechanism. Wang et al15 found in subjects with TT genotype a higher level of undercarboxilated osteocalcin but they assumed that the association found between the higher risk of vascular diseases (stroke, coronary heart disease, and aortic dissection) and the C allele of the +2255 locus might not be related to the effect on the gamma-carboxilation of the vitamin K-dependent proteins. Another yet-known function of VKORC1 could be responsible for this association15. Due to the lack of association between all the three variables (VKORC1 genotype, BMD, and IMT/calcified plaques) the hypothesis of different mechanisms of VKORC1 involvement in OP and ATS is suggested by our study: TT genotype influences the BMD via vitamin K-dependent proteins and the presence of calcified plaques via another unknown function. The effects of VKORC1 genetic polymorphism on hepatic expression in patients receiving warfarin had been studied but little is known about expression of the gene in other tissues24. More studies are needed in this direction.
The frequency of VKORC1 1137TT genotype was found to be significantly lower in patients with venous thromboembolism than in matched controls25. It was suggested that the VKORC1 haplotype group A (including the T allele of the VKORC1 1137C>T polymorphism) might be associated with a lesser procoagulant effect25. In these settings, haplotype B carriers (including the C allele of the VKORC1 1137C>T polymorphism) might have an elevated level of vitamin K-dependent proteins and protein C and protein S plasma levels would also expected to be elevated. This hypothesis was not confirmed by the study of Kimura et al26 raising the possibility of different mechanisms involved in this association.
We found an association between age and BMI, TT genotype, and normal BMD. The patients with TT genotype and normal BMD were younger than the other genotypes, suggesting that their BMD had become abnormal earlier and OP had appeared at a younger age. Also, the lower BMI of TT genotype patients compared to other genotypes should be interpreted as a risk factor for developing OP. The positive relation between BMI and OP is well known2728.
One of the limitations of the study was the absence of the data regarding genotype distribution of VKORC1 1173C>T in the Romanian population. The interethnic variability of VKORC1 genotype was demonstrated. The frequency of 1173TT in Asian patients is higher than in Caucasian and African populations2930. The frequency of TT genotype in the Caucasian population was 17 per cent31 and 15.1 per cent24 in the earlier studies compared to 36.8 per cent in our study. In the previously mentioned study, all the subjects were healthy volunteers, unlike the subjects in our study who were consecutively enrolled from patients presenting for BMD measurement. Large populational studies are required to establish the real proportion of VKORC1 genotype in the Romanian population. Another limitation of the study was the low sample size that might be responsible for the lack of statistical power.
In conclusion, VKORC1 polymorphism (TT genotype) was associated with OP and the presence of calcified plaques in the carotid artery. Probably different mechanisms are involved in these associations.
Acknowledgment
Authors acknowledge the ANCS (Romanian National Authority for Scientific Research) 42107/2008 PNII grant, for financial support.
References
- High dietary menaquinone intake is associated with reduced coronary calcification. Atherosclerosis. 2009;203:489-93.
- [Google Scholar]
- Oxidized low density lipoprotein inhibits phosphate signaling and phosphate-induced mineralization in osteoblasts. Involvement of oxidative stress. Biochim Biophys Acta. 2010;1802:1013-9.
- [Google Scholar]
- Metacarpal cortical area and risk of coronary heart disease: the Framingham Study. Am J Epidemiol. 2004;159:589-95.
- [Google Scholar]
- The association between carotid or femoral atherosclerosis and low bone mass in postmenopausal women referred for osteoporosis screening. Does osteoprotegerin play a role? Maturitas. 2010;67:358-62.
- [Google Scholar]
- Relationship between decreased bone mineral density and subclinical atherosclerosis in postmenopausal women. Climacteric. 2010;13:254-8.
- [Google Scholar]
- Low bone mineral density is related to atherosclerosis in postmenopausal Moroccan women. BMC Public Health. 2009;9:388.
- [Google Scholar]
- Lower bone mineral density is associated with higher coronary calcification and coronary plaque burdens by multidetector row coronary computed tomography in pre- and postmenopausal women. Clin Endocrinol (Oxf). 2009;71:644-51.
- [Google Scholar]
- Relationship of calcification of atherosclerotic plaque and arterial stiffness to bone mineral density and osteoprotegerin in postmenopausal women referred for osteoporosis screening. Calcif Tissue Int. 2008;83:112-20.
- [Google Scholar]
- Carotid plaque echogenicity and risk of nonvertebral fractures in women: a longitudinal population-based study. Calcif Tissue Int. 2006;79:207-13.
- [Google Scholar]
- Beyond deficiency: Potential benefits of increased intakes of vitamin K for bone and vascular health. Eur J Nutr. 2004;43:325-35.
- [Google Scholar]
- Identification of the gene for vitamin K epoxide reductase. Nature. 2004;427:541-4.
- [Google Scholar]
- A polymorphism in the VKORC1 gene is associated with an interindividual variability in the dose-anticoagulant effect of warfarin. Blood. 2005;105:645-9.
- [Google Scholar]
- VKORC1 haplotypes are associated with arterial vascular diseases (stroke, coronary heart disease, and aortic dissection) Circulation. 2006;113:1615-21.
- [Google Scholar]
- Vitamin K epoxide reductase (VKORC1) gene mutations in osteoporosis: A pilot study. Transl Res. 2010;156:37-44.
- [Google Scholar]
- VKORC1 deficiency in mice causes early postnatal lethality due to severe bleeding. Thromb Haemost. 2009;101:1044-50.
- [Google Scholar]
- VKORC1 common variation and bone mineral density in the Third National Health and Nutrition Examination Survey. PLoS One. 2010;5:e15088.
- [Google Scholar]
- Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis. Circulation. 2007;115:459-67.
- [Google Scholar]
- WHO Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser. 1994;843:1-129.
- [Google Scholar]
- Apolipoprotein E genotype and warfarin dosing among Caucasians and African Americans. Pharmacogenomics J. 2008;8:53-60.
- [Google Scholar]
- Vitamin K epoxide reductase complex subunit 1 (VKORC1) polymorphism and aortic calcification: the Rotterdam Study. Arterioscler Thromb Vasc Biol. 2008;28:771-6.
- [Google Scholar]
- VKORC1 genetic polymorphism and risk of venous thromboembolism in postmenopausal women: new findings and meta-analysis. J Thromb Haemost. 2009;7:1034-6.
- [Google Scholar]
- Vitamin K epoxide reductase genetic polymorphism is associated with venous thromboembolism: results from the EDITH Study. J Thromb Haemost. 2007;5:2020-4.
- [Google Scholar]
- Polymorphisms in vitamin K-dependent gamma-carboxylation-related genes influence interindividual variability in plasma protein C and protein S activities in the general population. Int J Hematol. 2006;84:387-97.
- [Google Scholar]
- The association between body mass index and osteoporosis in patients referred for a bone mineral density examination. J Womens Health. 2006;9:1028-134.
- [Google Scholar]
- Influence of lean and fat mass on bone mineral density (BMD) in postmenopausal women with osteoporosis. Arch Gerontol Geriatr. 2011;53:237-42.
- [Google Scholar]
- International Warfarin Pharmacogenetics Consortium. Warfarin pharmacogenetics: a single VKORC1 polymorphism is predictive of dose across 3 racial groups. Blood. 2010;115:3827-34.
- [Google Scholar]
- A novel functional VKORC1 promoter polymorphism is associated with inter-individual and inter-ethnic differences in warfarin sensitivity. Hum Mol Genet. 2005;14:1745-51.
- [Google Scholar]
- Cytochrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase (VKORC1) genotypes as determinants of acenocoumarol sensitivity. Blood. 2005;106:135-40.
- [Google Scholar]




