Translate this page into:
Reaching tribal men to improve awareness to sexual morbidities: Experience from Baiga tribe of Central India
Reprint requests: Dr Kalyan B. Saha, Scientist D (Demography), Regional Medical Research Centre for Tribals (ICMR), Nagpur Road, Garha, Jabalpur 482 003, Madhya Pradesh, India e-mail: kalyansaha_icmr@yahoo.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background and objectives:
Tribal men's reluctance in sharing responsibilities as supportive partners in reproductive and sexual health matters debar women from their sexual rights coupled with their negligence in health care and lesser utilization of reproductive health facilities. As a matter of fact a large proportion of ill health particularly related to sexually transmitted infections (STIs) suffered not only by men but also by their spouses. The present study was planned among one of the primitive tribes of Madhya Pradesh to understand the knowledge of males about reproductive tract infection (RTI)/STI/HIV/AIDS, RTI symptoms suffered, perception on sexual health, utilization of health services and to improve the knowledge by intervention of need based IEC (information, education, communication) strategy.
Method:
The study was conducted among 400 currently married men in the age group of 15-40 yr in one of the primitive tribes, Baigas of Dindori district of Madhya Pradesh. Eighteen villages were explored in the study. The IEC intervention was made by using quasi-experimental before and after with control design.
Result:
The baseline data generated indicated that Baigas male were poorly informed about RTI (18%), STI (21.5%) and HIV/AIDS (10%). Further, men also projected misconception on different aspects of sexuality. Women's views recorded also suggested a disturbing trend regarding male involvement in reproductive health particularly related to STIs.
Interpretation & conclusions:
After intervention of IEC targeting male population in age group 15 - 40 yr by adopting a before and after with controls design the awareness was improved significantly. The utilization of the health services was also improved significantly. The study recommends replication of the IEC strategy designed in other Baiga villages for improving the reproductive health of the tribe.
Keywords
Baiga tribe
currently married males
HIV/AIDS
IEC intervention
reproductive tract infections
sexual morbidities
STI

Reproductive morbidity, here designated as reproductive tract infection (RTI) particularly the sexually transmitted infection (STI), has always been a significant public health problem in India. The epidemic of HIV/AIDS has increased the significance of STIs in public health settings, as it increases the risk of HIV infection 2 to 10 folds12. The situation becomes serious as men play an important role in the spread of the infection but a less prominent role in prevention of the same. Lack of knowledge and non availability of male oriented services with quality of care deter men from sharing the responsibility in reproductive health matters3. In a study conducted by Khan et al4, the health workers reported that their activities in the area was hindered by the mass view that men's major responsibility is to provide financially for their families and that childbearing and contraception are women's role. In another study5, it was highlighted that husband and the wives themselves considered reproductive health mainly a “women's affair”. Hence, reproductive health generally has been considered as synonymous with women's health, and reproductive health of men has received little attention. In a society like ours predominated by the males, declining sex ratio for females, increasing number of women with sexually transmitted infection including HIV, increasing unintended pregnancies and induced abortions including unsafe abortions, higher infant mortality rate (IMR), suggest that women bear the brunt and carry the burden of reproductive ill health which can be prevented to a certain extent by active participation of men6. Misinformation regarding male sexuality and limited availability of scientific data contributed men's limited involvement in reproductive health17. There has been no systematic effort to involve men in reproductive health programmes8.
National Population Policy (2000) and Tenth Five Year Plan (2002-2007) have specifically mentioned importance of male involvement in planned parenthood, promotion of male contraceptives and control of STI/RTI910. Some of the studies pertaining to reproductive health such as U.N. Mysore population studies11, Wyon and Gordons12, Reproductive and Child Health Survey- 1998-9913, National Family Health Survey-2 (NFHS-2)14 merit citations as these depict the reproductive health situation in India. But these studies also lack proper information on male's participation in reproductive health issues.
Madhya Pradesh is the hub of tribal concentration in the country as it accommodates more than 20 per cent Scheduled tribes of the country1516. The reproductive health among tribal population of Madhya Pradesh and the extent of actual problem remain unknown. RTI/STIs among tribal men not only jeopardize their own health but also increase sexual morbidities among their spouses. STIs are primarily attributed to high risk sexual behaviour. Multiple sex partners, unsafe sex, etc. are the primary causes of transmission of STI and HIV infection. In order to prevent and control STIs in the tribe, it becomes imperative to sensitize men towards safer sexual behaviour particularly in the active reproductive age group. The present study was, therefore, planned among one of the primitive tribes of Madhya Pradesh with the objective to understand the knowledge of males about RTI/STI/HIV/AIDS, RTI symptoms suffered, perception of sexual health, utilization of health services and to improve the knowledge by intervention of need based Information, Education and Communication (IEC) strategy.
Material & Methods
This study was conducted during 2004 to 2006 in Dindori district of Madhya Pradesh by scientists, research assistants and other staff of Regional Medical Research Centre for Tribals (RMRCT), Jabalpur.
Community under study: The present study was restricted to primitive Baiga tribe of Baiga Chak area of Dindori district of Madhya Pradesh. The Baiga tribe is concentrated mainly in the districts Dindori, Mandla, Shahdol, Balaghat, Rajnandgaon, Bilaspur, Seoni and Jabalpur. Their actual population for undivided Madhya Pradesh as on today is not available. However, based on their population for 1981 Census (2,48,949)17 and 1991 Census (317549)18, it is projected to be 4,68,451 by 2007 and 5,25,648 by 2012. The Baiga chak villages were mainly located at forests. Being forest villages these were located in very remote areas where excess to health care facilities was meager. Information on Baigas exposed to mass media is not available. Further Madhya Pradesh is classified in the list of States which are poor in regular exposure to any mass media14.
Study design: The study was a trial on IEC materials made on reproductive health for currently married males in the age group 15-40 yr in Baiga villages. A quasi-experimental before and after with control design was adopted as shown below in box:

For baseline survey the sample size estimated for experimental group was 200 currently married males (CMM) assuming awareness to family planning among the tribe in MP 59 per cent19, 95% confidence level and design effect of 2. Attempt was made to estimate the sample size independently with prevalence rate of various other indicators of reproductive health. However, sample size estimated with awareness to family planning gave largest minimum sample size, and hence it was considered for the study. Equal number of sample was considered for control group. A total of 400 married males were surveyed in 2004. From the list of Baiga villages provided by Baiga Development Authority, Dindori district, Government of Madhya Pradesh, 18 villages were selected which were dominated (>90%) by Baiga population and were located in three blocks (Bajag, Karanjia and Samnapur) in the district of Dindori in Madhya Pradesh. Keeping in view the distance, nine villages were randomly selected from the blocks Bajag and Samnapur which were closely located for intervention. Control villages were randomly selected mostly from the block Karanjia which was distantly located from the other two blocks.
The ethical clearance for the study protocol was obtained from the ethics committee of RMRCT, Jabalpur. Informed consents were obtained from the respondents both during baseline and end-line survey.
Language used in interviews/IEC activities: Survey queries were made in local Hindi language so as to make it easy for the tribals to understand and respond. The IEC sensitization programme was also conducted in Hindi. Local popular terms for various aspects of reproductive health were identified during the pre-testing of survey instrument and were used both in surveys and during IEC activities. Beside Centre's staff local unemployed youths were also engaged in the study and they were trained and used as IEC activists.
In absence of any authentic population characteristics of the tribe, door-to-door survey was undertaken interviewing only one male from one household. To achieve the sample size of 400 CMM from 18 villages, 22 males were interviewed in a village. For determining the sample size for the end line resurvey the design effect was not considered keeping in view the same villages covered in the study and resource constrain. Hence, in resurvey a sample of 100 CMM each in test (intervention) and control area was interviewed in 2006. In both baseline and endline surveys CMM were randomly interviewed from the study villages.
Survey instrument: A pre-designed interview schedule was developed which contained both close and open ended questions. The schedule was pre-tested and modified before it was finally administered in the field. National Institute of Medical Statistics (ICMR), New Delhi, was also consulted before finalization of the schedule. A few in-depth interviews were also taken among the married women to get their views about male involvement in reproductive health by using a common interview guideline.
Statistical analysis: The data were analyzed using SPSS-10 software (Chicago). Test of significance was attempted and shown with estimates of net intervention effects. Multivariate logistic regression was attempted to give an insight into some of the background correlates of awareness to RTI and STI. Considering the fact that all RTIs are not STIs, the responses were recorded separately. RTI was explained as an infection in the reproductive tract, while for STI, emphasis was given on method of transmission, i.e., whether respondents were aware of infection through sexual activities. No distinction was made to collect information on HIV infection and AIDS as the target population was a backward group and was not in a position to distinguish between HIV and AIDS. Awareness to condom was also sought from the respondents. Utilization for health services due to reproductive health problems by the males or by their wives during one year preceding the survey was recorded. All these variables were treated as outcome variable after intervention.
Information, education and communication (IEC) activities: IEC camps were organized in the intervention villages once in every three weeks. The contents included the routes of transmission, signs and symptoms to identify RTI/STI. HIV and its transmission mechanism was also explained. The myths and misconceptions related to these diseases and their preventive aspects were also explained. The use of condom was specially emphasized. Further, men were motivated for better involvement as supportive partner to their wives in reproductive health. The effort was made to generate a demand for the health services among the needy. Men particularly in the age group 15-40 yr were targeted for sensitization. The sensitization tools included portable microphones to explain the portable EC posters kits specially designed for the purpose. Condoms were distributed free to those who demanded. Male involvement committees (MIC) with 4-5 members (including village headman with other local male members including teachers and Anganwadi worker or ANM who were better aware of their villages) were formed in all the intervention villages to continue with the IEC activities as welfare measure without any monetary exchange or any material gain throughout the year. The committees’ members were motivated, trained and supplied with IEC teaching aids developed by us for its use in the camps. They were provided with condoms for free distribution in the villages. MIC's activities were monitored regularly. The IEC activities were continued from January to December 2005.
Results
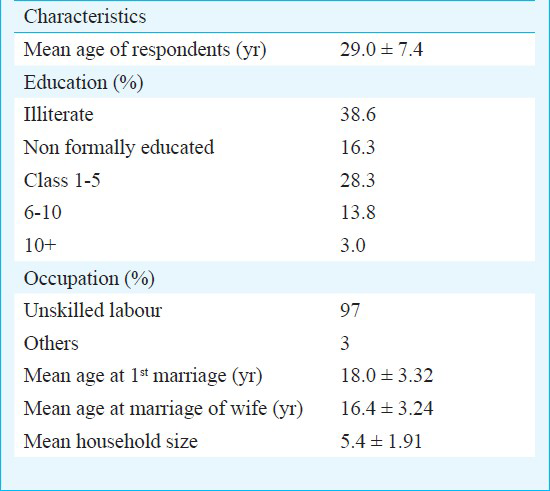
Around 61 per cent of the sample population was literate either non-formally educated or studied up to primary standard. Majority of them were engaged as unskilled labourer. The inter-spouse age difference was found to be narrow (Table I).
Less than a quarter of the sample male was aware of RTI/STI, 18 per cent were aware of RTIs and 21.5 per cent of STIs. Only 10 per cent had heard about HIV/AIDS and most of them had no knowledge of its transmission and prevention. Mean age at 1st intercourse (17.5 ± 3.12 yr) was significantly lower than mean age at first marriage (18.0 ± 3.20 yr) (P<0.001) suggesting prevalence of premarital sex relationship among the tribe. Further extramarital sex relation was also favoured in the tribe.
Results of logistic regression indicated that education (P<0.01) and number of children born (P<0.05) had positive association with awareness to RTI and STI. Other predictors considered in the model were age of the respondents and inter-spouse age difference and knowledge of condom. The dependent variables were awareness to RTI and awareness to STI.
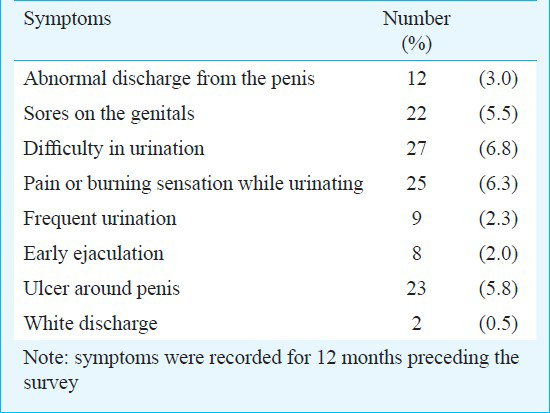
Men reporting symptoms of RTI/STI (Table II): In all 49 (12.3%) males gave multiple responses regarding symptoms suffered, among them 28 (57.1%) reported aware of treatment for such problems. Of these 28 males, 13 availed multiple treatments mostly from traditional healers (8), government doctors (5) and private doctors (3).
Men reported symptoms of RTI/STI (for wives): Some of the respondents reported multiple symptoms suffered by their wives; 34 men reported that their wife either suffered burning sensation/pain/difficulty while urination, 29 reported pain in lower abdomen/vagina during intercourse and 20 reported abnormal vaginal discharge during the last 12 months preceding the survey. Nineteen men extended help to their wives in seeking treatment and mostly from traditional healer. The nature of the symptoms revealed the possibility of existence of syphilis, gonorrhea and herpes simplex among the community.
The in-depth interviews of women indicated the existence of discordance between husband and wife in the Baiga tribe pertaining to seriousness of sexual diseases and importance of treating the same from proper sources. While assessing men's perception about the quality of government health services, only 113 (27%) utilized government health facility for any health problem during the preceding 12 months. Those who did not utilize government health services gave multiple responses for the same (Fig.). Only 248 (62%) men felt the need for reproductive health services and gave multiple responses such as need privacy by (16%), free treatment by (25.3%), at market place (5%), treatment within village by (48%), and need of reproductive health knowledge by (29%). Only one per cent men preferred service from government health posts.

- Reasons for non-utilization of health services.
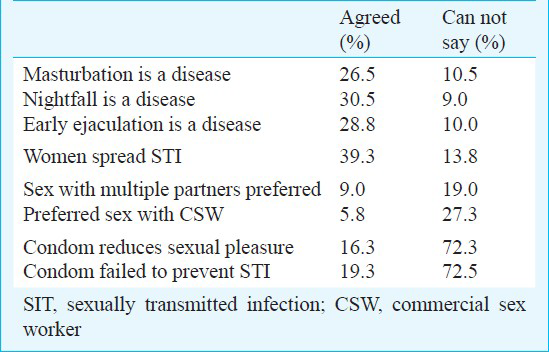
Perception on various aspects of sexuality: Men's attitude towards sexuality and different sexual problems was also recorded during survey (Table III). The data revealed that more than three-fourth of the respondents had a faulty notion about masturbation. Around 10 per cent respondents could not share any ideas. About 40 per cent males felt that women were responsible for the spread of STIs; 16 per cent men felt that condom use reduced the sexual pleasure while 19 per cent believed that it failed to prevent STIs, 72 per cent could not through any light on the efficacy of condom.
There was significant improvement in awareness to RTI in intervention group (47%) compared to control group (19%) (P<0.05), for STI 51 per cent in intervention group compared to 16 per cent in control (P<0.05) and for HIV/AIDS 70 per cent in intervention group compared to 19 per cent in control (P<0.05). Further, IEC could also improve the awareness to condoms significantly (Table IV).
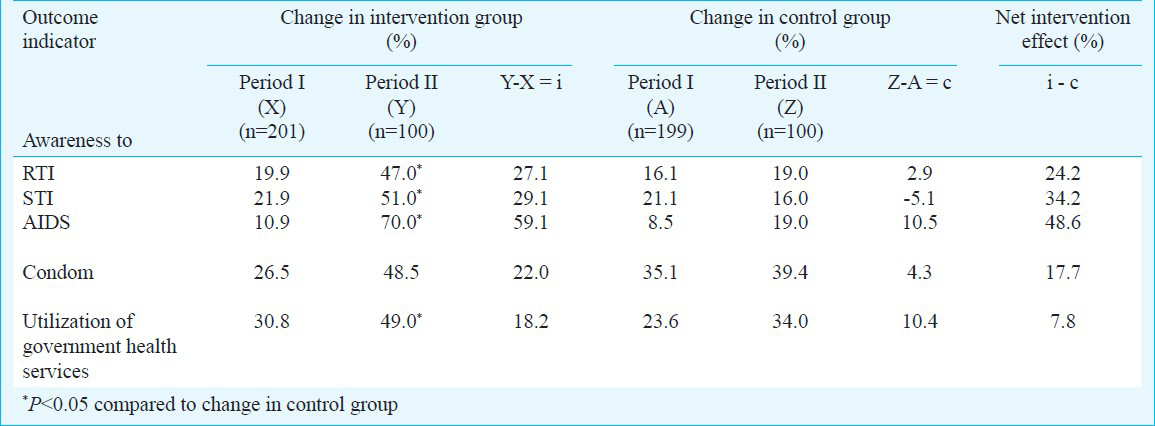
Intervention effect on health utilization (Government services): The utilization of the government health services also improved significantly among the intervention group (49%) compared to control group (34%) (P<0.05) (Table IV).
Discussion
Reproductive tract infections particularly the sexually transmitted infection are a major public health problem and also risk factors for transmission of HIV/AIDS among the tribe. To prevent and control the transmission of STIs and HIV/AIDS, it becomes imperative to understand the level of knowledge, the perception and behavioural dimensions pertaining to RTI/STI/HIV/AIDS among the tribe and secondly, to correct the deficiency by need based suitable gender sensitization programme.
The results of our study indicated that RTI/STI existed among the Baiga tribe as revealed from the reported symptoms. The symptoms were reported in both men and women by men (husbands) and thus there was a chance for under-reporting of the symptoms particularly for the women/wives. The reported symptoms indicated towards the possibility of existence of syphilis, gonorrhoea and herpes simplex among the community, and there is a need for clinical and laboratory based studies including VDRL test for syphilis, culture for gonococci, ELISA for herpes simplex to know the exact magnitude of the prevalence of these infections among the tribe.
The Baiga tribe though resides in remote areas but is not geographically isolated and also due to poverty and occupational compulsion they are exposed to outside people/society. The tribe is also liberal to sex behaviour with a limited number of Baiga men using condom either as a method of family planning or for protecting themselves from RTI/STI; coupled with their poor knowledge of RTI/STI/HIV/AIDS and faulty perception of sexuality attribute them to risk group and is a matter of concern and needs gender sensitization. Further the limited utilization of health services by them aggravates the situation. The IEC strategy for male adopted in the study showed an effect in improving the knowledge and utilization of health services. However, due to limitation of resources the IEC activities could not be extended beyond one year. It is believed that expansion of the same IEC strategy in the Baiga villages particularly those villages not covered in this study is expected to sensitize men towards various aspects of reproductive health. It was observed that local youths got strong role to play in generation of awareness on RTI/STI/HIV/AIDS among the masses. In the present study male involvement committees (MICs) comprising of local tribal youths were formed and they were trained, and motivated to continue with the IEC programme in their villages. Though in the study the views of service providers were not recorded, but effort has been made to look into the utilization and perception of the Baiga male towards the existing government health delivery system. It was observed that government services were not popular among the tribe. On the contrary, Baiga reported its confidence with different private health providers. A large number of unqualified practitioners provide health services to Baigas, consequently they pose a health threat to the group. There is a need to identify such practitioners, contact and provide them information and training on family planning and RTI/STI/HIV/AIDS and they can be used as intermediate behaviour change communicator. It is also suggested to strengthen the health delivery system in PHCs and in the sub centres particularly related to reproductive services in the remote areas and make it more accessible and friendly with the tribe. It is believed that proper gender sensitization, early diagnosis and prompt treatment of STIs will prevent and reduce the burden of RTI/STI among the tribe.
Acknowledgment
The authors acknowledge the Indian Council of Medical Research, New Delhi for financial support. Authors thank Dr Neeru Singh, Director, RMRCT, Jabalpur for providing the facilities, Dr Jyothi Bhat, Scientist D, for her suggestions, Dr D.C. Jain, Technical Assistant (Research) and Shri Shib Kumar Singh, Laboratory Technician at RMRCT, Jabalpur, for technical support. Authors also thank Dr Arvind Verma, Technical Assistant (Research) and Shri Rajdeep Mishra, SRF at RMRCT for help in statistical computations, and Collector and Forest Officials of Chada, Dindori district of Madhya Pradesh, for providing support to the study team during field work.
References
- Community prevalence of sexually transmitted diseases and human immunodeficiency virus infection in Tamil Nadu, India: A probability proportional to size cluster survey. Natl Med J India. 2002;15:135-40.
- [Google Scholar]
- Increased male responsibility and participation: a key to improving the reproductive health. ICMR Bull. 1999;29:59-70.
- [Google Scholar]
- Involving men in reproductive health: policy, action and future challenges from programme perspectives, paper prepared for the workshop on “Enhancing Male Responsibility in Sexual and Reproductive Health” , Kathmandu, Nepal, June 23-26. . 1998;2:14.
- [Google Scholar]
- Young husbands’ involvement 5. in reproductive health in rural Maharashtra. 1998. Men as supportive partners in reproductive sexual health. Narrating experiences. Workshop, Kathmandu, Nepal, June 23-26. Available from: http://www.popline.org/node/283501
- [Google Scholar]
- Enhancing male partnership in sexual and reproductive Health. Mumbai: National Institute of Research in Reproductive Health (ICMR); 2004.
- [Google Scholar]
- Action Research in Community Health and Development (ARCH). Perception of male members about reproductive health matters: preliminary evidence from a tribal area of Gujarat. Men as supportive partners in reproductive and sexual health. Narrating experiences. Workshop, Kathmandu, Nepal, June 23-26 1998. Available from: http:///www.popline.org/node/283509
- [Google Scholar]
- Narrowing the gender gap by enhancing men's involvement in reproductive health. 1998. Men as supportive partners in reproductive and sexual health. Narrating experiences. Workshop, Kathmandu, Nepal, June 23-26. Available from: http://www.popline.org/node/283510
- [Google Scholar]
- Sexual and reproductive health: recent advances, future directions. Vol I. Mumbai: New Age International (P) Limited, Publishers; 2001.
- [Google Scholar]
- Involving men in reproductive health in India: Policies, programs and achievements. J Family Welfare. 2004;50(Special Issue):57-70.
- [Google Scholar]
- Reproductive and Child Health Project: Rapid Household Survey (Phase I and II), 1998-1999. Mumbai: International Institute for Population Sciences;
- [Google Scholar]
- International Institute for Population Sciences, National Family Health Survey (NFHS-2) Madhya Pradesh, (India) and MEASURE DHS+ ORC Macro (USA) 1998-99
- [Google Scholar]
- Census of India 2001. Data Highlights: The Scheduled Tribes, Madhya Pradesh. Available from: http://censusindia.gov.in/Tables_published/SCST/dh_st_madhya_pradesh.pdf
- [Google Scholar]
- Regional Medical Research Centre for Tribals. In: Glimpses of Tribal Health 85th Anniversary. Jabalpur: Indian Council of Medical Research; 1995-96.
- [Google Scholar]
- Ministry of Tribal Affairs, Govt. of India, Annual Report. 2004-2005. :175. Available from: http://www.tribal.nic.in/writereaddata/mainlinkfile/file784.pdf
- [Google Scholar]
- Encyclopedia of primitive tribes in India. Vol I. Delhi: Kalpaz Publication; 2004. p. :25.
- [Google Scholar]
- Male involvement in reproductive health among the scheduled tribes: Experience from Khairwar of Central India. Rural Remote Health. 2007;605:1-5.
- [Google Scholar]




