Translate this page into:
Queyrat erythroplasia accompanied by bladder cancer in a circumcised male
*For correspondence: drsozturk@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 77 year-old male patient presented to the Dermatology clinic, Elazig Education and Research Hospital, Turkey, in November 2010 with complaints of redness and itching his penis. The patient was circumcised at prepubertal period and he underwent radical cystectomy and uretero-ileal loop procedure 10 years ago for bladder cancer. In the dermatologic examination, bright red plaques in the glans penis and also in the coronal sulcus of the circumcised patient with patches of uninvolved skin were observed (Fig. 1). The scar related to the previous operation was observed in the abdominal wall and the outlet of the uretero-ileal loop anatomosis and the connected urine bag (Fig. 2). KOH test was negative, and no growth was observed in the wound culture and fungal culture. In the histopathologic examination of the biopsy material collected from the penile coronal sulcus area, large parakeratotic cells were seen with hyperchromatic nuclei within the thick keratin layer on the surface. Acanthosis of the multi-layer epithelium and elongation of the rete were noted. In addition, there were dyskeratotic cells with large eosinophilic cytoplasms and hyperchromatic nuclei. The histopathologic findings were consistent with Queyrat erythroplasia (EQ) (Figs. 3 and 4).

- Bright red plaques in the glans penis and also in the coronal sulcus of the circumcised patient with patches of uninvolved skin.

- The scar related to the previous operation was observed in the examination of the abdominal wall and the outlet of the uretero-ileal loop anatomosis and the connected urine bag.
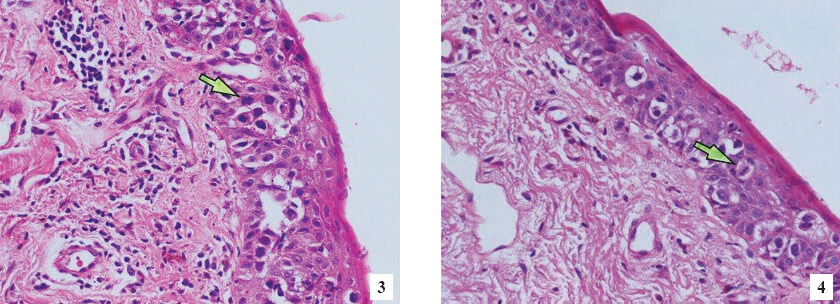
- Histopathology of the biopsy material collected from the penile coronal sulcus area. Large parakeratotic cells with hyperchromatic nuclei (shown by arrow) within the thick keratin layer on the surface. In addition, there were dyskeratotic cells with large eosinophilic cytoplasms and hyperchromatic nuclei. H&E stain at magnification 400x.
EQ can clinically resemble the other benign dermatoses involving the penis1. Histopathologic examination must be performed for differential diagnosis. Differentiation is important in determining the treatment approach and the risk of transformation into invasive carcinoma2. Successful treatment results have been reported with 5-fluorouracil (5-FU), electro-desiccation, curettage, deep fulguration, cryotherapy, radiotherapy, laser, partial or total penectomy, and micro surgery1, as also with imiquimod and photodynamic therapies34. The patient was asked to apply topical 5-fluorouracil cream 5 per cent and dexpanthenol pomade (twice a day).
The patient was followed up in the dermatology unit for about one year, six months later regression of lesions was seen. The patient died of cardiologic problems unrelated to the EQ and bladder cancer.
References
- Diseases and disorders of the male genitalia. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM, Austen KF, eds. Fitzpatrick's dermatology in general medicine (5th ed). New York: McGraw-Hill; 1999. p. :672-4.
- [Google Scholar]
- Erythroplasia of Queyrat with Zoon's balanitis: a diagnostic dilemma. Int J STD AIDS. 2008;19:861-3.
- [Google Scholar]
- Erythroplasia of Queyrat treated with imiquimod 5% cream. J Am Acad Dermatol. 2006;55:901-3.
- [Google Scholar]




