Translate this page into:
Progressive multifocal leucoencephalopathy in HIV/AIDS: Observational study from a tertiary care centre in northern India
Reprint requests: Dr. S.K. Sharma, Head, Department of Medicine, All India Institute of Medical Sciences New Delhi 110 029, India e-mail: sksharma.aiims@gmail.com, sksharma.aiims@yahoo.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Progressive multifocal leucoencephalopathy (PML) is seen mostly in advanced human immunodeficiency virus (HIV) infection. Little is known about the epidemiology and disease course of these patients from India. This study was aimed to determine the frequency of PML in patients with HIV/AIDS, and the clinical features and survival of these patients.
Methods:
The charts of HIV/AIDS patients with PML seen over a period of five years (2006-2011) at the Antiretroviral treatment (ART) centre at a tertiary care centre in New Delhi, India, were retrospectively reviewed.
Results:
Of 1465 patients with HIV/AIDS, 18 (1.2%) were diagnosed with PML; four were laboratory confirmed and 14 had consistent clinical and radiological features. PML was the initial presentation of HIV infection in 10 (56%) patients, and 16 (89%) patients had CD4 count less than 200/μl. Insidious onset focal limb weakness (78%) and visual disturbance (28%) were common symptoms. Magnetic resonance imaging (MRI) of the brain revealed characteristic white matter lesions in all the patients. The estimated median survival was 7.6 months (95% CI, 0-20 months).
Interpretation & conclusions:
Our results show that the patients present late to access treatment with advanced immunosuppression at presentation. PML is associated with high morbidity and mortality despite institution of highly active antiretroviral therapy (HAART). There is a need to address the lacuna in diagnostic and management services for these patients in India.
Keywords
Acquired immunodeficiency syndrome (AIDS)
human immunodeficiency virus (HIV)
JC virus
progressive multifocal leucoencephalopathy (PML)

Progressive multifocal leucoencephalopathy (PML) is a demyelinating disease of the central nervous system (CNS) caused by JC polyomavirus (JCV). After the advent of the HIV epidemic, acquired immunodeficiency syndrome (AIDS) became the most common predisposing disorder for PML1. This disease has been diagnosed in 2-4 per cent of HIV-infected patients in developed countries in the pre-highly active antiretroviral therapy (HAART) era234. The incidence of PML has decreased less dramatically when compared to other CNS diseases in the HAART era56. Interestingly, PML has rarely been reported in HIV-infected patients from developing countries in general, and India in particular78. We sought to study the frequency of PML in patients with HIV/AIDS and the clinical features and survival of these patients at a tertiary care centre in northern India.
Material & Methods
The charts of HIV/AIDS patients with PML seen at the All India Institute of Medical Sciences hospital, New Delhi, over a five year period (July 2006 and June 2011) were retrospectively reviewed. The study included adult patients recruited from the ART (antiretroviral treatment) clinic, various outpatient department or inpatient facility of the hospital. Patients with HIV/AIDS attending various departments/facilities in the hospital are referred to the ART centre. The ART centre works under the aegis of the National AIDS Control Organization (NACO), an initiative of the Ministry of Health and Family Welfare of the Government of India. The hospital provides tertiary care to the population of Delhi and neighbouring States and most of these patients come from the lower socio-economic strata. Ethical clearance was taken from the Institute Ethics Committee.
Clinical diagnosis of PML was suspected when a patient presented with subacute onset of neurological deficits. All patients underwent a thorough clinical evaluation including neurological assessment. These patients underwent computed tomography (CT) scan or magnetic resonance imaging (MRI) of the brain depending upon the appointment for test. The patients with PML were categorized as: histology-confirmed PML (clinical and radiological features consistent with PML associated with histopathological diagnosis); laboratory-confirmed PML (compatible clinical and radiological features associated with the presence of JC virus DNA in cerebrospinal fluid); and possible PML (clinical and radiological findings consistent with PML with exclusion of CNS lymphoma and opportunistic infections like tuberculosis, toxoplasmosis, cryptococcosis)9.
PML was also classified as classic (PML in the setting of severe immunodeficiency) and immune reconstitution inflammatory syndrome (IRIS)-related PML. PML-IRIS was defined as new onset or rapid worsening of PML shortly after initiation of HAART together with evidence of immune restoration (virological and immunological response demonstrated by a decrease in plasma HIV RNA level by more than 1 log10 copies/ml and an increase in CD4+ T cell count from baseline) and clinical symptoms and signs consistent with an infectious or inflammatory process. The symptoms could not be explained by a new infectious process or drug toxicity10.
Most of the patients were hospitalized for detailed assessment, whereas a few patients preferred to follow up at the outpatients facility. Investigations included haematological and biochemical parameters, CD4+ T-cell count and plasma viral load, wherever feasible. HIV infection was documented by a licensed third generation ELISA kit (Detect HIV-1/2, Biochem Immunosystem Inc., Canada, UBI HIV ½ EIA, Beijing United Biomedical Co. Ltd., PR China) as described in the previous study11. CD4+ T-cell count was done using flow-cytometry (Becton Dickinson, USA). Contrast enhanced MRI imaging of the brain was performed in all the patients. Multifocal scalloped white matter lesions were considered characteristic of PML. These lesions are hypointense on T1-weighted sequences and hyperintense on T2-weighted sequences without mass effect or contrast enhancement. Lumbar puncture for CSF analysis was done for JCV detection, wherever facility could be availed and to rule out other disease process.
Detailed clinical examination was repeated every month and recorded as the patients came to the ART clinic for follow up, and collection of antiretroviral drugs in accordance with the guidelines of NACO1213. However, based on the clinical status of the patient, the frequency of follow up was individualized. The HAART regimen consisted of two nucleoside reverse transcriptase inhibitors and one non-nucleoside reverse transcriptase inhibitor. The available drugs included zidovudine, lamivudine, efavirenz and nevirapine. No separate therapy for PML was instituted. During each visit the patients were evaluated for clinical improvement, drug toxicity and development of new opportunistic infections. Adherence (95% of drugs taken) was assessed during each visit by pill count, and patients were motivated by educator cum counselor to adhere to therapy. Medical social workers ensured regular visits of the patients to the ART clinic. Patients were contacted telephonically or their houses were visited in case they failed to turn up for their scheduled visits. Patients who survived were followed up throughout the period and the remaining patients until death or loss to follow up.
Statistical analysis: Continuous data are presented as mean ± standard deviation (for normally distributed variables) or median and interquartile range or IQR (for variable influenced by extreme values). Categorical data are presented as numbers with proportions. Survival distribution was estimated using the Kaplan-Meier method. All analysis was done using SPSS (version 17; SPSS Inc., USA).
Results
Of the 1465 patients registered and followed up in the ART centre during the study period, 18 (1.2%) patients were diagnosed with PML. Fifteen (83%) patients were males. The mean age at diagnosis was 36.9 ± 7.8 yr. Four (22%) were laboratory confirmed and 14 (78%) were possible cases. There were no cases of histology-confirmed PML. In 10 (56%) patients, PML was the first AIDS-defining illness. These patients were put on HAART within one week of the diagnosis. The median time of HAART use in the other eight patients was five months (range: 1-10 months). Important demographic, clinical and laboratory characteristics of the patients are shown in the Table.
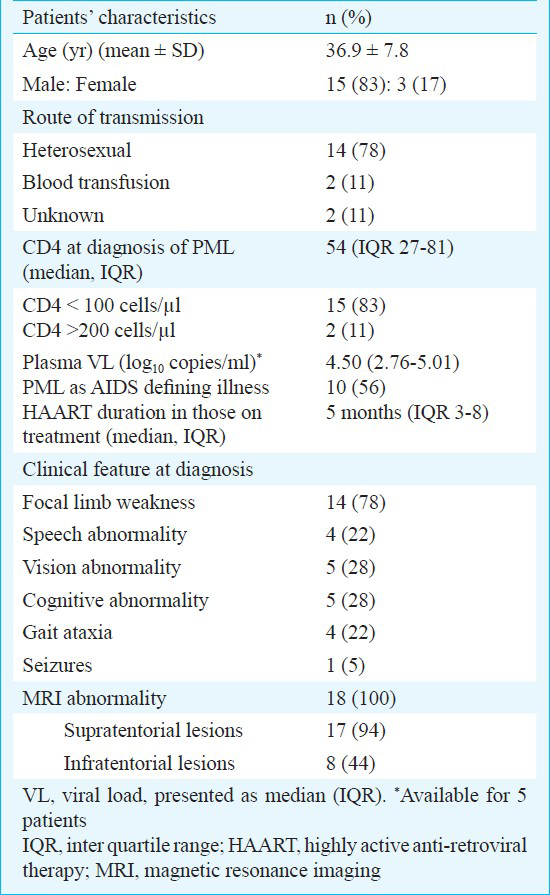
The median CD4 count at the time of PML presentation was 54 cells/μl (IQR 27-81). Sixteen (89%) patients had CD4 count lower than 200 cells/μl and two (11%) patients had count above 200 cells/μl at diagnosis of PML. Clinical features at presentation were variable. Motor deficits with focal limb weakness were the most common presentation seen in 14 patients (78%). Cognitive and behavioural disturbance was seen in five patients (28%), visual abnormality in five (28%), gait ataxia in four (22%) and speech disorders in four patients (22%) at presentation. Only one patient had seizures at the time of diagnosis. CSF analysis was available for 14 patients and showed elevated protein in six patients, pleocytosis in three patients (all mononuclear cells) with normal CSF glucose level in all of them. CSF analysis for JC virus detection was performed in four patients and found to be positive in all of them. Among patients positive for JC virus the viral load was 120000 and 450734 copies/μl (available in 2 patients). Multifocal white matter lesions in cerebral hemispheres were seen in MRI of all patients. These lesions appeared hyperintense on T2-weighted and fluid attenuated inversion recovery (FLAIR) images (Fig. 1), and were not associated with contrast enhancement in all but one patient (paradoxical IRIS). Fourteen (78%) patients presented with classic PML and IRIS-related PML was diagnosed in four (22%) patients; three of them had new onset symptoms after initiation of HAART within six months (unmasked IRIS) and one patient presented with paradoxical worsening of symptoms after initiation of HAART and improvement in immunological status (paradoxical IRIS). The mean time from initiation of HAART to diagnosis of IRIS was 12 wks.
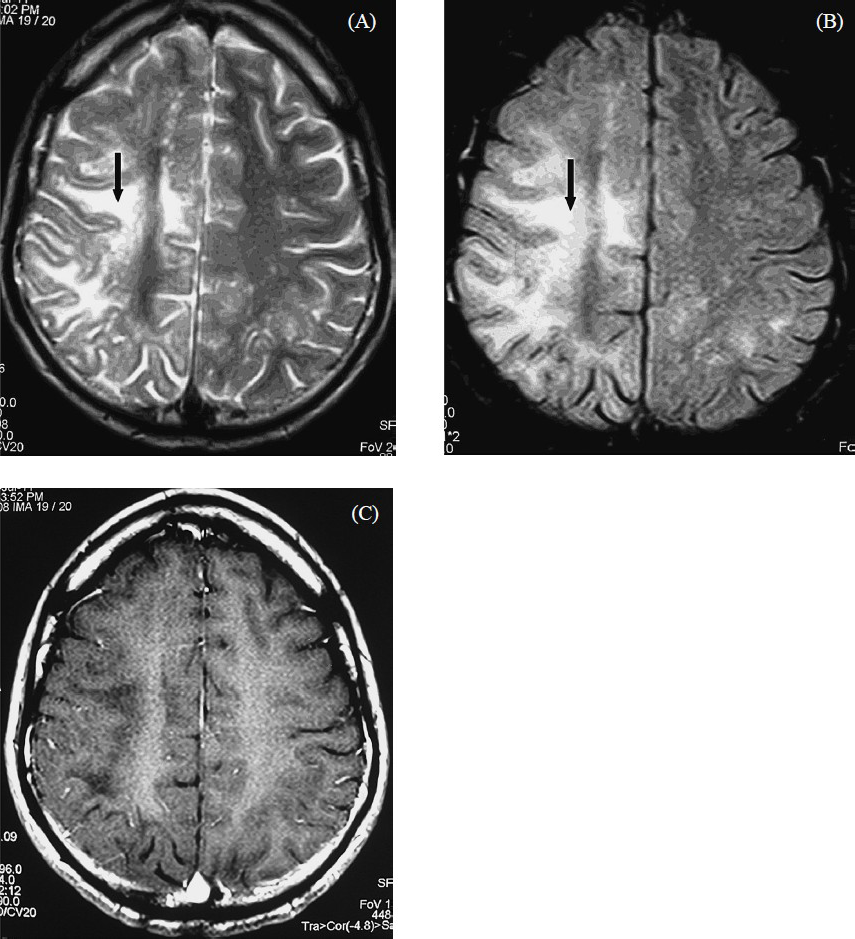
- A 30-year old man presented with insidious onset progressive weakness of left side of the body with visual impairment in the left eye for 6 wk duration. A contrast enhanced MRI brain done for the patient shows scalloped, high signal lesion in the right frontoparietal white matter in the axial T2- weighted fast spin-echo (FSE) image (A) (black arrow). The lesion is better seen on axial FLAIR-FSE image (B) (black arrow). There is no mass effect. No enhancement is seen in the contrast enhanced T1-weighted SE image (C). He was diagnosed to be HIV positive and the PCR for JC virus in the CSF was positive.
During the study period, 11 (61%) patients died, two (11%) were lost to follow up, and five (28%) continued to follow up. The Kaplan-Meier curve depicting the cumulative probability of survival is shown in Fig. 2. The median survival was 7.6 months (95% CI, 0-20 months).
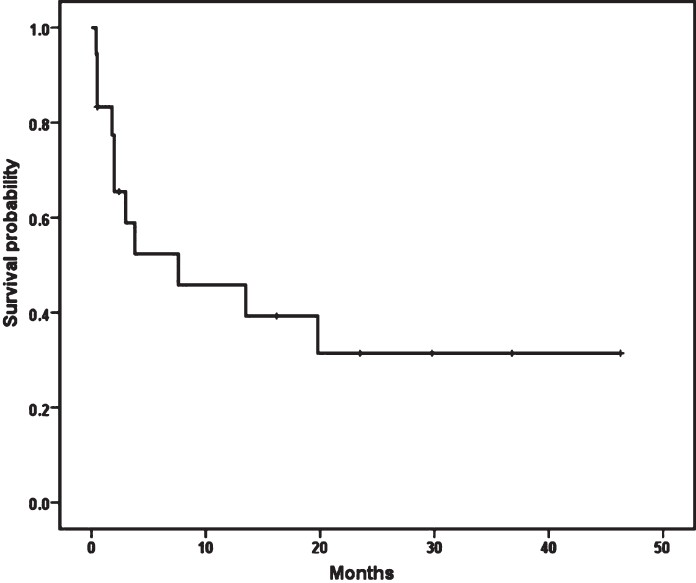
- Survival probability of patients with PML estimated using the Kaplan-Meier method.
Discussion
There is sparse literature on HIV/AIDS with PML from developing countries including India78. In the present study, 1.2 per cent of the patients attending the ART clinic had PML. We had previously described one patient with PML in a series of 135 patients (0.7%)14. It is less common compared to developed countries, where it has been reported in up to 5 per cent of patients15. Literature from India is limited to a small series and case reports. Three cases have been reported from a tertiary care centre in southern India16. Two of the patients died within 45 days of diagnosis, and the third patient was lost to follow up, limiting the data on long-term outcome.
In our study, majority of patients had advanced immunosuppression at the time of diagnosis of PML with 16 (89%) patients having a CD4 count of less than 200 cells/μl. Although PML is usually seen in a setting of advanced immunosuppression, it has also been reported in patients with CD4 counts in excess of 200 cells/μl1718. In 10 of our 18 patients (56%), PML was the first presentation of AIDS. The findings are consistent with that of a recent large retrospective study19. Focal weakness in one of the extremities, cognitive impairment, and visual disturbance were the common manifestations, which is consistent with the findings in the series from developed countries172021. PML-IRIS was diagnosed in 22 per cent of patients in the study, which is in agreement with previous reports in the literature18. While one patient had features of paradoxical IRIS; other three patients were HAART naïve and developed unmasking IRIS. The median survival was 7.6 months which is in agreement with data published in the HAART era1718. In the pre-HAART era, the prognosis of PML was dismal, with a median survival of 2.5-4 months222. Further, the majority of deaths occurred in the initial few months after diagnosis, which is consistent with other studies1821. Various treatment strategies directed against JC virus have been unsuccessful, and HAART remains the only proven effective therapy23. Survival has increased substantially after the introduction of HAART with reported 1-year survival of 39-56 per cent1924252627.
Limited access to diagnostic facilities is a major roadblock to diagnosis of PML, and results in underdiagnosis or underreporting from resource-constrained setting such as India. The limitation of our study arises from the resource constraints which precluded histological proof of diagnosis. Plasma viral load estimation and JC virus detection in CSF could be done only in a limited number of cases due to prohibitory cost of these tests. Most of the cases were in the category of possible PML. However, CSF analysis and relevant investigations were done to rule out other differential diagnosis. The patients were followed up clinically in consultation with a radiologist and imaging repeated if required. MRI was done in all patients as it is more sensitive than CT in early stages of PML.
In conclusion, PML in HIV/AIDS is rare in India. In more than half of the patients PML was the first presentation of AIDS. Advanced immunosuppression was common at diagnosis and the overall outcome poor with a median survival of 7.6 months. Patients not responding to HAART had a rapid course to death with substantial morbidity associated with the progression of neurological deficits. All patients had characteristic findings on MRI brain. Indeed, it should be mandatory to perform a HIV serology in previously healthy individuals who present with neurological deficits and MRI findings characteristic of PML. HIV associated PML is rare in India, and will likely become rarer in the future, if efforts are directed at early initiation of HAART, as recommended by World Health Organization28.
Well planned systematic prospective studies are required in resource-limited settings such as India to fill the yearning knowledge gap in diagnosis and management of these patients. Easy access to diagnostic tests such as viral load estimation, PCR for JC virus detection and confirmatory brain biopsy, wherever feasible, along with increased efforts from the government to ensure wider access to HAART will go a long way to fill the lacunae.
Acknowledgment
Authors thank the National AIDS Control Organization (NACO) and Delhi State AIDS Control Society (DSACS) for providing Integrated Counselling and Testing Centre (ICTC) facility, drugs and other support staff for management of these patients. Authors also thank the All India Institute of Medical Sciences hospital, New Delhi, for providing administrative and other logistic support for the study, and acknowledge support received from the residents, nursing and other staff in the management of these patients.
References
- Progressive multifocal leukoencephalopathy in acquired immunodeficiency syndrome: explaining the high incidence and disproportionate frequency of the illness relative to other immunosuppressive conditions. J Neurovirol. 2003;9:38-41.
- [Google Scholar]
- Progressive multifocal leukoencephalopathy associated with human immunodeficiency virus infection. A review of the literature with a report of sixteen cases. Ann Intern Med. 1987;107:78-87.
- [Google Scholar]
- Neuropathology of acquired immunodeficiency syndrome (AIDS): an autopsy review. J Neuropathol Exp Neurol. 1986;45:635-46.
- [Google Scholar]
- Progressive multifocal leukoencephalopathy: improved survival of human immunodeficiency virus-infected patients in the protease inhibitor era. J Infect Dis. 1999;180:621-5.
- [Google Scholar]
- Changing incidence of central nervous system diseases in the EuroSIDA cohort. Ann Neurol. 2004;55:320-8.
- [Google Scholar]
- The epidemiology of human immunodeficiency virus-associated neurological disease in the era of highly active antiretroviral therapy. J Neurovirol. 2002;8:115-21.
- [Google Scholar]
- Aids-related progressive multifocal leukoencephalopathy: a retrospective study in a referral center in São Paulo, Brazil. Rev Inst Med Trop Sao Paulo. 2008;50:209-12.
- [Google Scholar]
- Neuropathology of HIV/AIDS with an overview of the Indian scene. Indian J Med Res. 2005;121:468-88.
- [Google Scholar]
- The evolving face of human immunodeficiency virus-related progressive multifocal leukoencephalopathy: defining a consensus terminology. J Neurovirol. 2003;9:88-92.
- [Google Scholar]
- HIV seropositivity among adult tuberculosis patients in Delhi. Indian J Chest Dis Allied Sci. 2000;42:157-60.
- [Google Scholar]
- National guidelines for implementation of antiretroviral therapy. New Delhi: NACO; 2004.
- [Google Scholar]
- Outcomes of antiretroviral therapy in a northern Indian urban clinic. Bull World Health Organ. 2010;88:222-6.
- [Google Scholar]
- Spectrum of clinical disease in a series of 135 hospitalised HIV-infected patients from north India. BMC Infect Dis. 2004;4:52.
- [Google Scholar]
- Low prevalence of progressive multifocal leukoencephalopathy in India and Africa: Is there a biological explanation. J Neurovirol. 2003;9:59-67.
- [Google Scholar]
- Clinical epidemiology and survival of progressive multifocal leukoencephalopathy in the era of highly active antiretroviral therapy: data from the Italian Registry Investigative Neuro AIDS (IRINA) J Neurovirol. 2003;9:47-53.
- [Google Scholar]
- Influence of HAART on the clinical course of HIV-1-infected patients with progressive multifocal leukoencephalopathy: results of an observational multicenter study. J Acquir Immune Defic Syndr. 2008;49:26-31.
- [Google Scholar]
- Incidence and outcome of progressive multifocal leukoencephalopathy over 20 years of the Swiss HIV Cohort Study. Clin Infect Dis. 2009;48:1459-66.
- [Google Scholar]
- Progressive multifocal leukoencephalopathy in patients with HIV infection. J Neurovirol. 1998;4:59-68.
- [Google Scholar]
- Incidence, clinical presentation, and outcome of progressive multifocal leukoencephalopathy in HIV-infected patients during the highly active antiretroviral therapy era: a nationwide cohort study. J Infect Dis. 2009;199:77-83.
- [Google Scholar]
- The natural history of progressive multifocal leukoencephalopathy in patients with AIDS. Canadian PML Study Group. Clin Infect Dis. 1995;20:1305-10.
- [Google Scholar]
- Remission of progressive multifocal leucoencephalopathy following highly active antiretroviral therapy in a man with AIDS. Int J Gen Med. 2012;5:331-4.
- [Google Scholar]
- The effect of highly active antiretroviral therapy-induced immune reconstitution on development and outcome of progressive multifocal leukoencephalopathy: study of 43 cases with review of the literature. J Neurovirol. 2003;9:73-80.
- [Google Scholar]
- The effect of potent antiretroviral therapy and JC virus load in cerebrospinal fluid on clinical outcome of patients with AIDS-associated progressive multifocal leukoencephalopathy. J Infect Dis. 2000;182:1077-83.
- [Google Scholar]
- HAART improves prognosis in HIV-associated progressive multifocal leukoencephalopathy. Neurology. 1999;52:623-5.
- [Google Scholar]
- Clinical course and prognostic factors of progressive multifocal leukoencephalopathy in patients treated with highly active antiretroviral therapy. Clin Infect Dis. 2003;36:1047-52.
- [Google Scholar]
- Antiretroviral therapy for HIV infection in adults and adolescents: Recommendations for a public health approach, 2010 revision. Geneva: World Health Organization; 2010.
- [Google Scholar]




