
Translate this page into:
Primary amenorrhoea & virilization induced by pure testosterone-secreting adrenocortical adenoma
*For correspondence: stephensailo@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 20 yr old female† was referred to the department of Urology, North Eastern Indira Gandhi Regional Institute of Health & Medical Sciences, Shillong, India, in October 2016, with complaints of primary amenorrhoea, increased body hair and deepening of voice for five years. Physical examination revealed hirsutism (Figs 1 and 2), underdeveloped breasts, muscle and clitoral hypertrophy. The total serum testosterone was markedly elevated (233 ng/dl). Levels of serum cortisol, luteinizing hormone, follicle-stimulating hormone, estradiol and prolactin and 24 h urinary vanillylmandelic acid were normal.

- Excessive facial hair.

- Excessive abdominal hair.
Abdominal computed tomography detected a 7.5 × 7 × 6.8 cm right adrenal mass (Fig. 3). Open transabdominal adrenalectomy was performed (Fig. 4), and biopsy was reported as a benign adrenocortical adenoma with uncertain malignant potential (Modified Weiss Criteria). Serum testosterone estimated on the 5th post-operative day was normal (38 ng/dl). She began menstruation two months after the operation.

- Contrast-enhanced computed tomography showing well-defined heterodense right adrenal lesion (star).
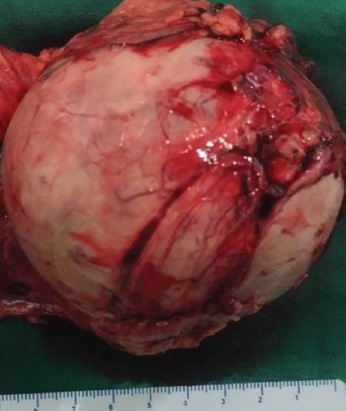
- Well-encapsulated right adrenal tumour.
Pure testosterone-secreting adrenal tumour is rare and should be suspected in the presence of hirsutism, elevated serum testosterone and abdominal mass.
Conflicts of Interest: None.




