Translate this page into:
Prevalence of tuberculosis in Faridabad district, Haryana State, India
Reprint requests: Dr S.K. Sharma, Department of Medicine, All India Institute of Medical Sciences, New Delhi 110 029, India e-mail: sksharma.aiims@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Epidemiological information on tuberculosis (TB) has always been vital for planning control strategies. It has now gained further importance for monitoring the impact of interventions to control the disease. The present study was done to estimate the prevalence of bacillary tuberculosis in the district of Faridabad in Haryana State of India among persons aged older than 15 years.
Methods:
In this cross-sectional study, residents of Faridabad district were assessed for the prevalence of tuberculosis. Twelve rural and 24 urban clusters with estimated populations of 41,106 and 64,827 individuals were selected for the study. Two sputum samples were collected from individuals found eligible for inclusion. The samples were also cultured by modified Petroff's method and were examined for growth of Mycobacterium tuberculosis once a week for eight weeks. A person found positive by smear and/or culture was identified as sputum-positive pulmonary TB positive.
Results:
A total of 105,202 subjects were enumerated in various clusters of the Faridabad district. There were 50,057 (47.58%) females and 55,145 (52.42%) males. Of these 98,599 (93.7%) were examined by the study group (47,976 females; 50,623 males). The overall prevalence of sputum smear or culture positive pulmonary tuberculosis in our study was found to be 101.4 per 100,000 population.
Interpretation & conclusions:
The present results showed that the prevalence of sputum positive pulmonary tuberculosis was higher in Faridabad district than the notification rates recorded by the World Health Organization for the contemporary period, a disparity that could be explained by a difference in case detection strategy employed for the study.
Keywords
Community-based survey
epidemiology
pulmonary tuberculosis
sputum-positive-tuberculosis

Prior to the twentieth century, tuberculosis as a disease was considered to be of little importance to the general population in India. Much more importance was attached to the description of disease in European immigrants as compared to its occurrence in native Indians, a fact that is much different from the situation today. In his notes on the prevalence of tuberculosis in India, Lt Col Wilkinson noted with interest in 1914 that the mention of tuberculosis in Indian literature was scanty due to its low prevalence1. However, he considered the possibility of the disease having been confused with an alternate diagnosis of malaria, which was more prevalent. Wilkinson documented a rise in the incidence of tuberculosis in India and also the mortality associated with it. While several studies during the last century have improved our understanding of the disease, yet the literature on tuberculosis in India leaves much to be desired.
Epidemiological information on tuberculosis has always been vital for planning control strategies, and has now gained further importance for monitoring the impact of interventions against the disease. There are only a few reports on the magnitude of tuberculosis from population based surveys, but most data come from health institution based case notifications in selected subsets and often lack completeness and consistency234567. In view of low health service coverage, a developing diagnostic network, and a weak disease notification system, it is not only difficult to determine the magnitude of tuberculosis from case notification alone, but it is also impossible to monitor the effectiveness of control measures. The targets for tuberculosis control framed within the United Nations’ Millennium Development Goals include reduction of the prevalence and mortality associated with the disease in 1990 to by 50 per cent by 2015. While monitoring control, the aim is to assess the incidence of tuberculosis accurately through routine surveillance. Prevalence surveys give an unbiased measure of burden and are justified in high burden countries where many cases may be otherwise missed89.
A survey conducted in 2003 indicated the presence of as many as 1.5 million infective cases of tuberculosis in the community10. Further, with 1.6-2.4 million incident cases in 2008, India was ranked first in terms of the total number of incident cases of tuberculosis in 200811. Tuberculosis is responsible for as many as 29 deaths per year per 100,000 people. In a country with over a billion people this translates to as many as 290,000 deaths in a year12. With a reported prevalence of 283 cases per 100,000 population, India is among the 22 high burden countries for tuberculosis in the world13. Different studies across the country have estimated a prevalence of smear-positive pulmonary tuberculosis between 60 and 760 per 100,000 population, culture positive tuberculosis between 170 and 980, and culture and/or smear positive prevalence between 180 and 1270 per 100,000 people9.
The present study was done to estimate the prevalence of bacillary tuberculosis in Faridabad district in Haryana, India, among persons aged older than 15 yr.
Material & Methods
The Faridabad district has a population of 2,194,586 people, growing at a rate of 48.47 per cent as recorded over the last decade, with a sex ratio of 839 females per 1000 males14. More than half (56%) of the people reside in the urban areas and almost a third are illiterate. The Revised National Tuberculosis Programme was adopted in Faridabad district in April 200015. Currently, there are four treatment units in the district at Ballabgarh, Palwal, Hodal and Faridabad city besides the 21 designated microscopy centers. In this cross-sectional study, residents of Faridabad district were assessed for the prevalence of tuberculosis. The rural and urban clusters were sampled separately proportional to their size.
Training of staff: The research staff recruited for the study was trained at Tuberculosis Research Center (now National Institute of Tuberculosis Research) in Chennai, for four weeks in November 2007. The field staff was trained for door-to-door census, elicitation of symptoms, sputum collection and reporting. The laboratory technicians were trained for sputum microscopic examination, use of fluorescent microscope and culture processing. Further, the research team was also trained to use ‘TPT 69’ card.
Before initiating field work, cooperation and support was obtained from the district health officials, and medical officers of various tuberculosis units and centers. In addition, local community leaders were contacted and sensitized towards the study. Cluster mapping was undertaken with their help.
Subject selection and data collection: The current recommended strategy for identification of cases of pulmonary tuberculosis is one of passive case finding among patients with respiratory symptoms who present spontaneously to health care facilities. Symptoms such as cough for two weeks or more is used to guide examination of sputum for tuberculosis detection. In a cross-sectional house-to-house survey over 15 months between January 2008 and March 2009, all individuals over 15 years were registered and screened by enquiring for previously defined symptoms suggestive of tuberculosis vis-à-vis cough, fever, chest pain and previous history of tuberculosis. The district was taken as the sampling universe and stratified cluster sampling was undertaken. Rural and urban clusters were sampled separately. The rural cluster was a village while an urban cluster was defined as an area which covered two contiguous polling booths. Rural and urban clusters were sampled separately so that the rural-urban distribution in the sample was similar to the rural-urban distribution of the population in the district. Clusters in urban and rural areas were selected systematically from the entire list of such clusters in the district and arranged in ascending order of the population. The sampling was proportional to size. The entire eligible population in the selected cluster was covered.
Individuals were classified as symptomatics if they had cough for over two weeks; or chest pain or fever for over one month; or haemoptysis on any occasion over six months preceding the interview. They were labelled asymptomatic but eligible if they had previously received anti-tubercular treatment on any occasion. It was estimated that 60 per cent of cases would be picked up by eliciting their symptoms and thus the prevalence was estimated at 2.4 per 1000 population. To achieve a precision of 20 per cent with 95 % confidence intervals presuming a minimum coverage of 90 per cent with a design effect of 2, the sample size required was calculated to be 90,000 individuals older than 15 yr. Twelve rural and 24 urban clusters with estimated populations of 41,106 and 64,827 individuals were selected for the study.
Two sputum samples were collected, one was taken on spot and the second was obtained next morning from all eligible subjects. The sputum samples were collected in sterile, single-use disposable containers and were transported to the central laboratory at the All India Institute of Medical Sciences, New Delhi on the same day in ice-packs for storage. The samples collected were examined by direct smear microscopy and subjects were identified as smear positive cases of tuberculosis if at least one sputum sample was found positive for acid-fast bacilli (AFB). These were processed by modified Petroff's method16 and examined under fluorescence microscopy. The sputum was cultured on Lowenstein-Jensen medium and examined for growth of Mycobacterium tuberculosis once a week for eight weeks. A person found positive by smear and/or culture was identified as a sputum-positive pulmonary tuberculosis case. All subjects identified as cases, were treated with Directly Observed Treatment Short-course (DOTS) under the Revised National Tuberculosis Control Programme (RNTCP). Subjects were excluded if no sputum could be obtained despite efforts at induction.
The study protocol was approved by the ethics committee of the All India Institute of Medical Sciences, New Delhi. All participants were included only after they gave written and informed consent.
Quality control: A random sample of study participants screened for symptoms by field workers was screened independently by an independent supervisor on day-to-day basis; 10 per cent of the individuals included in the study were reviewed by the supervisors who stayed in the field with investigators and interviewed the participants. The extent of agreement was reviewed between the two regularly during the course of the survey. Excellent concordance was reported by the supervisors in their survey. Sputum examination and culture were subjected to quality assurance protocols as per the guidelines under the Revised National Tuberculosis Control Programme. Five positive and five negative slides were re-examined by systematic random method and a feedback on quality of smear, stain, reading and reporting was given. The extent of agreement was ascertained and found to be excellent. The progress of the project was periodically reviewed by a team of experts including members from WHO, Geneva constituted by the Central TB Dvision of the Ministry of Health and Family Welfare, Government of India.
Statistical analysis: The results were analyzed using SPSS version 11.0 (SPSS Inc, Chicago, IL, USA). The outcome variable was the diagnosis of tuberculosis and the proportion of cases of tuberculosis among all included subjects was calculated. The prevalence of sputum and/or culture positive cases was calculated using appropriate formulae. The differences in proportions were analyzed for significance using the chi-square test.
Results
A total of 105,202 subjects were enumerated in various clusters of the Faridabad district. There were 50,057 (47.58%) females and 55,145 (52.42%) males; 61,368 (58.33%) were from the urban clusters while 43,834 (41.67%) were from the rural clusters. Of these, 98,599 (93.7%); (50,623 men and 47,976 women; 41,261 rural and 57,338 urban) were examined by the study group. A flowchart detailing the conduct of the study is presented in the Figure.
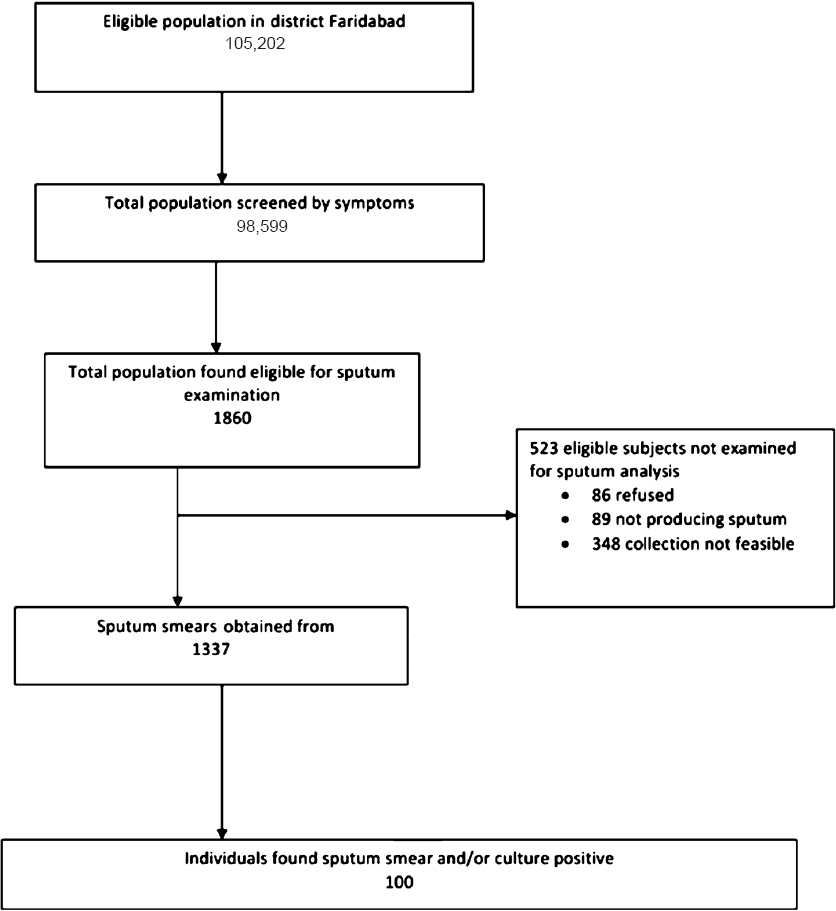
- Flowchart depicting the study design.
Among those found eligible for participation (n=1860), 221 (11.9%) subjects complained of cough for two to four weeks; 258 (14%) had cough for one month to less than two months; 122 (6.6%) had cough for two to three months; 154 (8.3%) had cough for three months to less than six months; while 576 (31%) had cough for more than six months duration. While evaluating chest pain it was found that 105 (5.6%) subjects had chest pain for over one to two months; 52 (2.8%) for two to three months; 75 (4%) for three to six months; while 156 (8.4%) subjects had chest pain for over six months. Further, 41 (2.2%) subjects had fever for one to two months; 18 (1%) since two to three months; 15 (0.8%) since three to six months; while 46 (2.5%) subjects were febrile for over six months. A total of 167 (9%) participants had haemoptysis over the previous six months and 786 (42.3%) subjects received anti-tuberculosis treatment in the past.
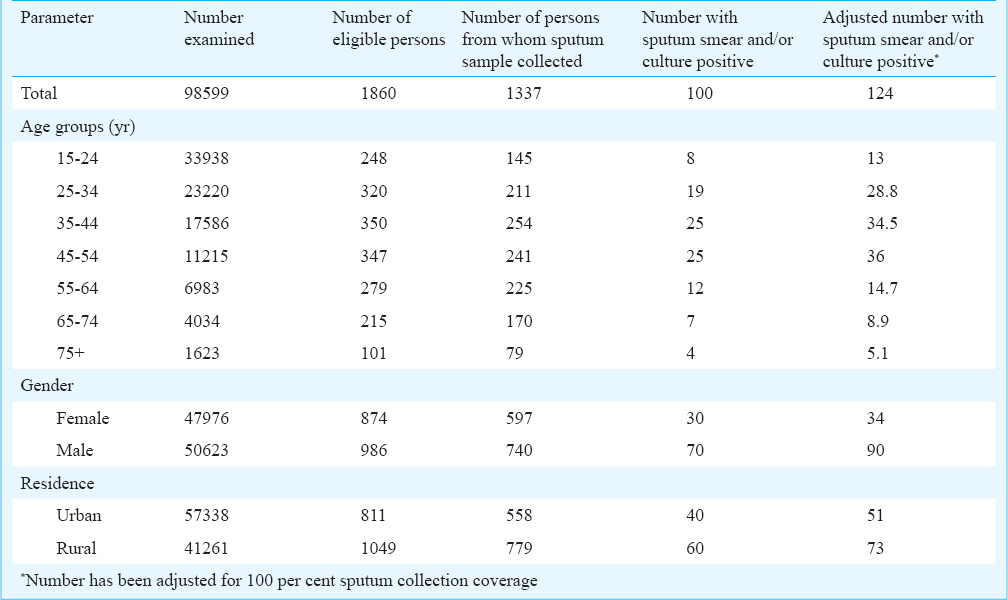
Of the 1860 individuals found eligible for sputum examination, two samples could be examined for 1362 (73.2%) subjects and at least one was examined for 1337 (71.9%) subjects. Sputum could not be examined from individuals who either refused (86, 4.6%), could not produce (89, 4.8%) or collection was not feasible (348, 18.7%). A total of 81 (4.4%) sputum samples were found smear positive while 82 (4.4%) were culture positive. Sixty three (3.4%) subjects were both smear and culture positive, while 19 were smear negative but culture positive and 18 (1%) were only smear positive for AFB. Of the total eligible population (105,202) in the district, 100 were found either smear or culture positive during the study. The overall prevalence of sputum smear or culture positive pulmonary tuberculosis in our study was found to be 101.4 per 100,000 population. The distribution of the examined subjects, results of the sputum examination and the calculated prevalence among the subjects is presented in the Table.
Discussion
A total of 105,202 individuals in urban and semi-urban sectors of Faridabad were included in the current cross-sectional house-to-house survey between January 2008 and March 2009, and the adjusted prevalence of smear positive pulmonary tuberculosis was found to be 101.4 per 100,000 population.
The prevalence of tuberculosis in India was first studied comprehensively in 150 villages, six cities and 30 towns in India in nearly 300,000 subjects aged more than five years by Chakraborty et al in 1950 and it was found that the disease was more prevalent in the rural areas with an overall prevalence of 400 per 100,000 population17. Several surveys have been done in subsequent decades for the estimation of tuberculosis in Tumkur18, Madanapalli19, Bengaluru, Car Nicobar20, Chingleput21, Delhi22, Raichur23, North Arcot24, Wardha25, Morena26, Chhindwara27 and Jammu28. The prevalence of tuberculosis has shown little change over the years as revealed by serial surveys91821.
The World Health Organization (WHO) has recorded a prevalence of 283 cases per 100,000 population of all forms of tuberculosis in India in its report published in 200913. In the same report a notification rate of 51 new sputum smear positive cases per 100,000 population/year has been reported. Our prevalence of 101.4 sputum smear positive cases per 100,000 population appears to be higher than the notification rate as reported by the WHO but this discrepancy may easily be due to the difference in the passive approach to case notification as compared to a more active case detection employed during the current study settings.
Individual studies across India have estimated a prevalence of smear-positive pulmonary tuberculosis between 60 and 760 per 100,000 population9. Authors have shown the association of occurrence of tuberculosis to several determinants including use of biomass fuels29, age, sex, initial tuberculin sensitivity30 and lower socio-economic index31. Narang et al25 studied a total of 114,266 individuals over five years of age in the tribal and non-tribal population in Ashti and Karanja districts of Wardha, Maharashtra in India in a cross-sectional house-to-house survey. They found that the prevalence of tuberculosis was highest in males over 55 years of age. The authors found a total of 148 sputum positive cases of tuberculosis. Of these, 55 were positive on both microscopy and culture while 65 were detected positive on culture alone. They found a prevalence of 142 smear positive cases per 100,000 population in the total population which is higher than our estimate. In another study, Chakma et al26 have reported a prevalence of 12.7 per 100,000 population of Morena district of Madhya Pradesh. In a recently concluded study, Rao et al27 estimated the overall prevalence of pulmonary sputum positive tuberculosis among the Bharia tribal population in Patalkot valley of Chhindwara district of Madhya Pradesh at 432 per 100,000 population. They found that the prevalence increased significantly in those over 45 yr of age27. Ray and Abel24 while studying four villages in the KV Kuppam Block of North Arcot Ambedkar district of Tamil Nadu, south India, covered the entire population of 22,847 people aged older than 10 yr in the area and estimated a prevalence of 241 per 100,000. Gopi et al3233 have found that the prevalence of smear positive TB was 323 per 100,000 and that of culture positive TB was 605 in Tiruvallur district in south India. Data available from Delhi and neighbouring areas indicated that the prevalence of tuberculosis in the region was 330 per 100,000 population in 199122. However, this estimate represents an era prior to the implementation of DOTS in the region and the statistics are likely to have changed with the implementation of RNTCP. A decline in prevalence has previously been noted in this district of Tiruvallur following the implementation of DOTS approach under the RNTCP over five years and the prevalence in the same population has been reported to be 169 smear positive cases per 100,00034 in 2008.
In the neighbouring countries in an earlier study Alvi et al35 have reported a prevalence of 554 smear positive cases detected from examination of a single spot sputum sample in a population of 100,000 while studying 1077 people in Shimshal Valley in Pakistan. They found a prevalence of 1949 cases of smear negative active tuberculosis diagnosed on chest radiography in the same region. Hussain et al6 from the same region reported a high prevalence of latent tuberculosis detected by tuberculin skin test in institutional setting from the North West Frontier Province in Pakistan. Similar studies have been conducted in other developing countries to estimate the burden of pulmonary tuberculosis. Shargie et al36 studied a population of 28,464 in Lemo district of Ethiopia and estimated a prevalence of 78 per 100,000 people in the area in 2003. They showed that the patients detected through their study were younger and ill for longer duration than those who were already on treatment. They also showed that for every two patients on treatment, there was one case of infective tuberculosis in the community who remained untreated and was diagnosed due to the survey.
The major strength of the current study was that it was one of the largest community based Indian studies to determine the prevalence of tuberculosis after the initiation of the Revised National Tuberculosis Control Programme with door-to-door survey and collection of data supported by sputum smears and cultures. It would have been desirable to have 100 per cent sputum collection from the 1860 subjects identified eligible for sputum examination but this was not possible due to operational difficulties and no sputum samples could be collected for 498 participants while only one sample could be examined for 25 participants. It would be interesting to consider how it would have affected our results had the study achieved an ideal one hundred per cent coverage within the study subjects. Considering similar positivity rates among the eligible subjects whose sputum could not be examined, our results might slightly underestimate the actual prevalence of tuberculosis in the community. While it would have been further desirable to support the diagnosis with radiographic evidence in the form of an X-ray of chest, this was beyond the scope of the current study.
In conclusion, the present study estimated the prevalence of sputum smear positive pulmonary tuberculosis to be 101.4 per 100,000 individuals in Faridabad district in Haryana. This compares favourably to the recorded national prevalence rate of 283 per 100,000 population and a case notification rate of 51 new sputum smear positive cases per 100,000 population per year13. Special efforts may be needed to identify individual pockets of higher prevalence of disease and address them specifically while planning and designing control programmes.
Acknowledgment
Authors acknowledge the role of the project staff during the conduct of this study for their invaluable help during the identification of cases and collection of data. The research project was funded by the National Operational Research Committee of the Central TB Division (CTD), Ministry of Health & Family Welfare, Government of India.
References
- The high incidence of tuberculosis among renal transplant recipients in India. Transplantation. 1996;61:211-5.
- [Google Scholar]
- Increasing incidence of fluoroquinolone-resistant Mycobacterium tuberculosis in Mumbai, India. Int J Tuberc Lung Dis. 2009;13:79-83.
- [Google Scholar]
- Incidence, etiopathogenesis and pathological aspects of genitourinary tuberculosis in India: A journey revisited. Indian J Urol. 2008;24:356-61.
- [Google Scholar]
- Postpartum tuberculosis incidence and mortality among HIV-infected women and their infants in Pune, India, 2002-2005. Clin Infect Dis. 2007;45:241-9.
- [Google Scholar]
- Prevalence of and risk factors associated with Mycobacterium tuberculosis infection in prisoners, North West Frontier Province, Pakistan. Int J Epidemiol. 2003;32:794-9.
- [Google Scholar]
- Post-HAART tuberculosis in adults and adolescents with HIV in India: incidence, clinical and immunological profile. Indian J Tuber. 2009;56:69-76.
- [Google Scholar]
- Measuring tuberculosis burden, trends, and the impact of control programmes. Lancet J Infect Dis. 2008;8:233-43.
- [Google Scholar]
- Tuberculosis epidemiology in India: a review. Int J Tuberc Lung Dis. 2005;9:1072-82.
- [Google Scholar]
- Epidemiological situation of tuberculosis in India. Indian Med Assoc. 2003;101:144-7.
- [Google Scholar]
- Global Tuberculosis Control. A short update to the 2009 report. World Health Organzation 2009. available from: http://whqlibdoc.who.int/publications/2009/9789241598866_eng.pdf
- [Google Scholar]
- Census of India. Office of the Registrar General and Census Commissioner, India, 2001. Available from: http://www.censusindia.gov.in/Census_Data_2001/India_at_glance/popu1.aspx
- [Google Scholar]
- Country Profile - India. World Health Organization, 2009. Available from: http://www.who.int/tb/publications/global_report/2009/pdf/ind.pdf
- [Google Scholar]
- Census of India. Office of the Registrar General and Census Commissioner, India. 2001. Available from: http://www.censusindia.gov.in/Census_Data_2001/India_at_glance/popu1.aspx
- [Google Scholar]
- Anti-TB programme in entire State of Haryana from November. The Tribune 2003 October 12
- [Google Scholar]
- Prevalence and incidence of tuberculosis infection and disease in India: a comprehensive review. WHO/TB/97. Geneva: World Health Organization; 1997. p. :1-26.
- [Google Scholar]
- Prevalence of tuberculosis in a south Indian district twelve years after initial survey. Indian J Tuberc. 1979;26:121-35.
- [Google Scholar]
- A controlled study of the effect of a domiciliary tuberculosis chemotherapy programme in a rural community in south India. Indian J Med Res. 1981;73:1-80.
- [Google Scholar]
- Tuberculosis situation among tribal population of Car Nicobar, India, 15 years after intensive tuberculosis control project and implementation of a national tuberculosis programme. Bull World Health Organ. 2004;82:836-43.
- [Google Scholar]
- Trends in the prevalence and incidence of tuberculosis in south India. Int J Tuberc Lung Dis. 2001;5:142-57.
- [Google Scholar]
- New Delhi TB Center. Study of epidemiology of tuberculosis in an urban population of Delhi-report on 30 year follow up. Indian J Tuberc. 1999;46:113-24.
- [Google Scholar]
- A tuberculosis prevalence survey based on symptoms questioning and sputum examination. Indian J Tuberc. 1997;44:171-80.
- [Google Scholar]
- Incidence of smear-positive pulmonary tuberculosis from 1981-83 in a rural area under an active health care programme in south India. Tuber Lung Dis. 1995;76:190-5.
- [Google Scholar]
- Prevalence of sputum-positive pulmonary tuberculosis in tribal and non-tribal populations of the Ashti and Karanja tahsils in Wardha district, Maharashtra State, India. Int J Tuberc Lung Dis. 1999;3:478-82.
- [Google Scholar]
- Survey of pulmonary tuberculosis in primitive tribe of Madhya Pradesh. Indian J Tuberc. 1996;43:85-9.
- [Google Scholar]
- Prevalence of pulmonary tuberculosis among the Bharia, a primitive tribe of Madhya Pradesh, central India. Int J Tuberc Lung Dis. 2010;14:368-70.
- [Google Scholar]
- Tuberculosis prevalence survey in Kashmir valley. Indian J Med Res. 1984;80:129-40.
- [Google Scholar]
- Biomass cooking fuels and prevalence of tuberculosis in India. Int J Infect Dis. 1999;3:119-29.
- [Google Scholar]
- Association of initial tuberculin sensitivity, age and sex with the incidence of tuberculosis in south India: a 15-year follow-up. Int J Tuberc Lung Dis. 2003;7:1083-91.
- [Google Scholar]
- The prevalence of tuberculosis in different economic strata: a community survey from South India. Int J Tuberc Lung Dis. 2007;11:1042-5.
- [Google Scholar]
- A baseline survey of the prevalence of tuberculosis in a community in south India at the commencement of a DOTS programme. Int J Tuberc Lung Dis. 2003;7:1154-62.
- [Google Scholar]
- Relationship of ARTI to incidence and prevalence of tuberculosis in a district of south India. Int J Tuberc Lung Dis. 2006;10:115-7.
- [Google Scholar]
- Rapid decline in prevalence of pulmonary tuberculosis after DOTS implementation in a rural area of South India. Int J Tuberc Lung Dis. 2008;12:916-20.
- [Google Scholar]
- Prevalence of pulmonary tuberculosis on the roof of the world. Int J Tuberc Lung Dis. 1998;2:909-13.
- [Google Scholar]
- Prevalence of smear-positive pulmonary tuberculosis in a rural district of Ethiopia. Int J Tuberc Lung Dis. 2006;10:87-92.
- [Google Scholar]




