Translate this page into:
Prevalence of Rh, Duffy, Kell, Kidd & MNSs blood group antigens in the Indian blood donor population
Reprint requests: Dr R.N. Makroo, Director, Department of Transfusion Medicine, Indraprastha Apollo Hospital, Sarita Vihar, Mathura Road, New Delhi 110 044, India e-mail: makroo@apollohospitals.com, raj_makroo@hotmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Little data are available regarding the frequencies of the blood group antigens other than ABO and RhD in the Indian population. Knowledge of the antigen frequencies is important to assess risk of antibody formation and to guide the probability of finding antigen-negative donor blood, which is especially useful when blood is required for a patient who has multiple red cell alloantibodies. This study was carried out to determine the frequencies of the D, C, c, E, e, K, k, Fya, Fyb, Jka, Jkb, M, N, S and s antigens in over 3,000 blood donors.
Methods:
Samples from randomly selected blood donors from Delhi and nearby areas (both voluntary and replacement) were collected for extended antigen typing during the period January 2009 to January 2010. Antigens were typed via automated testing on the Galileo instrument using commercial antisera.
Results:
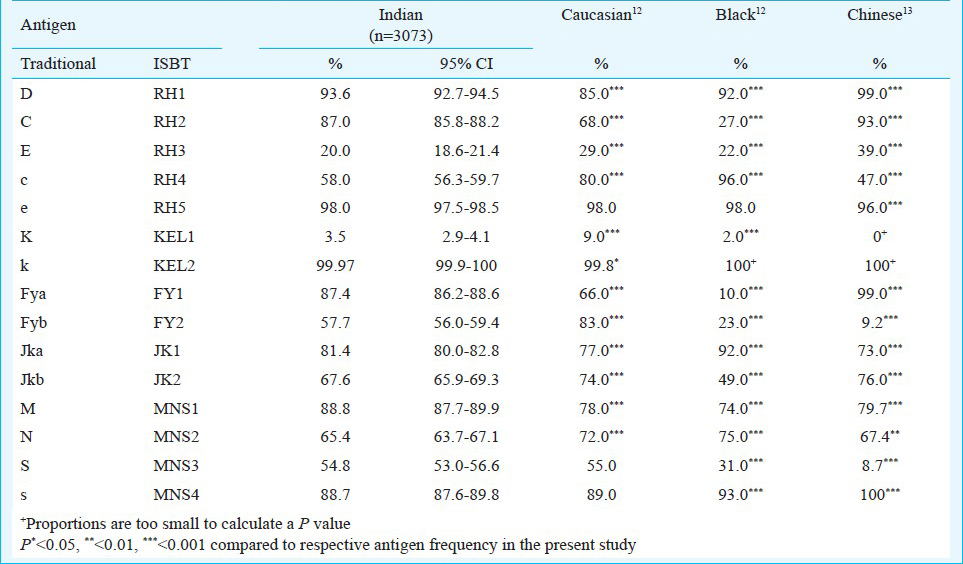
A total of 3073 blood samples from donors were phenotyped. The prevalence of these antigens was found to be as follows in %: D: 93.6, C: 87, c: 58, E: 20, e: 98, K: 3.5, k: 99.97, Fya: 87.4, Fyb: 57.6, Jka: 81.5, Jkb: 67.4, M: 88.7, N: 65.4, S: 54.8 and s: 88.7.
Interpretation & conclusions:
This study found the prevalence of the typed antigens among Indian blood donors to be statistically different to those in the Caucasian, Black and Chinese populations, but more similar to Caucasians than to the other racial groups.
Keywords
ABO
alloantibodies
blood group antigens
extended antigen typing

In India, more than 2,500 blood banks collect and transfuse a total of approximately 8 million blood units annually1. According to published data, rates of alloimmunization in random patients vary from 0 to 3 per cent2. Patients who develop alloantibodies in their blood are left with no option other than receiving blood units that are negative for the antigens against which the alloantibodies have been developed. Blood units that have been antigen typed and matched for these minor antigens show expected in vivo survival rates and prevent adverse transfusion reactions in these patients.
The alloantibodies, which frequently develop and are encountered during compatibility testing, are primarily against antigens related to Rh34, Kell5, Kidd6, Duffy7 and MNSs8 blood group systems. Antibodies directed against these antigens are implicated in cases of haemolytic transfusion reactions (HTRs) and haemolytic disease of the foetus and newborn (HDFN), and are, therefore, regarded as clinically significant if these react in the indirect antiglobulin test at 37°C9.
It is important to know the frequencies of the various antigens when dealing with patients who have developed multiple alloantibodies. This information is necessary to predict the availability of blood units that lack the corresponding antigen(s). The current practice of providing compatible blood to patients in such cases in India is still reliant upon random cross matching of available units in the inventory. This study was aimed to provide data regarding the frequency of various blood group antigens with their phenotypic expression in the Indian blood donors, and to compare with other ethnic groups/populations.
Material & Methods
Samples from randomly selected blood donors (both voluntary and replacement) coming for blood donation to the department of Transfusion Medicine, Indraprastha Apollo Hospital, New Delhi, India, were collected for extended antigen typing during January 2009 to January 2010. Written consent was taken at the time of donor screening. The study protocol was approved by the ethics committee of the hospital. The antigen typing of donors was performed using the Galileo fully automated immunohematology analyzer (Immucor, Roedermark, Germany) that uses the microplate haemagglutination technique for typing with IgM monoclonal antiserum and Capture-R Select (SPRCA-Solid Phase Red Cell Adherence) for typing with polyclonal IgG antiserum.
The D, C, c, E, e, K, M and N antigens were typed using monoclonal antisera from Immucor derived from clones D175-2/TH28, MS24, MS33, MS258+MS80, MS16+MS21, MS56, M-11H2 and 1422-C7, respectively. Donors typed as D negative were confirmed using an antiglobulin weak D test in an automated solid phase test using Novaclone anti-D (Immunocor Rodermark, Germany) which contains IgG clone D415 in addition to IgM clone D175-2. Fya, Fyb, Jka, Jkb, S, s and k antigens were typed by commercially prepared polyclonal antisera (Immucor) with Capture-R Select. Any NTD (no type determined) results determined by the instrument were further tested and confirmed using the test tube methods10. Those donors testing negative for both the antigens of the Duffy blood group system i.e. Fy (a-b-) were further tested by tube technique (Immunocor Rodermark, Germany) for confirmation.
To establish the validity of results of the automated system, the initial 100 samples were typed manually using the tube method10 in parallel to the study using reagents from Immucor Inc. The manual testing was done according to manufacturers’ (Immunocor Rodermark, Germany) instructions. No discrepancies were found in any of these tests.
Statistical analysis: For the antigen frequencies determined for the Indian donors 95% confidence intervals in this study were calculated using the formula CI: p-hat ± Z ((p-hat*(1 - p-hat))/n)11 where p-hat is the calculated proportion and n is the population number (in this case it was 3073). The significance of the difference between the determined frequencies and those published for other populations were calculated using a Z test (two-sided, alpha = 0.05) utilizing published antigen frequencies1213 as the hypothesized mean.
Results
A total of 3073 donors were typed during the study period. The most common Rh antigen observed in the study population was e (98%) followed by D (93.6%), C (87%), c (58%) and E (20%). The antigen frequencies among Indian donors were compared with those published for other populations (Table I). The frequency of D antigen in Indian donor population was significantly higher than in the Caucasians (85%) and lower than in the Chinese (99%). The frequencies of C, c and E antigens were dissimilar to other ethnic groups while the e antigen was present in high frequency in Indians as also in the other ethnic groups. (Table I).
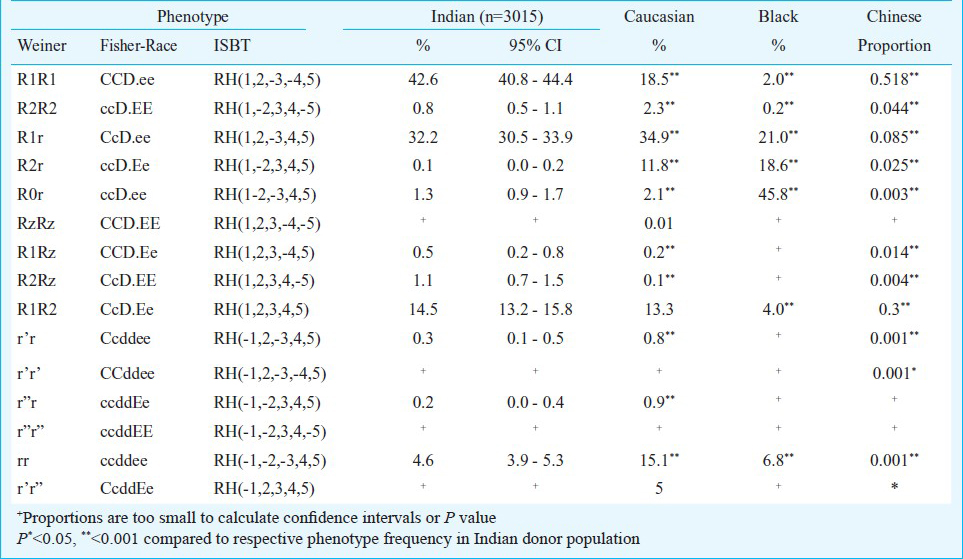
The frequencies of Rh Phenotypes among 3015 Indian donors were compared with those of other racial groups (Table II). The commonest Rh phenotype was R1R1 constituting 42.6% of the whole study population and the rarest was R2r (0.1%). The most common Rh phenotype among Caucasians was R1r (34.9%) and that in Blacks was R0r (45.8%). The frequencies of phenotypes for Kell, Fy, Jk and MNS systems were compared with those from other populations (Table III).
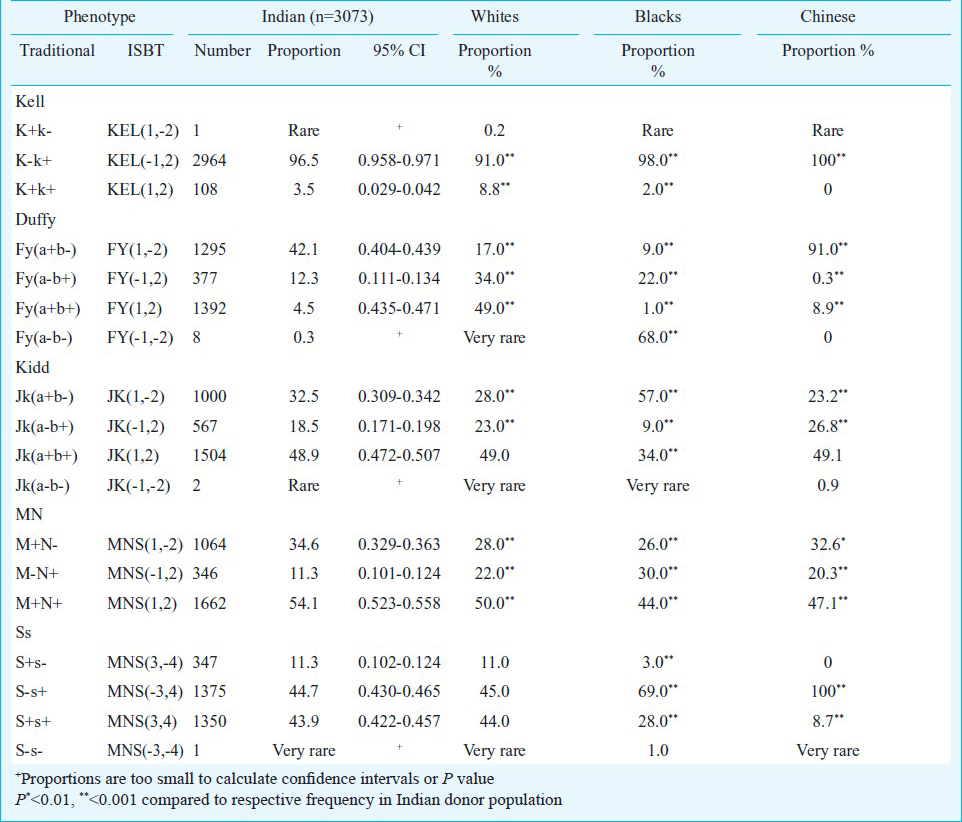
The frequency of the Kell antigen (K) was 3.5 per cent, while that of Cellano (k) was 99.97 per cent. Kell antigen frequency was intermediate between the frequencies reported for Caucasian (9%) and Black populations (2%). In the current study, only one donor was typed as k (Cellano) negative, therefore, this phenotype was labelled as “rare” in Indians as in the Black population. (Table III). The most common Kell phenotype was K-k+, not just in Indians (96.5%) but also in Caucasians (91%), Blacks (98%) and Chinese (100%) (Table III).
The frequencies of all Duffy phenotypes in the Indian donors were dissimilar to all of the three ethnic groups compared (Table III). Fy (a+b-) was the most common phenotype identified (42.1%) in Indians, while Fy (a+b+) was the most common phenotype in Caucasians (49%), and Fy (a-b-) in Blacks (68%). Frequency of Fy (a-b-) phenotype i.e. individuals lacking both Duffy antigens was 0.3 per cent in the present study. Of the 3073 donors, eight were identified and confirmed by test tube method. This phenotype is quite uncommon in the Caucasian and Chinese populations whereas 68% of Blacks have this ‘null’ phenotype.
The frequencies of the Kidd blood group system antigens (Jka = 81.4%, Jkb = 67.6%) were significantly different than other ethnic groups, but more similar to Caucasians (Jka = 77%, Jkb = 74%) and Chinese (Jka = 73%, Jkb = 76%) than to Blacks (Jka = 92%, Jkb = 49%) (Table I). The most common Kidd phenotype was Jk (a+b+) which was the same in Caucasian and Chinese populations, however, in Blacks Jk(a+b-) was the commonest phenotype (57%). Two donors were found to have the Jk (a-b-) phenotype, which is very rare in Caucasian and Black people, but higher frequencies have been reported in Chinese (0.9%) and other populations, such as Polynesian Islanders.
The distribution of MN frequencies in our population was statistically dissimilar to the other ethnic groups. The M+N+ phenotype was the most frequent in Indian population and other ethnic groups, being 54.1 per cent in Indians, 50 per cent in Caucasians, 44 per cent in Blacks and 47.1 per cent in Chinese (Table III).
Frequencies of S (54.8%) and s (88.7%) antigens in Indians were statistically similar to those of Caucasians, but different from Blacks and Chinese (Table I). S-s+ phenotype was the commonest in Indians as in Caucasians (45%) and Blacks (69%). (Table III).
Discussion
The knowledge of prevalence of different blood group antigens in any given population is always helpful in managing cases of alloimmunization. Multiply transfused patients such as those with thalassaemia, sickle cell anaemia, patients on dialysis, cancer patients, etc. are likely to develop antibodies against these minor blood group antigens as it is not practically feasible to match all these minor antigens before transfusion so as to avoid immunization. Finding compatible units for such patients without having any knowledge of the prevalence of the implicated antigens in the local population is a difficult task, more so if the patient has developed more than one antibody.
The results derived in our study were similar to those derived in another study on north Indian population by Thakral et al14. The differences in antigenic composition of Indian population and the Caucasian, Blacks and Chinese populations highlight certain important points. One of these is the use of screening cell panels with foreign antigenic profile. Most of the transfusion centers in our country that perform antibody screening to detect the presence of unexpected antibodies in their patients mostly use commercially prepared screening cell panel procured from western countries. The intention of improving blood safety by performing antibody screening in all prospective patients is a great step towards reducing adverse reactions caused by transfusion15. However, the use of screening cells prepared from foreign donors still leaves a possibility where the antibodies, especially the ones against minor antigens may go undetected12.
In recent years, medical tourism to India has increased largely due to affordable medical facilities available here. In context of transfusion medicine, this trend would mean that a large number of international patients would be receiving blood transfusions from Indian donors. The differences observed in antigen frequencies among different ethnic groups can lead to problems. One such example would be the relatively higher risk of development of Duffy antibodies in patients from Africa, who are transfused with blood from Indian donors since nearly 68% of the Blacks bear the Fy (a-b-) phenotype, while the prevalence of both the Duffy antigens among the Indians is relatively high.
The prevalence of cellano (k) antigen is almost 100% in the Indian population, whereas 0.2 per cent of the Caucasians are k negative12. This implies that while Caucasians occasionally develop anti-k (cellano), the likelihood of finding this alloantibody in Indians is negligible. This information also implies that if a Caucasian patient with anti-k requires blood in India, it will be very difficult to find a ‘k’ negative donor that is also compatible for ABO and D. This further indicates that the presence of ‘k’ negative cells in the identification cell panel may not be as important in India, as it is in the White dominated regions of the world where it is a must or at least preferred to have one ‘k’ negative cell to determine and confirm the specificity of anti-k in case it develops.
Though the sample size of this study was relatively small compared to the huge population of the country, it still gives an estimate of the frequencies of minor blood group antigens. The current study was conducted at the Indraprastha Apollo Hospitals, New Delhi, located in the northern part of country. Although this hospital generally caters to patients from all across India but most of the donors were from the north of India. The gene pool of people from other parts like south/east/west India may be somewhat different from that of the north Indians and thus a multi-centric study in hospitals located in different regions, would be valuable to provide information regarding the frequencies of the various blood group antigens in different regions of India.
Acknowledgment
As the extended phenotyping for antigens other than Rh and Kell is not performed routinely in our blood bank, the authors thank Immucor Gamma for providing all necessary reagent, equipments and technical assistance for this study.
Conflict of interest: The authors declare no conflict of interest.
References
- Red blood cell alloimmunization after blood transfusion. Leiden: University Press; 2008.
- [Google Scholar]
- Probability of anti-D development in D- patients receiving D+ RBCs. Transfusion. 2003;43:893-8.
- [Google Scholar]
- The Rh blood group system (and LW) In: Klein HG, Anstee D, eds. Mollison's blood transfusion in clinical medicine (11th ed). Oxford, United Kingdom: Blackwell Publishing Ltd; 2005. p. :163-208.
- [Google Scholar]
- The Kell blood group system: Kell and XK membrane proteins. Semin Hematol. 2000;37:113-21.
- [Google Scholar]
- Review: the Kell, Duffy, and Kidd blood group systems. Immunohematology. 2004;20:37-49.
- [Google Scholar]
- Transfusion- induced autoantibodies and different immunogenicity of blood group antigens: a novel hypothesis. Transfusion. 2007;47:2189-96.
- [Google Scholar]
- Red cell typing. Methods Section 2, AABB technical manual. (17th ed). Bethesda (MD): American Association of Blood Banks; 2011.
- [Google Scholar]
- Confidence Intervals: Confidence Interval for a Population Proportion [Connexions Web site] 2012. Available at: http://cnx.org/content/m16963/1.20/
- [Google Scholar]
- The distribution of blood group antigens and alloantibodies among Chinese in Taiwan. Transfusion. 1988;28:350-2.
- [Google Scholar]
- Phenotype frequencies of blood group systems (Rh, Kell, Kidd, Duffy, MNS, P, Lewis, and Lutheran) in north Indian blood donors. Transfus Apher Sci. 2010;43:17-22.
- [Google Scholar]
- Role of crossmatch in testing for serologic incompatibility. Transfusion. 1982;22:12-6.
- [Google Scholar]




