Translate this page into:
Prevalence of dental fluorosis & dental caries in association with high levels of drinking water fluoride content in a district of Gujarat, India
Reprint requests: Dr Patel Sangita V., 5, Gokul Society, Sindhwai Mata Road, Pratapnagar, Vadodara 390 004, India e-mail: sangita_psm@yahoo.co.in
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Endemic fluorosis resulting from high fluoride concentration in groundwater is a major public health problem in India. This study was carried out to measure and compare the prevalence of dental fluorosis and dental caries in the population residing in high and normal level of fluoride in their drinking water in Vadodara district, Gujarat, India.
Methods:
A cross-sectional study was conducted in Vadodara district, six of the 261 villages with high fluoride level and five of 1490 with normal fluoride level in drinking water were selected. The data collection was made by house-to-house visits twice during the study period.
Results:
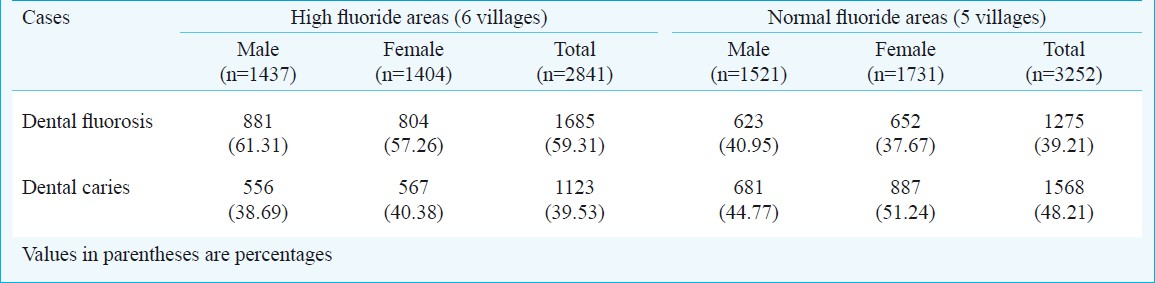
The dental fluorosis prevalence in high fluoride area was 59.31 per cent while in normal fluoride area it was 39.21 per cent. The prevalence of dental caries in high fluoride area was 39.53 per cent and in normal fluoride area was 48.21 per cent with CI 6.16 to 11.18. Dental fluorosis prevalence was more among males as compared to females. Highest prevalence of dental fluorosis was seen in 12-24 yr age group.
Interpretation & conclusions:
The risk of dental fluorosis was higher in the areas showing more fluoride content in drinking water and to a lesser degree of dental caries in the same area. High fluoride content is a risk factor for dental fluorosis and problem of dental fluorosis increased with passage of time suggesting that the fluoride content in the water has perhaps increased over time. Longitudinal studies should be conducted to confirm the findings.
Keywords
Cross sectional study
dental caries
dental fluorosis
fluoride water
India
prevalence rate

Endemic fluorosis resulting from high fluoride concentration in groundwater is a public health problem in India. The available data suggest that 15 States in India are endemic for fluorosis (fluoride level in drinking water >1.5 mg/l), five of these have category III (>50% of the districts affected) which includes Gujarat1. The Assam region of North East India has also been recognized as a fluoride-affected area2. World Health Organization (WHO) has set the upper limit of fluoride concentration in drinking water at 1.5 mg/l3. The Bureau of Indian Standards, has therefore, laid down Indian standards as 1.0 mg/l as maximum permissible limit of fluoride with further remarks as “lesser the better”4. The WHO in Oral Health Report (2003)5 has stated fluoride as most effective agent in dental caries prevention.
Gujarat Water Supply and Sewerage Board (GWSSB) has surveyed all the villages in Gujarat and reported 15.8 per cent of the villages having fluoride level more than 1.5 mg/l (personal communication, GWSSB).
This study was aimed to test the hypothesis whether high fluoride level in drinking water is more a risk factor leading to fluorosis than its protective role in the prevention of dental caries.
The objectives were to measure the prevalence of dental fluorosis and dental caries in the population residing in areas with high and normal level of fluoride in the drinking water, and to find out whether high fluoride level in drinking water is more protective for dental caries or a risk factor for dental fluorosis.
Material & Methods
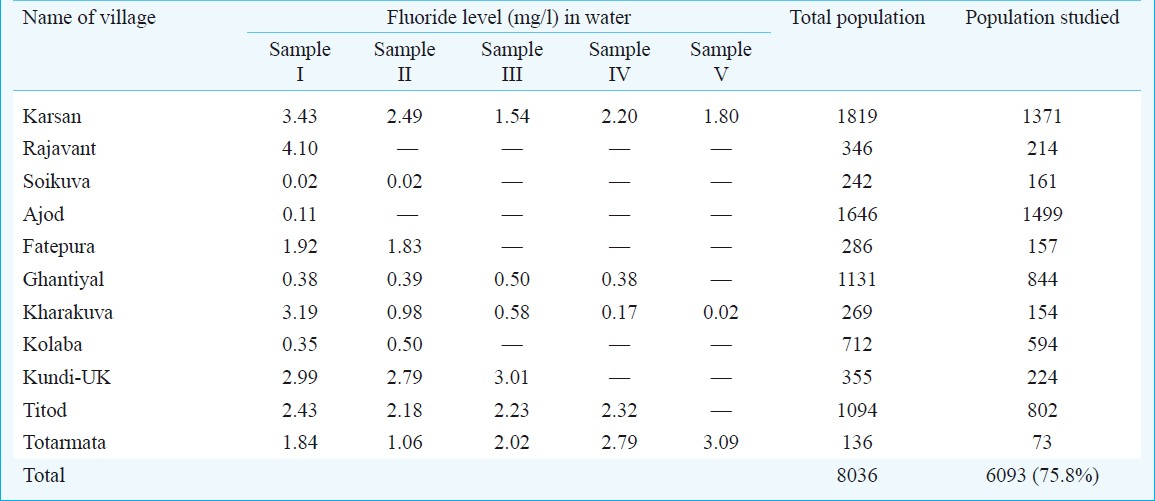
This cross-sectional prevalence study was conducted by the Department of Preventive and Social Medicine, Medical College, Vadodara, Gujarat, for a period of six months. Vadodara district has total 7794 sq. kilometer area spread in 12 talukas and 1651 villages6. Ethical approval for the study was obtained from institutional review board of Medical College, Vadodara. Under assumption of detecting a difference of 3 per cent prevalence in dental fluorosis in the areas having high and normal fluoride in the drinking water, the sample size required was 2500. Of the 1651 villages, 261 (15.81%) have been detected to have drinking water fluoride level of more than 1.5 mg/l (personal communication, GWSSB). Eleven of these 261 villages having high fluoride content in the drinking water and 11 villages of the remaining 1490 having normal fluoride in drinking water were randomly selected for water sampling. Water samples were collected from all the water sources (maximum 5) from all these selected villages. The analysis for the fluoride level was made by auto analyzer using a spectrophotometric method7. The results of these 22 villages were compared with GWSSB reports (personal communication, GWSSB). Eleven of the 22 villages showed similar findings and these 11 villages were selected for further study (Table I). Of these 11 villages, five had fluoride level <1.5 mg/l. All the houses in each village were visited for data collection by trained tutors and assistant professors of Preventive and Social Medicine Department, Medical College, Vadodara. All age groups were included in the study after taking informed consent. Those who could not be studied in the second visit were excluded from the study.
Dental caries care was counted when any of the teeth falls into the category of decayed, decayed and filled or missing due to caries (grade 2, 3, or 4)8 and dental fluorosis when tooth was not normal. The grading for dental fluorosis was done as: questionable (grade 1), very mild fluorosis (grade 2), mild fluorosis (grade 3), moderate fluorosis (grade 4), and severe fluorosis (grade 5)9.
For subsequent analysis all the grades of fluorosis were dichotomized as fluorosis (grade 1 to grade 5) or no fluorosis (grade 0) and area was also dichotomized as high fluoride villages (water fluoride level >1.5 mg/l, villages Karsan, Rajavant, Fathepura, Kundi-U.K., Titod & Totarmata) and normal fluoride level (water fluoride level ≤ 1.5 mg/l, villages Ajod, Ghantial, Kharakuva, Kolaba & Soikuva). Data were analyzed by Chi-square and Mental Hensel Chi-square tests.
Results
The prevalence of dental fluorosis in high fluoride area was 59.31 per cent while in normal fluoride area it was 39.21 per cent (Table II). The difference was statistically significant (CI 17.59-22.57% with RR=1.51). Also the prevalence of dental caries in high fluoride area was 39.53 per cent and in normal fluoride area was 48.21 per cent with a difference of 8.68 per cent (CI 6.16 to 11.18%), RR=0.82 indicating protective effect of fluoride for dental caries.
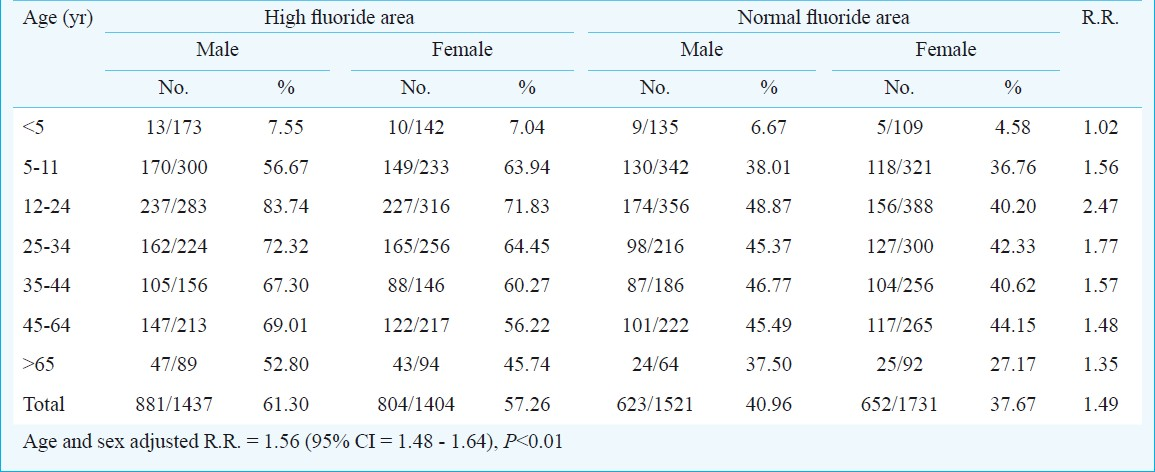
The prevalence of dental fluorosis in high fluoride area was 61.30 per cent in males and 57.26 per cent in females while in normal fluoride area was 40.96 per cent in males and 37.67 per cent in females (Table III). Age and sex adjusted R.R. was 1.56 with CI 1.48-1.64 per cent. The prevalence of dental fluorosis was highest in 12 to 24 yr age group.
Discussion
Of the total population under study (n=8036), 6093 persons (response rate of 75.8%) were studied. The non-response rate was more (28.91%) (1203/4161) for men while for women it was only 19.1 per cent (740/3875). This was due to their non-availability for various reasons including being out of station for work or sickness, etc. The prevalence of dental fluorosis in the study population was 49.26 per cent. Choubisa9 reported the prevalence of dental fluorosis as 45 per cent among 21 different villages in southern Rajasthan. Another study conducted in a village in Maharashtra also found the prevalence of dental fluorosis as 43 per cent10. In Turkey, the dental fluorosis prevalence was reported as 29 per cent in normal fluoride area and 77 per cent in high fluoride area among 12 to 14 yr old school children11. A study conducted on Mexican school going children showed the prevalence of dental fluorosis as 60 per cent12. In Tanzania, Vuhahula et al13 observed the prevalence of dental fluorosis as 96.3 per cent.
Our findings do not tell us about the period of fluoride ingestion in the studied population. Dental fluorosis develops only when one is exposed to high fluoride level during 0-6 yr of age when dentition develops. Once fluorosis develops, it is permanent14.
Dental caries being lower in high fluoride area is suggestive of its protective effect. Similar findings were observed earlier by Tsutsui et al15 in Japanese communities, and also by others16. There is no alternative but to reduce exposure to fluoride level for prevention of fluorosis while dental caries can be prevented by the improved oral hygiene and ensuring the reduced bacterial growth and less production of acid17. One study conducted in Namibia on fluorosis, caries and oral hygiene in school children observed that high concentrations of fluoride in drinking water alone did not result in acceptable caries levels18.
The relative risk of having dental fluorosis increased with decrease in age up to 12 yr and age and sex adjusted relative risk was 1.56 with the 95 per cent confidence interval of 1.48 to 1.64. The analysis suggested to interpret the age-wise data separately as the relative risk differed by the stratum. The crude R.R. was 1.49.
While discussing effect of fluoride in drinking water on dental fluorosis, one major confounder may be for those who stay currently in high or normal fluoride areas but at the time of the permanent dentition (first 6 years of their life) may not be staying there and, therefore, would be misleading the analysis. To correctly interpret the data, we need to have the exact information of their stay at the time of dentition. Alternatively, we restricted the analysis to those who were staying in the same villages since birth. For re-analysis, the study population was excluded for those who have not been staying in the respective villages from the birth. The difference in dental caries decreased while difference in dental fluorosis increased justifying the need for removing the confounder in the analysis. The crude, and age and sex adjusted relative risk also increased for dental fluorosis for high fluoride area. Further, it also indicates that fluoride in water is more a risk factor for fluorosis than a protective factor for dental caries.
In conclusion, our findings showed that the risk of dental fluorosis was significantly higher in the areas showing more fluoride content in drinking water and to a lesser degree of dental caries in the same area. There was also an increased problem of dental fluorosis with the passage of time. It is recommended to reduce the fluoride content of drinking water in the high fluoride area by making either alternative sources available or providing water with reduced fluoride content.
References
- Fluorosis: Indian scienario : A treatise on fluorosis. New Delhi: Fluorosis Research and Rural Development Foundation; 2001.
- Fluoride and endemic fluorosis in the Karbianglong district, Assam, India. Res Rep Fluoride. 2008;41:42-5.
- [Google Scholar]
- World Health Organization. In: Guidelines for drinking water quality. Geneva: WHO; 2004.
- [Google Scholar]
- Government of India. In: Prevention and control of fluorosis in India. New Delhi: Rajiv Gandhi National Drinking Water Mission; 1993. p. :25.
- [Google Scholar]
- WHO. In: The World Oral Health Report 2003; Poul Erik Peterson. Geneva: World Health Organization; 2003.
- [Google Scholar]
- Government of India. 2001. Census 2000. New Delhi: Ministry of Home Affairs, Office of the Registrar General and Census Commissioner of India; Available at: http://censusindia.gov.in/
- [Google Scholar]
- DHV Consultants BV & Delfthydraulics. In: How to measure Fluoride: SPADNS spectrophotometric method, Training module # WQ - 36. 2000.
- [Google Scholar]
- Endemic fluorosis in an isolated village in western Maharashtra, India. Trop Doct. 2006;36:221-3.
- [Google Scholar]
- Dental caries and fluorosis in low- and high-fluoride areas in Turkey. Quintessence Int. 2003;34:354-60.
- [Google Scholar]
- Fluoride consumption and its impact on oral health. Int J Environ Res Public Health. 2011;8:148-60.
- [Google Scholar]
- Dental fluorosis in Tanzania Great Rift Valley in relation to fluoride levels in water and in ‘Magadi’ (Trona) Desalination. 2009;248:610-5.
- [Google Scholar]
- The prevalence of dental caries and fluorosis in Japanese communities with up to 1.4 ppm of naturally occurring fluoride. J Public Health Dentistry. 2000;60:147-53.
- [Google Scholar]
- High fluoride concentration in drinking water may increase the prevalence and severity of dental fluorosis, and decrease occurrence of caries. J Evidence-based Dental Practice. 2008;8:15-6.
- [Google Scholar]
- Fluorosis, caries and oral hygiene in schoolchildren on the Ombili Foundation in Namibia. Oral Health Prev Dent. 2010;8:269-75.
- [Google Scholar]




