
Translate this page into:
Prevalence & correlates of tobacco use among adolescents in Kerala, India
Reprint requests: Dr T. S. Jaisoorya, Department of Psychiatry, National Institute of Mental Health & Neurosciences (NIMHANS), Bengaluru 560 029, Karnataka, India e-mail: tsjaisoorya@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Most tobacco users who initiate its use during adolescence are likely to continue the use into adulthood and contribute to the 90 per cent of premature deaths among tobacco users. In this context the prevalence, patterns and correlates of tobacco use were studied among adolescent school students in Kerala, India.
Methods:
Total 7560 students from classes 8, 10 and 12, within the age group of 12-19 yr, across 73 schools in Ernakulam district, Kerala, India, selected by cluster random sampling, completed a self-administered questionnaire incorporating standardized instruments.
Results:
Of the 7350 valid questionnaires, the overall lifetime prevalence of tobacco use was 6.9 per cent (12.5% males and 1.2% females). The prevalence of tobacco use increased from 3.1 per cent at 12-13 yr to 15.1 per cent at 18-19 yr. The mean age of onset of tobacco use was 14.0±2.2 yr. The prevalence was higher among students from urban backgrounds, lower socio-economic status and those with part-time jobs. Tobacco users had significantly higher rates of use of alcohol (67.8 vs. 11%) and illicit drugs (33 vs. 6.1%). They had poorer academic performance (24.7 vs. 9.1%), more severe psychological distress (10.8 vs. 4.5%), suicidal attempts (10.2 vs. 3.5%), higher scores of ratings of attention deficit hyperactivity disorder (8.3 vs. 2.5%) and history of sexual abuse (12.5 vs. 3.8%).
Interpretation & conclusions:
The prevalence of tobacco use in adolescents reported in this study was relatively lower than those reported from other Indian States. However, it correlates with multiple negative outcomes suggesting a need to promote specific interventions to prevent adolescent tobacco use.
Keywords
Adolescent
correlates
epidemiology
India
risk behaviour
tobacco use

Tobacco is the most commonly abused drug in the world. The most susceptible time for initiation of tobacco use in India is during adolescence and early adulthood i.e., in the age group of 15-24 yr1. Worldwide, nearly, all (88%) initiation to smoking occurs before the age of 18 yr. Among every three young smokers, only one will quit and one of the remaining smokers will die of tobacco-related causes2. Data from the Monitoring the Future Study showed that 38 per cent of American school students of both genders were regularly smoking by 12th grade in 2013, in spite of the overall prevalence showing a declining trend since 19963. In India, it is estimated that about five million children under the age of 15 are tobacco users4. The Global Youth Tobacco Survey (GYTS) (2000-2004), the first national survey of tobacco use among adolescents in India5, reported the prevalence of ever use of tobacco in any form to be 25.1 per cent, with current cigarette smoking being 17.5 per cent and current use of smokeless tobacco (SMT) to be 14.6 per cent in the age group of 13-15 yr5. In replications of the GYTS in 2006 and 2009, about 14 per cent (13.7% in 2006 and 14.6% in 2009) of students aged 13-15 yr reported using tobacco (smoking and/or SMT)5. Two school surveys from Kerala, one an exclusive rural survey reported eight per cent prevalence and the second from northern Kerala reported the prevalence of tobacco smoking and chewing to be 9.8 and 2.2 per cent, respectively in students between 13 and 17 yr67.
In studies from India, the mean age of initiation to tobacco varied between eight and 15 years689. Across studies worldwide, using different measures of current smoking status, smoking has been found to increase with age. The prevalence of smoking increases in all countries, from around five per cent at 11 yr to 10-25 per cent at 15 yr1910. Most studies from India report a male predominance (10-30 vs. 1-3%),89 in contrast to most Western studies311 and a few Indian studies1213 which have reported a female predominance or equal prevalence.
Many family characteristics have been shown to influence adolescent tobacco use. Low family income, low parental education and living in single-parent families have been found to predict smoking in American adolescents3. Family factors such as high levels of connectedness, monitoring and parental punishment were protective against smoking9121314.
Nicotine use has been correlated with many adolescent problem behaviours including sexual risk behaviours, aggression, alcohol and illicit drug use15161718. High levels of impulsivity have been reported in adolescents who initiate smoking early [19.0-46% vs. 10-24% for adolescents with and without attention deficit hyperactivity disorder (ADHD), respectively]1619. Adolescents who smoke are also reported to have higher rates of anxiety and mood disorders than non-smokers17. Smoking has been shown to be positively correlated with suicidal ideation and suicidal attempts17. An Indian study with a small sample size reported a positive correlation between sexual risk behaviour and nicotine use15. Though studies have reported prevalence and factors associated with initiation of adolescent tobacco use in India, there is little information available on the psychosocial correlates of tobacco use among adolescents in the community. The present study was undertaken to determine the prevalence of tobacco use among schoolgoing adolescents of age 12-19 years and to evaluate the pattern of use and psychosocial correlates among adolescents who have reported lifetime tobacco use in Kerala, India.
Material & Methods
This single-stage cross-sectional epidemiological survey was conducted in January 2013 in a single random division of classes (year) 8, 10 and 12 of 73 schools. These schools were selected by cluster random sampling from the 168 high and higher secondary schools in the district of Ernakulam, Kerala, India. Each of the four educational subdistricts formed a cluster. In each of the cluster, 40 per cent of institutions were randomly selected. The initial sample size calculated to identify one per cent prevalence with 95 per cent confidence interval with a five per cent error and 50 per cent response distribution was 3520. Of the 73 schools surveyed, the number of schools in government sector was 45 and in the government-aided sector was 28. Further, 51 of the surveyed schools were situated in the panchayat area, 15 in the municipal areas and seven were situated within corporation limits.
In addition to tobacco use, other domains assessed included the use of other substances, psychological distress and ADHD. Standardized instruments or pertinent sections or questions from standardized instruments were identified. To assess suicidality and sexual abuse, checklists were constructed using questions from standardized instruments with items being determined by expert consensus. The time allocated for the survey was restricted to one school period (50 min). The questionnaire initially prepared in English was translated into Malayalam (the vernacular language) and then back translated to check for accuracy. In addition, a pilot study was conducted in four schools (not included in the data analyzed) to test for accuracy of translation and validity. No psychometric properties of specific instruments were tested for the purpose of this survey.
Assessment tools: Socio-demographic profile (age/sex/area of residence/economic indicators/religion/academic performance) was assessed using a checklist. For assessing socio-economic status, students were asked to indicate whether their family belonged to the ‘below poverty line’ or ‘above poverty line’. No formal instruments were used for the assessment of socio-demographic profile and socio-economic status.
Tobacco & substance use: The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) developed by the WHO18 was used to assess the use of alcohol, tobacco and other drugs. Tobacco use assessed in the questionnaire refers to ‘lifetime use’ (defined as having smoked/used SMT ever in their lifetime) and ‘current use’ (defined as having smoked/used SMT in the last one month). The ASSIST provides information about people who have used tobacco in their lifetime; the pattern of tobacco use in the past three months; craving; need to cut down; the level of others’ concern about the person's tobacco use and problems related to use. An individual response to each of these questions has a standardized score and it is possible to calculate the tobacco involvement score by adding together the standardized scores of each of the questions. Three groups of people could be distinguished based on tobacco involvement score: those with tobacco involvement score of 0-3: abstainers or low risk users (means they may not be using or using tobacco occasionally, with no likely harm now or in the future if they continue the same pattern); those with tobacco involvement score of 4-26: indicates hazardous use (means the individual is of moderate risk of harm from their current pattern of use); and tobacco involvement score 27+ : indicates dependence (means a dependent pattern of use on tobacco with serious problems in multiple areas of life). The test-retest reliability coefficients of ASSIST ranged between 0.58 and 0.90. The internal consistency of the different domains ranged between 0.77 and 0.94. The sensitivity values were between 66 and 91 per cent while specificity values were between 80 and 91 per cent18. Use of alcohol and illicit drugs (cannabis, solvents and other substances grouped together) was reported only as lifetime use.
Psychological distress - Kessler's Psychological Distress Scale (K10): Psychological distress was assessed using Kessler's Psychological Distress Scale (K10)20, a screening tool for non-specific psychological distress. This tool has been validated to screen common mental disorders in developing country settings including India. It consists of ten questions to elicit the frequency of depressive and anxiety symptoms over the past month on a 4-point Likert scale. Based on the total scores, psychological distress can be categorized into mild, moderate and severe20. K10 has been shown to have high internal consistency (Cronbach's α -0.8), high correlation with composite international diagnostic interview (0.84) and area under curve of 0.8.
Assessment of suicidality: A checklist constructed from items in the Suicidal Behaviour questionnaire (SDQ-14)21 was used to assess lifetime suicidality. Two questions were asked to assess lifetime suicidality. ‘Have you ever thought of killing yourself?’ ‘Have you ever made an attempt to kill yourself?’
Assessment of sexual abuse: Four questions taken from ISPCAN Child Abuse Screening Tool Children's Version (ICAST-C)22, an instrument validated in India, were asked with regard to lifetime exposure to sexual abuse. These questions were: (i) has someone misbehaved with you sexually against your will; (ii) has someone forced you to look at pornographic materials against your will; (questions 1 & 2 – non-contact sexual abuse); (iii) has someone forced you to fondle or fondled you against your will; and (iv) has someone forced you to a sexual relationship against your will (questions 3 & 4 - contact sexual abuse).
Assessment of ADHD: Using Barkley Adult ADHD rating scale–IV (BAARS–IV) – Childhood Symptoms self-report23, the students were asked to rate their behaviour for features of ADHD between the ages of 5-12 yr. The scale consists of 18 questions – nine for features of inattention and nine questions for hyperactivity-impulsivity. Each question was rated in the form of a Likert scale with four options ranging from ‘never’ to ‘always’. Based on the total ADHD scores, it was possible to categorize the presence or absence of ADHD. Reliability of the scores was quite satisfactory as evidenced by high internal consistency (Cronbach's alpha of 0.92 for current ADHD and 0.95 for childhood ADHD symptom scores); good interobserver agreement (0.67 to 0.70 across scales) and high test-retest reliability over a 2-3 wk interval (0.75 for current ADHD and 0.79 for childhood ADHD symptom scores).
Ethical considerations: Institutional ethical approval was received from Government Medical College, Ernakulam, and administrative approvals were received from the school authorities prior to the survey. Information about the nature of the survey was provided to the parent-teacher association, and parental consent was obtained. The questionnaires were administered only to consenting students. Students who did not wish to take part were given the option either to leave the classroom (none did) or return the questionnaire unanswered (2.7% questionnaires were unanswered).
Students were also told that if they required any help with regard to issues surveyed, they could approach the School Junior Public Health Nurses (JPHNs), who had received training in handling these issues.
Statistical analysis: Statistical Package for Social Studies (SPSS) version 15 (SPSS Inc., Chicago, USA) was used for the analysis. Life time prevalence of tobacco use was determined. The pattern of use was determined among tobacco users. The socio-demographic variables were compared between the tobacco and non-tobacco groups using Chi-square and Fisher's exact tests, as necessary. Academic performance, self-reported prevalence of psychological distress, suicidality and sexual abuse, and ADHD were compared between the tobacco and non-tobacco groups using logistic regression analysis. A multivariable binary logistic regression was done to identify factors related to tobacco lifetime use by controlling for socio-demographic variables which were significant. The forward step-wise Wald method24 was used for variable selection. The Hosmer–Lemeshow test was used for the model fitting24. All tests were two-tailed.
Results
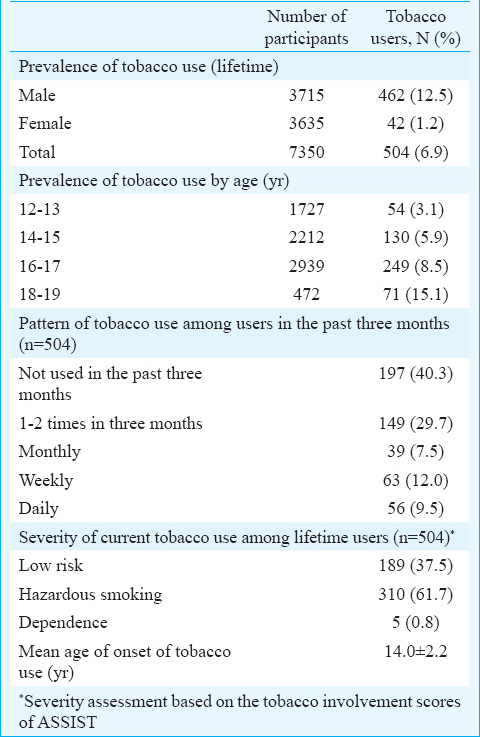
A total of 7560 students (97.7%) of the total 7740 eligible students, from 73 schools took part in the survey. Of the total questionnaires, 210 (2.7%) were discarded as these were found unanswered and the rest (n=7350) were analyzed. The response rate was 97.3 per cent. Of the questionnaires analyzed, 3715 (50.6%) were boys and 3635 (49.4%) were girls with a mean age of 15.3±1.7 yr and range 12 -19 yr. The prevalence and pattern of tobacco usage among school students are described in Table I. A total of 504 (6.9%) adolescents reported lifetime use of tobacco, of whom 462 (12.5%) were boys and 42 (1.2%) were girls. Gender differences between tobacco users were not analyzed as number of girls using tobacco was small. There was increasing use of tobacco with age with the proportion of students with lifetime alcohol use increasing from 3.1 per cent in age category 12-13 yr to 15.1 per cent at 18-19 yr. Current use was 29 per cent. Daily use was reported in 9.5 per cent of users. Among students who reported lifetime tobacco use (n=504), the frequency and severity of tobacco use (indicated by collated ASSIST scores) showed 37.5 per cent of users were at low risk and 61.7 per cent of users had hazardous level of use. Dependent use (0.8%) was only reported among boys. The mean age of onset of tobacco use was 14±2.2 yr (Table I).
The socio-demographic variables are shown in Table II. Urban residence (P<0.004), lower socio-economic status (P<0.01) and having a part time job (P<0.01) were significantly correlated with lifetime tobacco use. There was no significant correlation with family structure or religion.
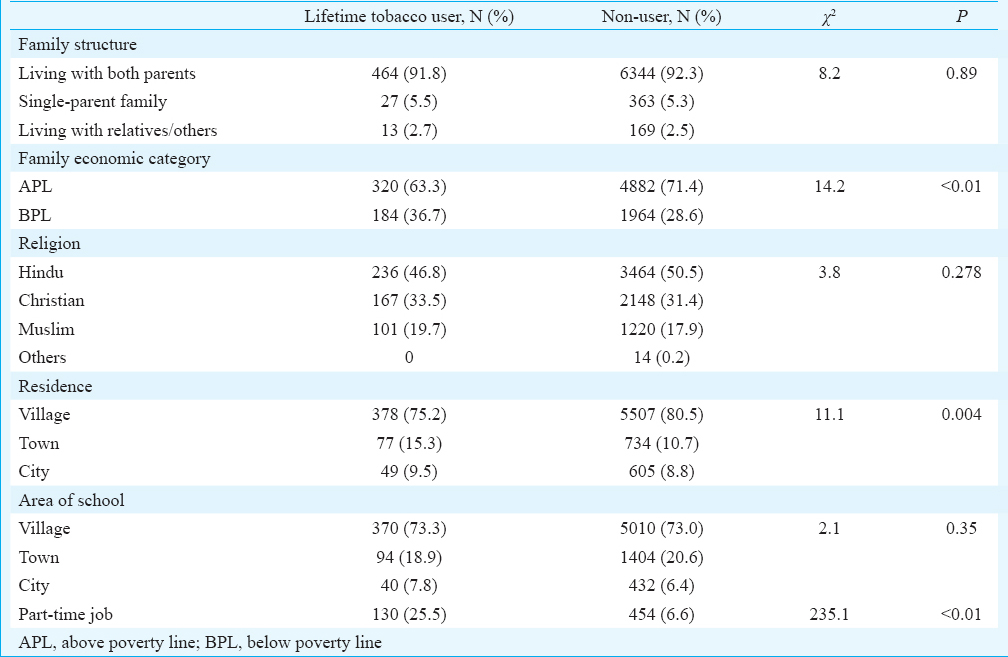
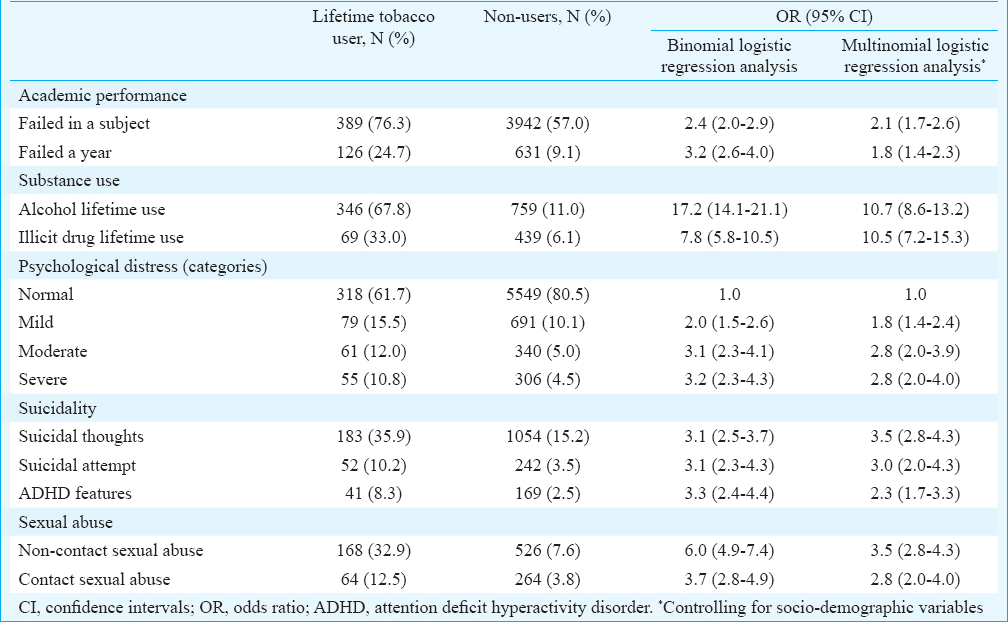
Table III describes the academic and psychological correlates of tobacco use. In the bivariate analysis, use of tobacco was highly predictive of use of alcohol and illicit drugs. Further, students who used tobacco had significantly higher odds of poorer academic performance, psychological distress, suicidal thoughts, suicidal attempts, ADHD, contact and non-contact sexual abuse (Table III). In the multivariable binary logistic regression analysis, the variables that were significantly associated with tobacco lifetime use after controlling for socio-demographic variables were failure in a year and a subject, alcohol use, illicit drug use, psychological distress, suicidal ideas, suicidal attempts, ADHD and sexual abuse. The Hosmer–Lemeshow test indicated that the model had adequate fit. The overall percentage predicted was 94.1 per cent.
Discussion
The overall prevalence of lifetime tobacco use in our study among adolescents of age group 12-19 yr was 6.9 per cent, with 12.5 per cent of males and 1.2 per cent females reporting use. The prevalence found in our study was lower than the rates of the nationwide survey conducted in 2009 which reported prevalence of 9.5 per cent5, and a Kerala study in 2011 reporting 9.8 per cent prevalence7. Further, the prevalence reported was much lower than findings from studies from Western countries which showed varying prevalence between 20 and 67 per cent311. The unique and geographically varying social, economic, cultural characteristics and tobacco policies could account for the wide range of prevalence rates of tobacco use reported across different States/countries. The low prevalence of tobacco use reported in our study could also be due to public health measures taken in Kerala. Smoking in public places is banned in Kerala and there is a ban on the sale of tobacco products around educational institutions following implementation of the Cigarettes and other Tobacco products (Prohibition of Advertisement and Regulation of Trade and Commerce, Production Supply and Distribution) Act, 2003 (COTPA)25.
Though the age category comparative prevalence rates of our study was lower than the other studies1234510, the increasing prevalence with age has been reported prior, in multiple studies from India and other countries1234510. Males were more likely to smoke than females in our sample. Most studies from India16 have reported male predominance suggesting that social norms against female tobacco use, especially smoking, continues to be strong. The exceptions have been reported from a few small States such as Goa and north-eastern States which have reported almost equal prevalence1213, reflecting the gender distribution seen in studies from Western countries310. Though our prevalence rates of tobacco use were relatively lower than many other studies, 61.7 per cent of adolescent users in our sample were hazardous users and 0.8 per cent dependent users as assessed by the ASSIST tobacco involvement scores. Daily use of tobacco was seen in 9.5 per cent of users and current use was 29 per cent. The higher proportion of users having hazardous use and current use in adolescence could be owing to tobacco being highly addictive26.
The mean age of onset of tobacco use of 14 yr was comparable to another study from Kerala which reported an age of onset of around 13 yr9. Many Indian studies, particularly from States reporting higher prevalence, have observed a younger age of onset, for example, of 10 yr or less15, which is also similar to studies in countries with high baseline prevalence among adolescents310.
Tobacco use was higher among students belonging to the lower socio-economic status similar to previous findings345. Adolescents engaged in a part-time job had significantly increased risk of tobacco use. A higher proportion of students working part time belonged to the lower socio-economic class, thus having access to extra income. Thus students from lower socio-economic status in our sample had greater access to disposable income which is known to increase the risk of tobacco and substance use8. (This text was present in submission). This factor could have contributed in addition to already reported risk factors in families from lower socio-economic status which includes larger family size, lower parental education and less effective supervision15. This study was cross-sectional in nature, and the data could not be used to support directionality or causality. Yet, the data appeared to suggest that students with tobacco use had significantly greater academic failures (similar to previous reports of association between substance use and lower academic achievement610). Students who used tobacco in our study had a significantly higher risk of using alcohol and illicit drugs supporting to prior literature that use of one substance increases the risk of use of other substances27.
Students with tobacco use had higher psychological distress, suicidal thoughts and suicidal attempts. Though there are no Indian studies looking at these links, previous studies from other countries have found that adolescents who smoke have higher rates of anxiety and mood disorders than non-smokers19, and higher rates of smoking have been found in the group with severe psychological distress in comparison to people without distress17. Smoking has also been correlated with suicidal ideation and suicidal attempts17. This may suggest that tobacco use may be used as forms of ‘self-medication’ to manage psychological distress and suicidality1928.
In our study, retrospective self-reported ADHD features in childhood were higher among tobacco users. Though the retrospective assessment of ADHD has its limitations with regard to accuracy of recall, it has been suggested that childhood ADHD symptoms predict onset as well as progression from experimental to daily and dependent smoking16. Studies have also shown ADHD to be associated with eventual development of tobacco and substance use disorders which have an earlier onset and greater severity1617. Our findings that contact sexual abuse and non-contact sexual abuse were correlated with tobacco use have added to the evidence that sexual abuse/risk behaviours and substance use form an important cluster in adolescent risk behaviours1929. While most studies have been in clinical samples, one community study also reported the same association15.
The present study had some limitations. First, this study did not include out of school adolescents who tend to have higher risk for using tobacco and other drugs30. Second, the use of different forms of tobacco was not assessed separately. Third, all aspects were evaluated by using questionnaires and no evaluation was carried out by mental health professionals. For assessment of suicidality and sexual abuse questions in the form, checklists were used. Fourth, the cross-sectional design on some aspects of the questionnaire (psychological distress) provided information about the present state and did not allow inferences on lifetime psychopathology. Fifth, the information of the questionnaire was collected anonymously which precluded any individual specific intervention. Finally, many factors which are known to influence adolescent tobacco use including peer pressure and parental tobacco use were not assessed.
In conclusion, the overall lifetime prevalence of tobacco use in our study was 6.9 per cent which was lower in comparison to findings from previous studies in Kerala and other regions of India. The association of tobacco use with psychological distress, suicidality, sexual abuse and ADHD was observed among tobacco using adolescents from Kerala. Given the multiple negative correlates and clustering of risk behaviours among adolescents who use tobacco, there is a need to further promote specific public health policies and interventions to prevent tobacco use among adolescents.
Acknowledgment
The study was partly funded by the NRHM (Kerala). The authors thank the Junior Public Health Nurses (JPHNs) and Block PROs of NRHM (Ernakulam) who were involved in administering the questionnaire and Shri Ajayakumar and team who helped in the data entry.
Conflicts of Interest: None.
References
- Reddy KS, Gupta PC, eds. Report of tobacco control in India. New Delhi: Ministry of Health and Family Welfare, Government of India; 2004.
- U.S. Department of Health and Human Services. 2012. Preventing tobacco use among youth and young adults: A report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; Available from: http://www.surgeongeneral.gov/library/reports/preventing-youth-tobacco-use/full-report.pdf
- [Google Scholar]
- Monitoring the future national results on drug use: 1975-2013: Overview, key findings on adolescent drug use. Ann Arbor: Institute for Social Research, The University of Michigan; 2014.
- Prevalence of tobacco use in Karnataka and Uttar Pradesh In India. New Delhi: Indian Council of Medical Research; 2001.
- A survey of 24,000 students aged 13-15 years in India: Global Youth Tobacco Survey 2006 and 2009. Tob Use Insights. 2010;3:23-31.
- [Google Scholar]
- Self-reported tobacco use, knowledge on tobacco legislation and tobacco hazards among adolescents in rural Kerala State. Indian J Dent Res. 2011;22:195-9.
- [Google Scholar]
- Evaluation of a tobacco control programme to reduce tobacco use among school children in Kerala. Asian Pac J Cancer Prev. 2013;14:3455-9.
- [Google Scholar]
- Tobacco use and related factors among pre-university students in a college in Bangalore, India. Natl Med J India. 2009;22:294-7.
- [Google Scholar]
- Tobacco use in Kerala: findings from three recent studies. Natl Med J India. 2005;18:148-53.
- [Google Scholar]
- Psychosocial correlates of substance use in adolescence: a cross-national study in six European countries. Drug Alcohol Depend. 2007;86:67-74.
- [Google Scholar]
- Tobacco use among students in the eight North-Eastern states of India. Indian J Cancer. 2003;40:43-59.
- [Google Scholar]
- Tobacco use among school students in Goa, India. Indian J Public Health. 2004;48:147-52.
- [Google Scholar]
- Racial/ethnic differences in cigarette smoking initiation and progression to daily smoking: a multilevel analysis. Am J Public Health. 2004;94:128-35.
- [Google Scholar]
- A study on the prevalence of alcohol consumption, tobacco use and sexual behaviour among adolescents in urban areas of the Udupi District, Karnataka, India. Sultan Qaboos Univ Med J. 2014;14:e104-12.
- [Google Scholar]
- Attention deficit hyperactivity disorder symptoms predict nicotine dependence and progression to regular smoking from adolescence to young adulthood. J Pediatr Psychol. 2007;32:1203-13.
- [Google Scholar]
- Comorbid psychopathology in adolescents and young adults treated for substance use disorders: a review. Eur Child Adolesc Psychiatry. 2006;15:319-28.
- [Google Scholar]
- The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): development, reliability and feasibility. Addiction. 2002;97:1183-94.
- [Google Scholar]
- Psychiatric comorbidities in adolescent substance use disorders. In: Rosner R, ed. Clinical handbook of adolescent addiction. Oxford: John Wiley and Sons; 2013.
- [Google Scholar]
- Interpreting scores on the Kessler psychological distress scale (K10) Aust N Z J Public Health. 2001;25:494-7.
- [Google Scholar]
- Suicidal behaviour questionnaire (SBQ-14) – Pretreatment. Seattle: University of Washington; 1997.
- ISPCAN Child Abuse Screening Tool Children's Version (ICAST-C): instrument development and multi-national pilot testing. Child Abuse Negl. 2009;33:833-41.
- [Google Scholar]
- Childhood symptoms. Barkley adult ADHD rating scale-IV (BAARS-IV). New York: Guilford Press; 2011.
- Building and applying logistic regression models. Categorical Data Analysis. New Jersey: Wiley Online Library; 2002. p. :211-66.
- Cigarettes and other Tobacco products (Prohibition of Advertisement and Regulation of Trade and Commerce, Production Supply and Distribution) Act, 2003 (COTPA) No. 34. 2003
- [Google Scholar]
- Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) Drug Alcohol Depend. 2011;115:120-30.
- [Google Scholar]
- Trajectories of substance use disorders in youth: identifying and predicting group memberships. J Child Adolesc Subst Abuse. 2010;19:135-57.
- [Google Scholar]
- Nicotine dependence and problem behaviors among urban South African adolescents. J Behav Med. 2010;33:101-9.
- [Google Scholar]
- Drug abuse among street children in Bangalore. In: A project in collaboration between NIMHANS, Bangalore and the Bangalore Forum for street and working children, Monograph funded by CRY. Bengaluru: NIMHANS; 1998.
- [Google Scholar]




