
Translate this page into:
Prevalence, clinical & biochemical correlates of non-alcoholic fatty liver disease in overweight adolescents
For correspondence: Prof. Vandana Jain, Division of Pediatric Endocrinology, Department of Pediatrics, All India Institute of Medical Sciences, New Delhi 110 029, India e-mail: drvandanajain@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Non-alcoholic fatty liver disease (NAFLD) characterized by excessive accumulation of fat in the liver, which can progress to inflammation, and cirrhosis, has emerged as an important complication of obesity in adults as well as children. This study was undertaken to assess the prevalence of NAFLD and its correlation with clinical and biochemical parameters in overweight Indian adolescents.
Methods:
In this cross-sectional study, 218 overweight adolescents aged 10 to 16 yr and their parents were included. Measurements included anthropometry, ultrasonography to diagnose NAFLD, fasting glucose, aspartate aminotransferase (AST), alanine aminotransferase (ALT) and lipids for adolescents and parents, and additional parameters of blood pressure, body fat percentage (BF%), fasting insulin, apolipoprotein C3, tumour necrosis factor-α and adiponectin for adolescents. The variables were compared between adolescents with and without NAFLD, and logistic regression analysis was performed.
Results:
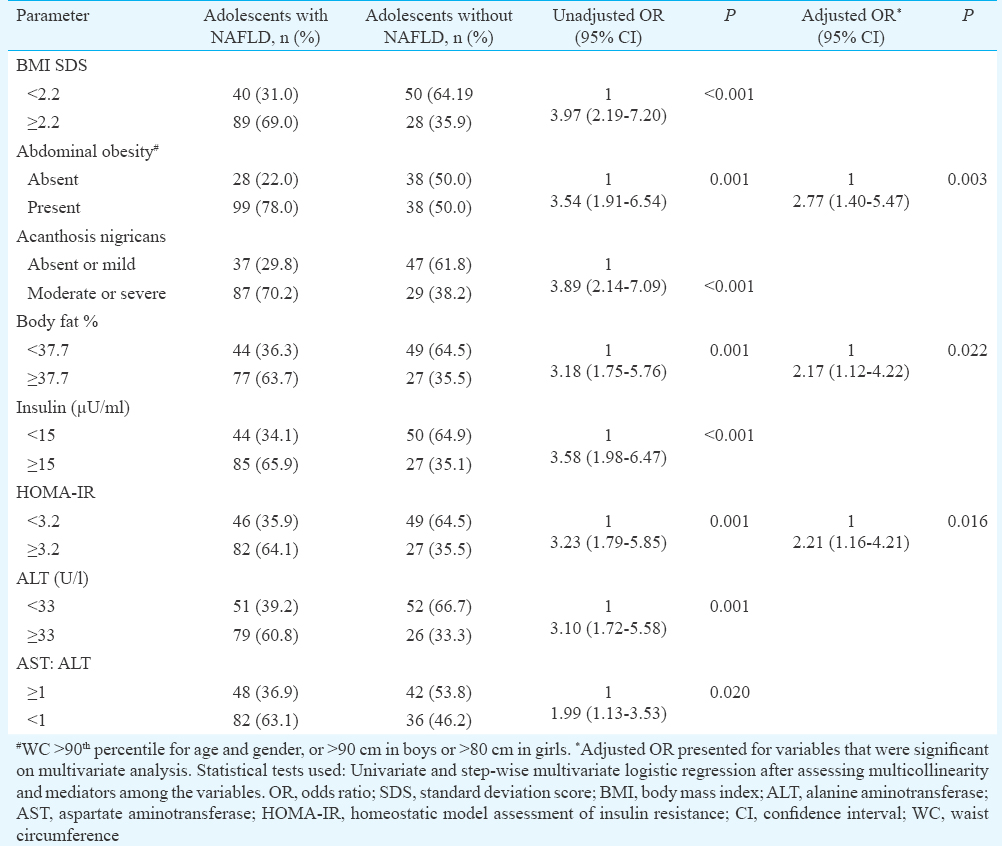
Mean age and body mass index (BMI)SD score (SDS) were 11.9±1.6 yr and 2.3±1.1, respectively. NAFLD was seen in 62.5 per cent of the adolescents. The prevalence of NAFLD in the parents was similar among the adolescents with and without NAFLD, while BMI and waist circumference SDS, BF per cent, blood pressure (BP), ALT, AST, insulin and homeostatic model assessment of insulin resistance (HOMA-IR) were significantly higher in the adolescents with NAFLD. On multiple logistic regression, abdominal obesity, HOMA-IR and BF per cent were independently associated with NAFLD with odds ratios (95% confidence interval) of 2.77 (1.40-5.47), 2.21 (1.16-4.21) and 2.17 (1.12-4.22), respectively.
Interpretation & conclusions:
NAFLD was noted among nearly two-thirds of the overweight adolescents. An independent association was observed between abdominal obesity, HOMA-IR and body fat percentage and NAFLD in overweight adolescents.
Keywords
Abdominal obesity
alanine aminotransferase
body fat percentage
childhood obesity
insulin resistance
steatohepatitis

The developing world while still struggling to devise ways and means of reducing the burden of childhood undernutrition has been thrown unprepared into the midst of the epidemic of childhood obesity. Up to 18 per cent of urban children and adolescents in the Indian subcontinent are overweight or obese1. Previous studies in overweight and obese Indian adolescents have documented a high prevalence of insulin resistance, hypertension and metabolic syndrome23.
Non-alcoholic fatty liver disease (NAFLD), characterized by the accumulation of fat in the liver without a history of alcoholism or known liver pathology, has emerged as an important health problem in India, with an overall prevalence of 9-32 per cent among adults, being higher in those who are overweight and/or diabetic4. The spectrum of NAFLD ranges from simple steatosis through steatohepatitis to advanced fibrosis and cirrhosis4. With an estimated mean prevalence in the general paediatric population of 7.6 per cent and in obese children of 34.2 per cent5, NAFLD is considered the most common cause of liver disease in paediatric population in the developed world5. Children with NAFLD have a high prevalence of concomitant metabolic syndrome, increased risk for developing type 2 diabetes, and progression to end-stage liver disease5. There is, however, a scarcity of data regarding the prevalence and determinants of susceptibility to NAFLD in paediatric age group in India. Recently, a study in 100 overweight/ obese adolescents from a Mumbai school reported NAFLD in 62 per cent6.
We undertook the present study to assess the prevalence of NAFLD and gain an insight into the clinical and biochemical parameters, such as age, gender, pubertal status, body mass index (BMI), central adiposity, body fat per cent, serum insulin, transaminases, lipid profile, adiponectin and tumour necrosis factor (TNF)-α; and the prevalence of obesity and fatty liver in parents, that may be associated with a higher risk of NAFLD in overweight/obese adolescents.
Material & Methods
This cross-sectional study was undertaken at the department of Paediatrics, All India Institute of Medical Sciences, New Delhi, India, between November 2012 and October 2015. The study was approved by the Institutional Ethics Committee. There were no data on the prevalence of NAFLD in Indian overweight adolescents when we commenced the study. In overweight adolescents from other countries, the prevalence ranged from 30-50 per cent789. A sample size of 196 was estimated taking prevalence as 50 per cent, with 95 per cent level of confidence and absolute precision of seven per cent. Adolescents aged 10-16 yr with BMI >85th percentile10 who presented to the paediatric OPD during the first two years of the study were approached. Those with obesity caused by endocrine or genetic disorders, and those with previously diagnosed diabetes mellitus or chronic liver disease were excluded. Both parents of all the enrolled adolescents were also invited to participate. Written informed consent from parents and assent from the adolescents were taken.
General information, anthropometry and body composition: Socio-economic status (assessed by modified Kuppuswamy scale) and demographic information, dietary intake, physical activity and family history of obesity, diabetes or liver disease were recorded. Blood pressure (BP) was measured using an automated BP instrument (Omron HEM-7203, Kyoto, Japan). Weight and height were measured to the nearest 0.1 kg and 0.5 cm, respectively and BMI calculated. Waist (WC) and hip circumferences (HC) were measured using non-stretchable tape according to WHO guidelines11, and waist to HC ratio (WHR) was calculated. Skinfold thickness was measured at biceps, triceps, mid-thigh, subscapular and supra-iliac regions using Holtain's skinfold calipers (Holtain Ltd, Crymych, UK). The anthropometric measurements were converted to standard deviation scores (SDS) based on Indian reference data1012. Tanner staging was done, and the adolescents were grouped into prepubertal, early pubertal (stage 2 and 3) and late pubertal (stage 4 and 5). Acanthosis nigricans over the neck was classified as absent, mild (if visible on close visual inspection and limited to the base of skull), and moderate-to-severe (if extending to lateral margins of the neck or further anteriorly)13. Body fat percentage was measured using bioelectrical impedance analysis (Maltron BF-907, Essex, UK).
Biochemistry: Fasting venous sample (5 ml) was obtained after a 12 h overnight fast for estimation of alanine aminotransferase (ALT), aspartate aminotransferase (AST), glucose, insulin, triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL), apolipoprotein C3, TNF-α and adiponectin levels. Modified oral glucose tolerance test was done by administering oral glucose at 1.75 g/kg (maximum 75 g) and taking a repeat blood sample after two hours. ALT, AST and glucose were estimated by Roche automated clinical analyzer; TG, TC and HDL by Randox kits (Randox Ltd, Antrim, United Kingdom), and Insulin by electrochemiluminescence (Roche Cobas e411, Roche Diagnostics Germany GmbH). Commercial enzyme-linked immunosorbent assay kits were used to measure TNF-α (Diaclone, Besancon Cedex, France), apolipoprotein C3 (Assaypro St. Charles, USA), and adiponectin (R&D, Minneapolis, USA). Homeostatic model assessment of insulin resistance (HOMA-IR) was calculated as fasting insulin (μU/ml) × fasting glucose (mmol/l)/22.5. Low-density lipoprotein cholesterol (LDL) was calculated using Friedewald's equation14.
Diagnosis of non-alcoholic fatty liver disease (NAFLD): The diagnosis of NAFLD was based on ultrasonography (USG), performed using curvilinear probe (2-5 Hz) of Acuson S2000 (Siemens, Germany). Fatty liver was diagnosed and graded as mild, moderate and severe based on echogenicity, visualization of vasculature, parenchyma and diaphragm15. In adolescents with fatty liver, hepatitis B surface antigen (HBsAg) and anti-hepatitis C virus (HCV) antibodies were assayed using electrochemiluminescence (Roche Cobas e411, Roche Diagnostics Germany GmbH).
Parents' data: Parents' age was recorded, and height and weight measured. Fasting venous samples were collected for ALT, AST, lipid profile and glucose; USG was performed to diagnose and grade fatty liver.
Definitions: WC was considered high if >90th percentile for Indian adolescents12, or more than the adult cut-offs of 90 and 80 cm for Asian males and females, respectively16. WHR was considered to be high if >0.95 for boys and >0.85 for girls17. Hypertension was diagnosed at systolic BP ≥130 mmHg and /or diastolic BP ≥85 mmHg18. Elevated ALT was defined as >26 U/l for boys and >23 U/l for girls19. Parents were considered overweight and obese at BMI ≥23 and ≥25 kg/m2, respectively20. Fasting and two hours blood glucose were considered elevated if ≥100 and 140 mg/dl, respectively21, and HOMA-IR was considered high if >2.522. TG was considered high if ≥150 mg/dl; HDL was considered low if < 40mg/dl in adolescents of either gender, and fathers, and <50 mg/dl in mothers1618. TC and LDL cholesterol were considered elevated if >200 and 130 mg/dl, respectively23. Metabolic syndrome in adolescents was diagnosed using the International Diabetes Federation criteria18.
Statistical analysis: Data were analyzed by Stata 11.2 (Stata Corp 4905 College Station, Texas 47845 USA) and presented as mean±SD, median (range) or frequency (percentage). Parameters of the adolescents with and without NAFLD were compared using Chi-square test or Fisher's exact test for categorical variables, one-way ANOVA or independent t test for continuous variables following normal distribution, and Kruskal-Wallis or Wilcoxon rank sum test for parameters following non-normal distribution. Receiver operating characteristic (ROC) curves were generated to identify the cut-offs for various parameters for association with NAFLD. Univariate and step-wise multivariate logistic regression was used to calculate unadjusted and adjusted odds ratios after assessing multicollinearity and mediators among the variables.
Results
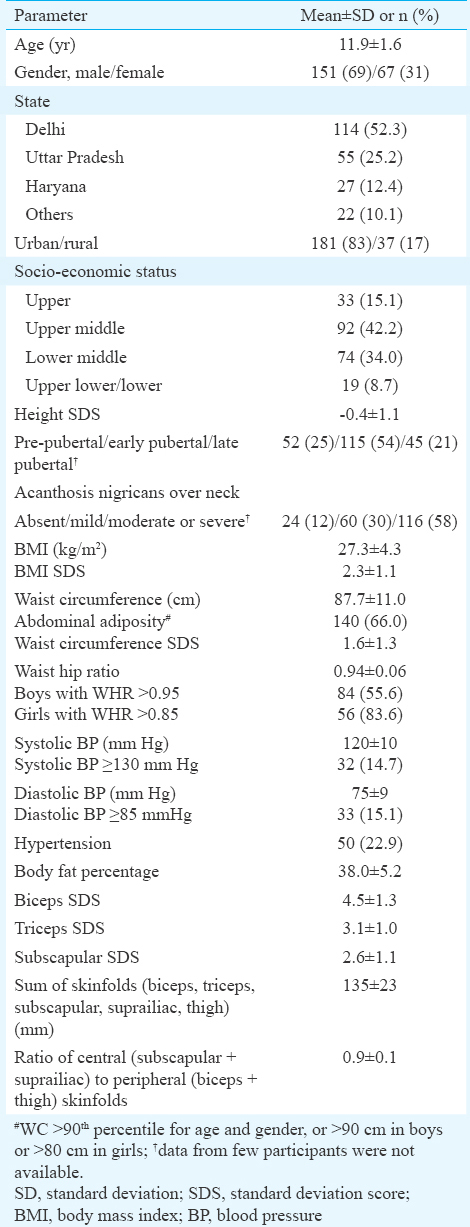
Clinical, demographic and anthropometric parameters of the adolescents: A total of 218 adolescents and their parents were included in the study. Mean age of the adolescents was 11.9±1.6 yr. Mean BMI SDS was 2.3±1.1; 52 (23.9%) were overweight, and 166 (76.2%) were obese. Acanthosis nigricans was present in 88 per cent, abdominal obesity in 66 per cent and hypertension in 22.9 per cent (Table I).
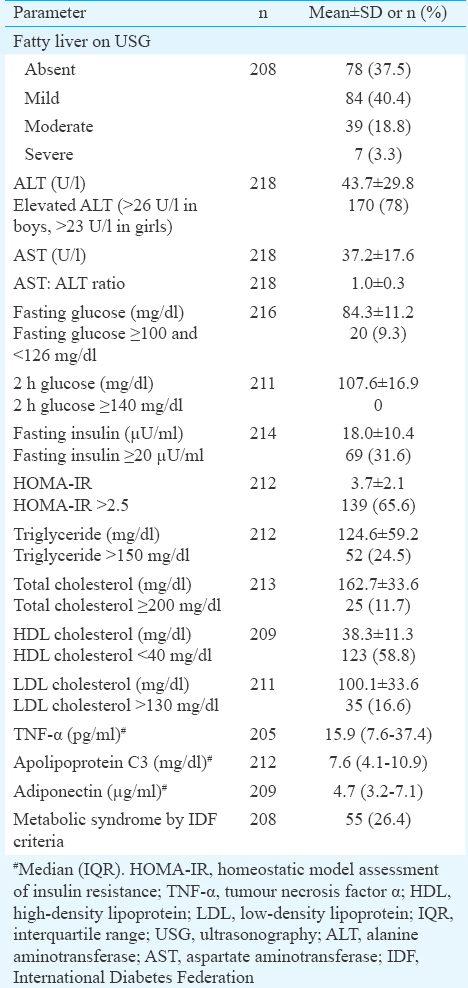
Radiological and biochemical profile of the adolescents: NAFLD was present in 130 (62.5%) of the adolescents [95% confidence interval (CI) 56.2-69.4%], and serum ALT was elevated in 78 per cent. Among the other metabolic derangements, elevated HOMA-IR and low HDL were the commonest, noted in 65.6 and 58.8 per cent, respectively. Metabolic syndrome was present in 26.4 per cent (Table II). None of the adolescents with fatty liver or elevated ALT had positive HBsAg or anti-HCV antibody test.
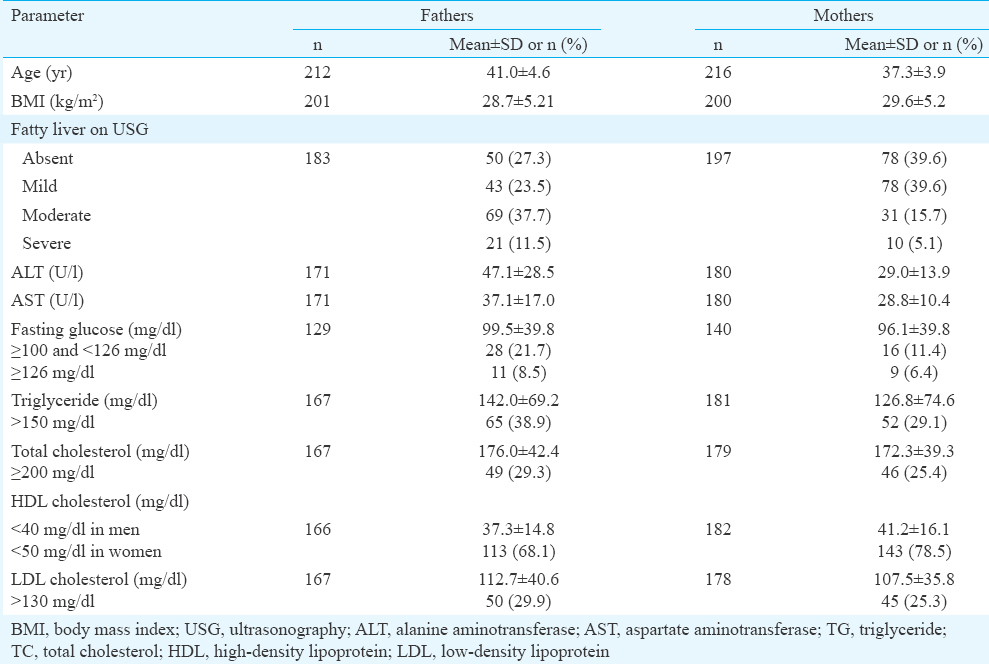
Clinical, radiological and biochemical parameters in the parents: Overweight/obesity was present in 90.6 per cent of the fathers and 90.5 per cent of the mothers. Diabetes was present in 8.5 and 6.4 per cent of fathers and mothers, respectively. Fatty liver was observed in 72.7 and 60.6 per cent of the fathers and mothers, respectively (Table III). Moderate and severe fatty liver was commoner among fathers compared to mothers. The most common dyslipidemia was low HDL.
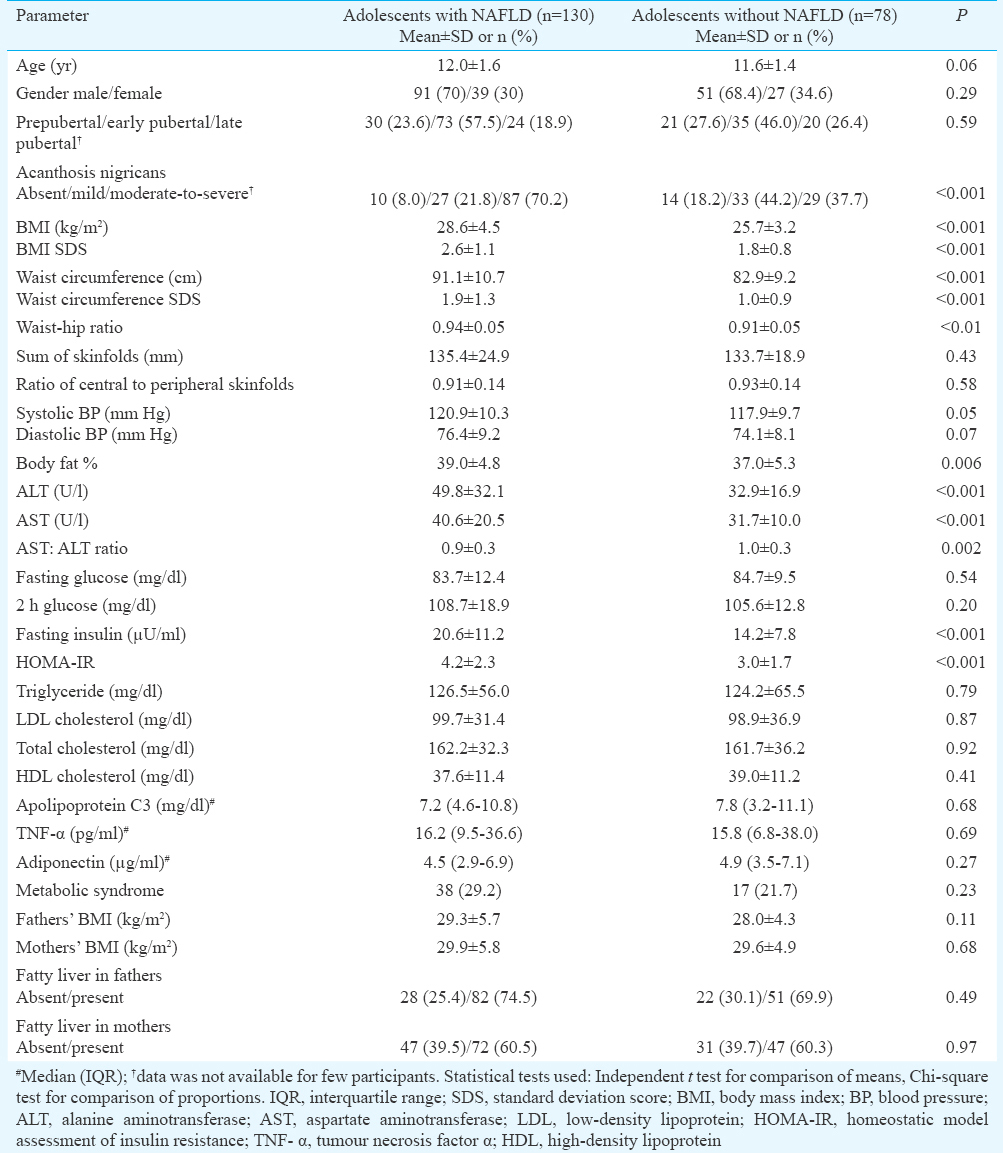
Comparison among adolescents with and without NAFLD: The comparison of the clinical and biochemical parameters in the adolescents with and without fatty liver is presented in Table IV. Age, distribution of gender and pubertal status and socio-demographic profile were similar in the two groups. BMI SDS, WC SDS, WHR, BP, FM per cent, ALT, AST, fasting insulin, HOMA-IR and prevalence of acanthosis nigricans were higher in the adolescents with NAFLD compared to those without NAFLD. Parents' mean BMI as well as the proportion of parents who had fatty liver was similar in both the groups.
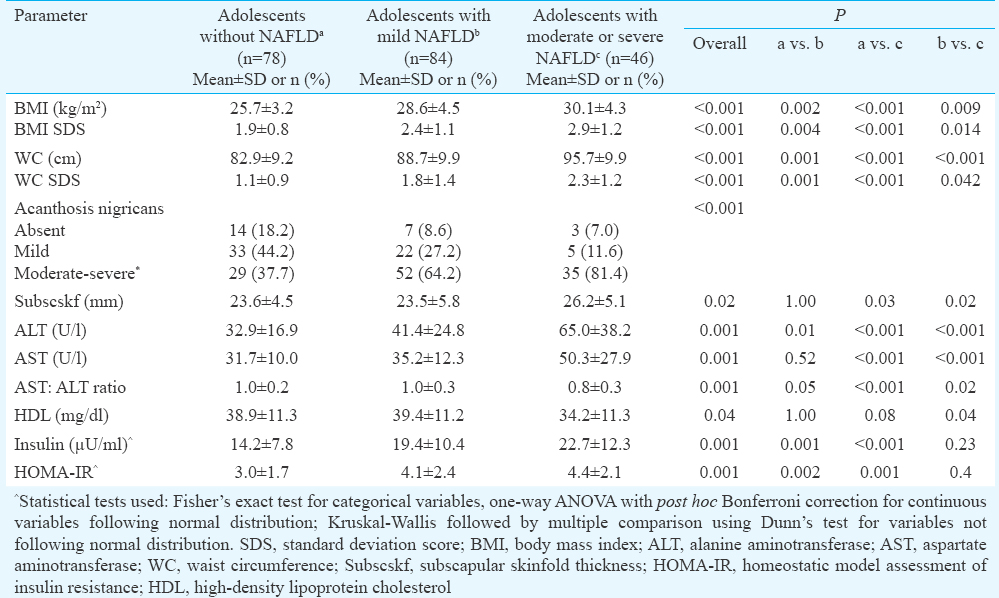
The anthropometric and biochemical parameters were further compared between the adolescents without NAFLD (n=130), with mild NAFLD (n=84) and with moderate or severe NAFLD (n=46). The parameters that were significantly different among the adolescents in these three groups are presented in Table V. A clear gradation of BMI, WC, acanthosis nigricans, ALT, AST, fasting insulin and HOMA-IR was observed across the three groups, elucidating further the association between severity of obesity, insulin resistance and NAFLD. Subscapular skinfold thickness, a measure of central adiposity was higher and HDL significantly lower among the adolescents with moderate or severe NAFLD as compared to those with mild NAFLD. Mean serum adiponectin in adolescents with moderate or severe NAFLD (4.9±3.8 μg/ml) was lower compared to those without NAFLD (5.5±3.1 μg/ml, P=0.08).
Receiver operating characteristic (ROC) and regression analysis: ROC analysis was performed to obtain the cut-offs of anthropometric and biochemical parameters for predicting a higher risk for NAFLD. WC SDS had the highest discriminating ability, with area under the curve (AUC) of 0.73 (95% CI 0.66-0.80), and the cut-off being 1.4 sensitivity 70.1% and specificity 70.6%). This was followed by ALT ≥33 U/l (AUC ROC 0.70; 95% CI 0.63-0.77, sensitivity 60.8% and specificity 66.2%); BMI SDS ≥2.2 (AUC ROC 0.70; 95% CI 0.62-0.76, sensitivity 69% and specificity 63.6%); insulin ≥15 μU/ml (AUC ROC 0.68; 95% CI 0.61-0.76, sensitivity 67.4%, specificity 64.9%), HOMA-IR ≥3.2 (AUC ROC 0.67; 95% CI 0.59-0.74, sensitivity 64% and specificity 64.5%) (Figure) and body fat per cent ≥37.7 (AUC ROC of 0.63; 95% CI 0.55-0.71, sensitivity 63.6% and specificity 64.0%).
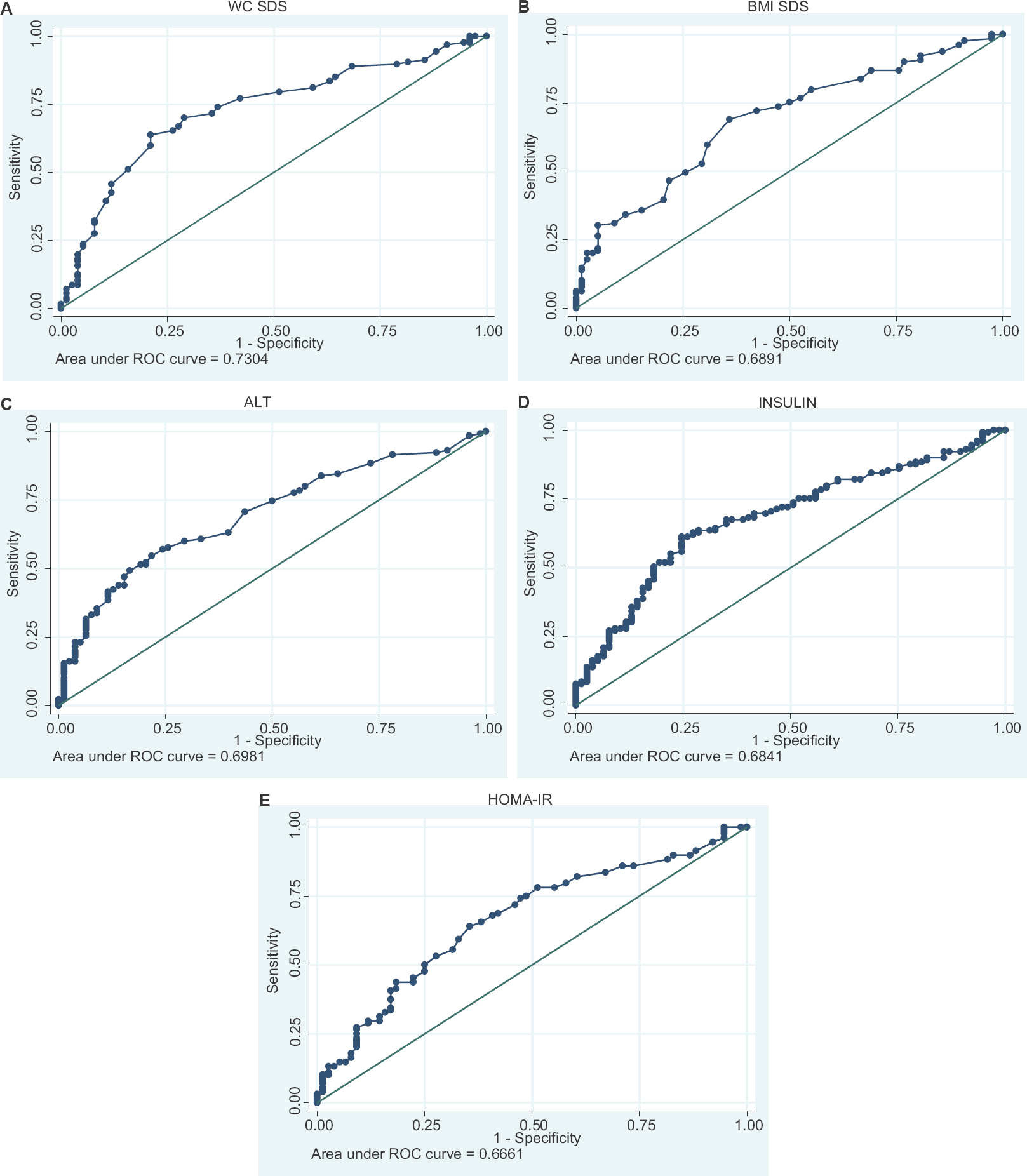
- Receiver operating characteristic (ROC) curves to identify the cut-offs for various parameters (A) Waist circumference standard deviation scores (WC SDS), (B) body mass index standard deviation scores (BMI SDS), (C) alanine aminotransferase (ALT), (D) insulin, (E) homeostatic model assessment of insulin resistance (HOMA-IR) for association with non-alcoholic fatty liver disease.
Association of various parameters with NAFLD was checked by univariate followed by multiple logistic regression analysis. Abdominal obesity, HOMA-IR and body fat percentage (BF%) emerged as significant independent variables that were associated with NAFLD (Table VI).
Discussion
A high prevalence of NAFLD (62.5%) was observed in the overweight/obese adolescents in our study. BMI, WC, BF per cent, insulin resistance and levels of ALT and AST were positively associated with a higher risk of NAFLD. The presence of obesity and/or fatty liver in parents was not associated with a higher prevalence of NAFLD in the adolescents. WC SDS ≥1.4, BMI SDS ≥2.2, ALT ≥33 U/l, insulin ≥15 μU/ml and HOMA-IR ≥3.2 were identified as cut-offs predictive of higher risk for NAFLD.
In previous studies in overweight children and adolescents, the prevalence of NAFLD has ranged from about 30 per cent in studies from Europe7 to about 45-50 per cent in studies from China9 and Turkey8. In another study in Indian overweight adolescents, a similarly high prevalence has been reported6. Earlier studies have indicated an ethnic difference in the prevalence of NAFLD, with Hispanic adolescents being at the highest risk and Africans the least24. Our observations suggest a higher predilection for NAFLD in Asian Indian adolescents.
Asian Indians have a high prevalence of central adiposity and insulin resistance beginning at a young age, with clustering of cardiometabolic risk markers including high body fat percentage dyslipidaemia and fasting glucose225. The present study places NAFLD as a prominent member of the cluster of complications associated with central adiposity and insulin resistance in Indian adolescents. Considering that India is home to 243 million adolescents, more than 20 per cent of the world's adolescent population26, up to 25 million of whom are overweight, this high prevalence of NAFLD has a huge potential implication for our health infrastructure and resources.
Among the fathers and mothers, majority of whom were overweight/obese, the prevalence of fatty liver was 72.3 and 60.4 per cent, respectively. This was similar to the prevalence of 72.3 per cent reported among overweight/obese adults from Chennai27. We did not find any difference in the prevalence of NAFLD in our study participants based on their age, pubertal stage or gender. Among parents, the prevalence, as well as the severity of NAFLD, was higher among fathers as compared to mothers. This is in agreement with previous literature suggesting that male gender is associated with a higher prevalence of NAFLD, while estradiol affords some protection in females28. Our results indicated that in adolescents, both genders were at similar risk of NAFLD. Higher BMI and WC SDS were significantly associated with NAFLD in the present study, as reported in several earlier studies78. Presence and severity of acanthosis nigricans were also observed to be significantly higher in the adolescents with NAFLD compared to those without, thus indicating its usefulness as a clinical risk marker for complications of obesity.
In the present study, fasting and two hours glucose, triglyceride, total and LDL cholesterol and apolipoprotein C3 were similar in the adolescents with and without NAFLD. HDL cholesterol was lower in the adolescents with moderate or severe NAFLD compared to those with mild NAFLD. In a previous study on paediatric population, higher levels of LDL-C, TG, TC and apolipoprotein C329 have been found to be independent predictors of NAFLD. Cytokines and inflammatory mediators are considered important in the pathogenesis and progression of NAFLD30. Adiponectin has insulin-sensitizing effects and has been reported to be lower in obese children and adults with NAFLD compared to those without NAFLD30. In the present study, adiponectin was lower among the children with moderate or severe NAFLD as compared to those with mild or no NAFLD, but no such difference was noted for TNF-α.
The strength of the present study was that a reasonably large number of adolescents and both their parents were evaluated clinically, biochemically and by USG. The limitations were that the prevalence of NAFLD was not assessed in lean adolescent controls, and the diagnosis of NAFLD was not confirmed by more robust methods such as magnetic resonance imaging (MRI) or histology.
In conclusion, our results showed NAFLD in nearly two-thirds of the overweight adolescents. The clinical and biochemical parameters associated with higher risk for NAFLD were higher BMI and WC, the presence of acanthosis nigricans, and elevated ALT and HOMA-IR. Screening for NAFLD should be incorporated in the evaluation of all overweight adolescents, especially if one or more of the risk markers are present.
Acknowledgment:
Authors acknowledge the help from Shri Brijesh Kumar in performing the ECLIA based laboratory assays, and Ms. Shruti Adhikari in enrolment of participants.
Financial support & sponsorship: This study was funded by Indian Council of Medical Research, New Delhi (Ref. No. 5/4/3-1/TF/2012/NCD-II).
Conflicts of Interest: None.
References
- Prevalence of overweight and obesity among children and adolescents of the Indian subcontinent: A meta-analysis. Nutr Rev. 2014;72:541-50.
- [Google Scholar]
- Prevalence of metabolic syndrome in adolescents from a North Indian population. Diabet Med. 2007;24:195-9.
- [Google Scholar]
- Nonalcoholic fatty liver disease in India - A lot done, yet more required! Indian J Gastroenterol. 2010;29:217-25.
- [Google Scholar]
- The prevalence of non-alcoholic fatty liver disease in children and adolescents: a systematic review and meta-analysis. PLoS One. 2015;10:e0140908.
- [Google Scholar]
- Most overweight and obese Indian children have nonalcoholic fatty liver disease. Ann Hepatol. 2016;15:853-61.
- [Google Scholar]
- Thyroid dysfunction and hepatic steatosis in overweight children and adolescents. Pediatr Obes. 2017;12:67-74.
- [Google Scholar]
- Non-alcoholic fatty liver disease in obese children and the relationship between metabolic syndrome criteria. Obes Res Clin Pract. 2014;8:e356-63.
- [Google Scholar]
- Prevalence of nonalcoholic fatty liver disease and metabolic abnormalities in 387 obese children and adolescents in Beijing, China. Zhonghua Liu Xing Bing Xue Za Zhi. 2013;34:446-50.
- [Google Scholar]
- World Health Organization. WHO STEPS surveillance manual: The WHO STEPwise approach to chronic disease risk factor surveillance. Geneva: World Health Organization; 2005.
- Waist circumference percentiles in 2-18 year old Indian children. J Pediatr. 2014;164:1358-62.
- [Google Scholar]
- Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499-502.
- [Google Scholar]
- Ultrasonographic quantitative estimation of hepatic steatosis in children with NAFLD. J Pediatr Gastroenterol Nutr. 2011;53:190-5.
- [Google Scholar]
- Metabolic syndrome - A new world-wide definition. A consensus statement from the international diabetes federation. Diabet Med. 2006;23:469-80.
- [Google Scholar]
- The optimal cutoff values and their performance of waist circumference and waist-to-hip ratio for diagnosing type II diabetes. Eur J Clin Nutr. 2010;64:23-9.
- [Google Scholar]
- International diabetic federation: Criterion of metabolic syndrome in children and adolescents. J Pediatr. 2004;145:439-44.
- [Google Scholar]
- Safety study: Alanine aminotransferase cut-off values are set too high for reliable detection of pediatric chronic liver disease. Gastroenterology. 2010;138:1357-64. 1364e1-2
- [Google Scholar]
- Ethnic-specific criteria for classification of body mass index: A perspective for Asian Indians and American Diabetes Association position statement. Diabetes Technol Ther. 2015;17:667-71.
- [Google Scholar]
- Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-90.
- [Google Scholar]
- A study of insulin resistance by HOMA-IR and its cut-off value to identify metabolic syndrome in urban Indian adolescents. J Clin Res Pediatr Endocrinol. 2013;5:245-51.
- [Google Scholar]
- National cholesterol education program report of the expert panel on blood cholesterol levels in children and adolescents. Pediatrics. 1992;89:525-84.
- [Google Scholar]
- Pediatric fatty liver disease: Role of ethnicity and genetics. World J Gastroenterol. 2014;20:7347-55.
- [Google Scholar]
- Insulin resistance and clustering of cardiometabolic risk factors in urban teenagers in Southern India. Diabetes Care. 2007;30:1828-33.
- [Google Scholar]
- Adolescent health: Present status and its related programmes in India? Are we in the right direction. J Clin Diagn Res. 2015;9:LE01-6.
- [Google Scholar]
- Comparison of characteristics between nonobese and overweight/obese subjects with nonalcoholic fatty liver disease in a South Indian population. Diabetes Technol Ther. 2014;16:48-55.
- [Google Scholar]
- Gender-specific prevalencesof fatty liver in obese children and adolescents: Roles of body fat distribution, sex steroids, and insulin resistance. J Clin Endocrinol Metab. 2009;94:3872-81.
- [Google Scholar]
- Adipocyte cell size, free fatty acids and apolipoproteins are associated with non-alcoholic liver injury progression in severely obese patients. Metabolism. 2014;63:1542-52.
- [Google Scholar]
- Association of hypoadiponectinemia with non-alcoholic fatty liver disease in urban South Indians -(CURES - 81) Indian J Med Res. 2010;132:271-7.
- [Google Scholar]




