
Translate this page into:
Phlebolith with dyspnoea
*For correspondence: meghna.vasanth@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 45 yr old male† presented to the Emergency department of Apollo First Med Hospitals, Chennai, India, in September 2017, with progressive dyspnoea over two months. He had type-1 respiratory failure. Examination revealed a soft-tissue swelling over the posterior aspect of the right chest wall. Echocardiogram showed severe pulmonary artery hypertension. Computed tomography chest with pulmonary angiogram showed extensive phleboliths in the chest and abdomen region (Figure A) with soft-tissue haemangiomata in the chest wall (Figure B) and acute-on-chronic pulmonary embolism (Figure C). He was started on oral anticoagulation with rivaroxaban after the diagnosis in the same admission and continued till April 2019 and showed clinical improvement. This is a rare case of Klippel-Trenaunay syndrome. It is a congenital condition associated with soft-tissue hypertrophy and vascular malformations. The patient was on regular follow up on until April 2019. He had clinical improvement except for minimal dyspnea on exertion. His repeat CT in April 2019 showed chronic pulmonary thromboembolism predominantly in the right lung.
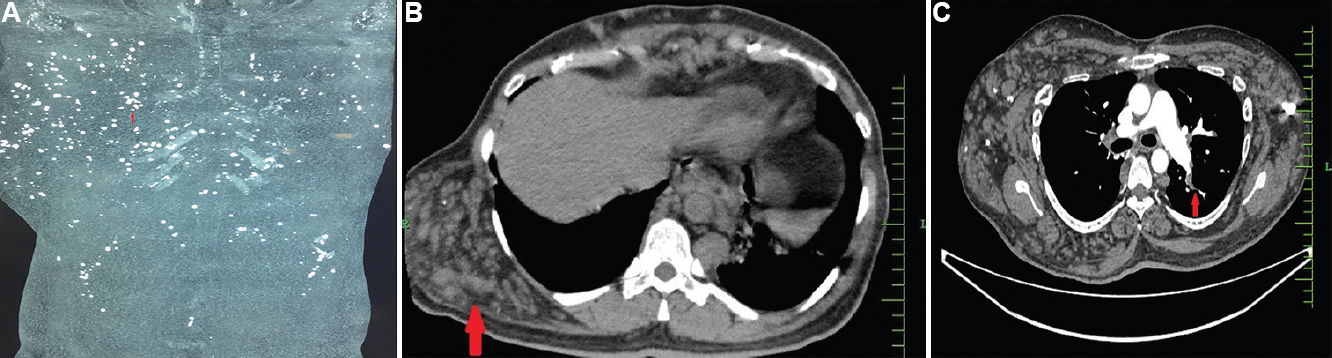
- (A) CT chest with pulmonary angiogram showed extensive phleboliths in the chest and abdomen (arrow). (B) Haemangiomata over the right posterolateral chest wall (arrow) in CTPA. (C) Thrombus in the left lobar pulmonary artery (arrow).
Conflicts of Interest: None.




