
Translate this page into:
Peripilar keratin cysts or pseudonits: When nits are not nits!
*For correspondence: vkm1@rediffmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 19 yr old girl presented to the Dermatology Outpatient Clinic of Dr. R. P. Government Medical College, Kangra (Tanda), Himachal Pradesh, India, in April 2015, with whitish cylindrical nits-like structures of variable sizes encircling scalp hair shafts (Fig. 1) for the past 5-6 months. Their removal by washing or combing and treatments for pediculosis was unsuccessful. She did not have seborrhoeic dermatitis or pediculosis capitis. KOH mounts showed no fungus. A diagnosis of peripilar keratin cystswas made after light microscopy and dermatoscopic examination (Fig. 2). Tretinoin 0.025 per cent solution application overnight, shampooing and combing next morning for two weeks was useful, after that she did not come for follow up.

- Naked eye examination showing peripilar keratin cysts as multiple discrete firm, shiny, 2-7 mm long, white tubular accretions encircling hair on vertex/frontal scalp at variable lengths from the scalp.
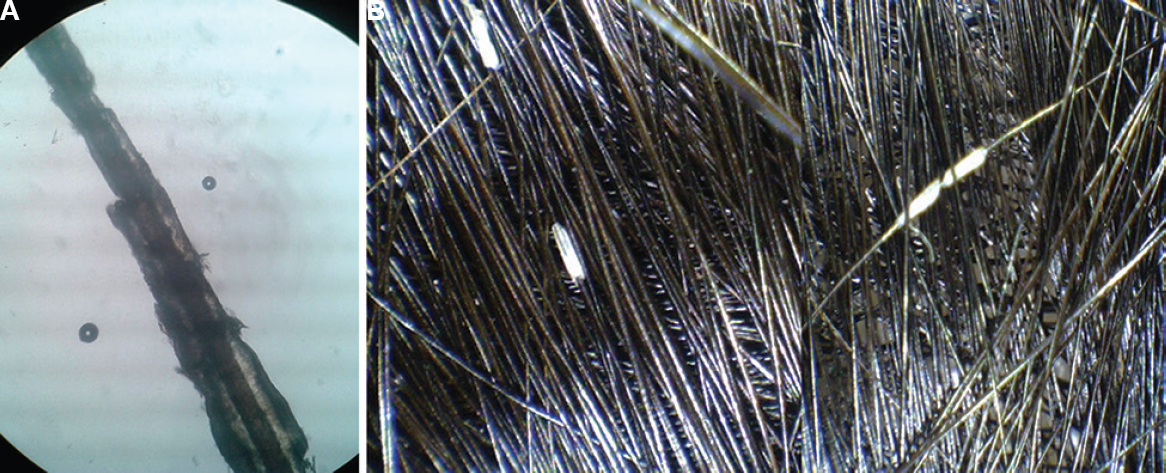
- (A) Peripilar keratin cysts as seen under light microscopy in saline mount. These can be missed in KOH mount as these are dissolved (B) Amorphous whitish tubular structure of peripilar keratin cysts of variable lengths encircling the hair shaft on dermoscopy.
Pseudonits resembling lice/nits cause significant psychosocial embarrassmentin children/adolescents. These are often idiopathic/primary or secondary to seborrhoeic dermatitis, psoriasis or excessive traction. Treatment with topical retinoic acid (0.025%) solution and keratolytic/tar shampoos and physical removal become imperative to prevent embarrassment, but recurrences are usual.




