
Translate this page into:
Perioperative time course of matrix metalloproteinase-9 (MMP-9), its tissue inhibitor TIMP-1 & S100B protein in carotid surgery
Reprint requests: Dr Diana Mühl, Department of Anesthesiology & Intensive Therapy, University of Pécs, Hungary e-mail: drdianamuhl@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Ischaemic stroke is a life burdening disease for which carotid endarterectomy (CEA) is considered a gold standard intervention. Pro-inflammatory markers like matrix metalloproteinases (MMPs) and their inhibitors (TIMPs) and S-100 Beta (S100B) may have a role in the early inflammation and cognitive decline following CEA. This study was aimed to describe the perioperative time courses and correlations between of MMP-9, TIMP-1 and S100B following CEA.
Methods:
Fifty four patients scheduled for CEA were enrolled. Blood samples were collected at four time points, T1: preoperative, T2: 60 min after cross-clamp release, T3: first postoperative morning, T4: third postoperative morning. Twenty atherosclerotic patients were included as controls. Plasma MMP-9, TIMP-1 and S100B levels were estimated by ELISA.
Results:
TIMP-1 was decreased significantly in the CEA group (P<0.01). Plasma MMP-9 was elevated and remained elevated from T1-4 in the CEA group (P<0.05) with a marked elevation in T3 compared to T1 (P<0.05). MMP-9/TIMP-1 was elevated in the CEA group and increased further by T2 and T3 (P<0.05). S100B was elevated on T2 and decreased on T3-4 compared to T1.
Interpretation & conclusions:
Our study provides information on the dynamic changes of MMP-9-TIMP-1 system and S100B in the perioperative period. Preoperative reduction of TIMP-1 might be predictive for shunt requirement but future studies are required for verification.
Keywords
Carotid surgery
matrix metalloproteinase
MMP-9
POCD
S100B
TIMP-1

Ischaemic stroke is a major healthcare problem accompanied by a high rate of long-term disability and heavy medical expense12. Stroke survivors remain at high risk of recurrent attacks especially from the common carotid bifurcation. Carotid endarterectomy (CEA) is considered to be the gold standard revascularization therapy and has a well-established role in prevention in selected patients3. According to Cochrane Collaboration data4, CEA is associated with a 30 days mortality of 1.1 per cent, and stroke incidence of 3.4 per cent. However, post-operative cognitive dysfunction (POCD) is a frequent complication (20-30%)5. Three key factors implicated in POCD after CEA are microembolization, hypoperfusion during clamping and postoperative hyperperfusion678. Many methods and biomarkers have been tested to detect impaired oxygen supply to brain cells and to predict POCD in CEA, but possibly due to the complexity of the underlying processes no ideal tests are available yet. First, central nervous system markers like neuron specific enolase and S 100 Beta (S100B) have been evaluated with conflicting results910.
Several investigators have examined matrix metalloproteinases (MMPs) and their natural occurring inhibitors (TIMPs) in CEA and CEA associated POCD111213. Enzymatic cleavage is needed to activate the MMPs before their main role in extracellular matrix (ECM) turnover, degradation and remodelling. Besides these functions, these are considered to be signaling proteases. Therefore, MMPs have been widely evaluated in many physiological and pathophysiological processes and in some their role and prognostic significance have been established14151617. Rosell et al18 assessed MMP-9 levels in stroke patients and reported increased levels of MMP-9 in perivascular tissues of the stroke core, as well as increased production by microglial cells. MMP-9 plays a crucial role in neuronal injury and brain damage19. According to a recent review20, MMP-9 may be released in response to ischaemic insult from brain cells and has been shown to be associated with complications like excitotoxicity, apoptosis, oxidative stress, blood-brain barrier opening and cerebral oedema. MMP-9 is also considered to be responsible for the detrimental effects of tissue plasminogen activator in thrombolysis. Thus, inhibition of MMP-9 is considered as a new therapeutic target20 with promising results in animal model21.
The interaction between MMPs and tissue inhibitors of metalloproteinases (TIMPs) is stoichiometric, therefore, MMP/TIMP ratios can be used to express activity. In vitro data suggest the protective role of TIMP-1 on neuronal cell death and neurotrophic action, but in vivo data are controversial, as the possibility of blood-brain barrier leakage and secondary TIMP-1 increase cannot be completely ruled out22. However, the clinical usefulness of MMP-9 and S100B in acute settings to diagnose ischaemic stroke could be limited compared to clinical parameters23.
Both the MMP-TIMP system and the S100B have already been evaluated in CEA9101112, but the perioperative time courses of these variables have not been evaluated. Therefore, the primary aim in this study was to examine the time course of CEA related changes in MMP-9, TIMP-1, and S100B levels to establish baseline data for future studies. As secondary objectives, we examined the effects of coexisting diseases, medications, cross-clamp time (CCT), demographic data, as well as intra- and post-operative complications on MMP-9, TIMP-1 and S100B levels and compared CEA group with an atherosclerotic control group.
Material & Methods
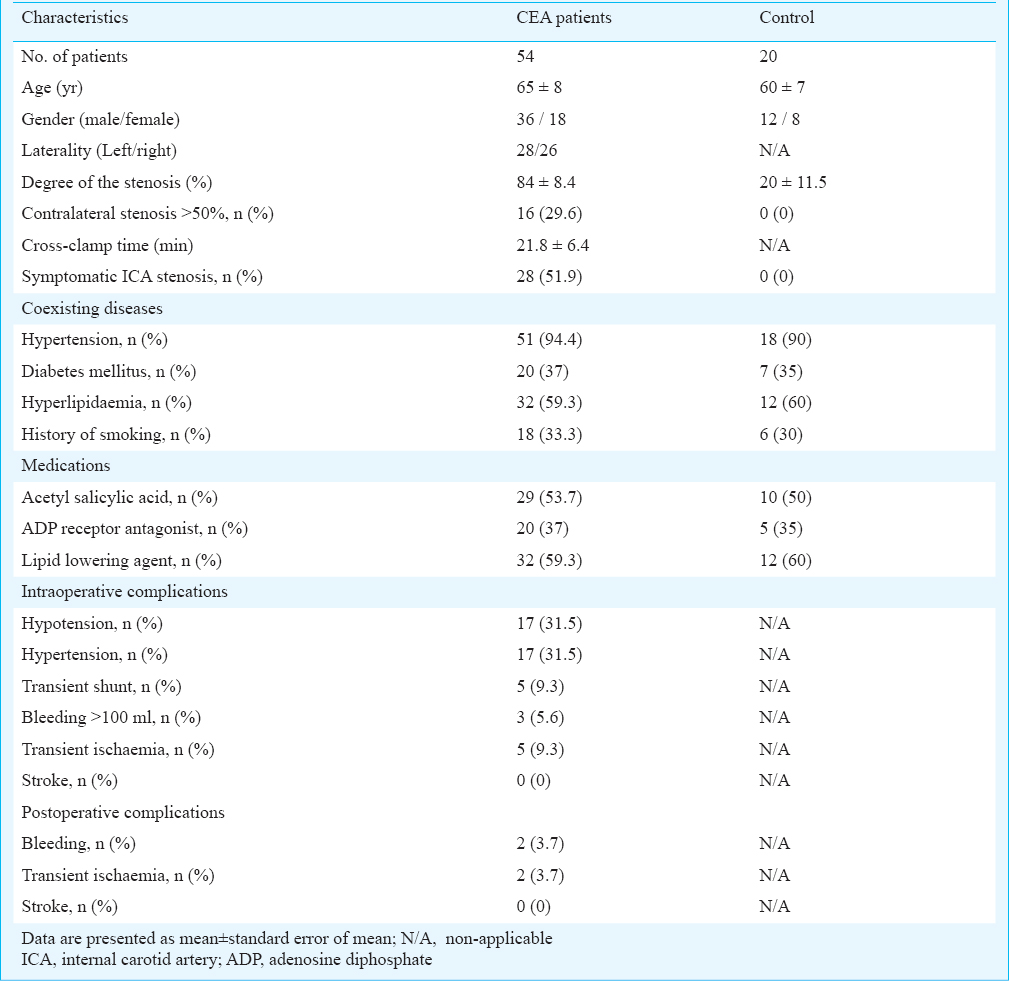
The study was carried out at the Clinical Center of University of Pécs, Hungary. The study protocol was cleared by the Institutional Scientific and Human Research Ethics Committee of the University of Pécs. All patients scheduled for elective CEA in 2012 were considered. They were included consecutively between January to December 2012. Twenty atherosclerotic patients scheduled for outpatient ophthalmological examinations were invited as controls. No significant difference was observed regarding age, gender, medications and coexisting diseases compared to the operated group, but controls were scanned with ultrasound to be free from significant carotid diseases (Table I). Controls were also free from symptoms and positive medical history regarding cerebral atherosclerosis and carotid diseases.
Patients suffering from diagnosed malignant diseases, psychiatric disorders or previous debilitating stroke were excluded. In 2012, a total of 66 patients were scheduled for elective CEA. Twelve patients were excluded as five met the exclusion criteria and seven refused to participate. Overall, 54 patients were included in the study.
Surgical procedure: Operations were performed under loco-regional anaesthesia. The anatomical landmarks based deep and superficial cervical blockade with bupivacaine and/or lidocaine and fentanyl was carried out. Occasionally, supplementary lidocaine was administered by the surgeons during the operation, especially after opening of the carotid sheath. All procedures were performed according to current guidelines and based on local protocols32425. Although receiving no premedications, patients received conscious sedation with propofol. Target blood concentrations of propofol were generally set at 0.4-1.0 μg/ml. Careful dissection and preparation were performed to decrease the incidence of cerebral embolization. Conscious level of the patients was tested by Glasgow Coma Score26, especially verbal response and motor function on the contralateral upper limb (Duck Squeezing test)27 were evaluated. Sudden loss of consciousness, aphasia or decreased motor power implied significant reduction of brain perfusion resulting in shunt placement. Cross-clamp times (CCTs) measured by stopwatch were recorded on the anaesthetist chart in seconds. Euvolemia was maintained with crystalloid (5-15 ml/kg of Isolyte, B. Braun Medical Ltd., Budapest, Hungary) and occasionally with colloid (5-10 ml/kg of Volulyte 6% 130/0.4, Fresenius Kabi Hungary Ltd., Budapest, Hungary) infusions. Supplemental oxygen via nasal cannula was given with a flow rate of 4-6 l/min. Haemodynamic stability was maintained meticulously. With optimal analgesia, any alteration of mean arterial pressure by 20 per cent for 10 min (compared to the preoperative values) was considered significant and treated with appropriate intravenous agents. Hypotension was counteracted with ephedrine (5-10 mg/bolus up to 50 mg) and/or phenylephrine (0.05-0.2 mg/bolus). Hypertension was treated most frequently with urapidil (12.5-25 mg/bolus). Hypotension accompanied by neurological symptoms was treated by the aforementioned drugs. Prior to arteriotomy, all patients received intravenous unfractionated sodium heparin (5000-7500 units). All patients were admitted to the Intensive Care Unit for postoperative care.
Blood sampling and biochemical analysis: Blood samples from CEA patients were collected via arterial line, which was inserted preoperatively for invasive blood pressure monitoring. Samples were withdrawn at four time points (T1-4), T1: right after the insertion of the arterial line, T2: 60 min after the cross-clamp release, T3: first postoperative morning, T4: third postoperative morning.
Blood samples (20 ml) were also collected from controls. Plasma S100B levels in volunteers have been well established, so we did not measure these in our controls28. Plasma was isolated from heparin anticoagulated blood samples by low speed centrifugation at 4 °C, and stored at -80 °C until analyzed in a single batch at the end of the study. MMP-9 and TIMP-1 were determined by the quantitative sandwich enzyme-linked immunosorbent assay (ELISA) techniques according to the manufacturer instructions (R&D Systems Inc., Minneapolis, MN, USA). The S100B protein concentration was measured by a commercially available ELISA kit (BioVendor L.M., A.S., Brno, Czech Republic). In comparison with standard curves, the concentrations of MMP-9, TIMP-1 and S100B in plasma were determined spectrophotometrically (Multiskan Ascent microplate photometer, Type: 354, Thermo Electron Corporation, Waltham, MA, USA) by reading the absorbance at 450 nm. Plasma concentrations of MMP-9 and TIMP-1 were expressed as ng/ml, and plasma concentrations of S100B were expressed as pg/ml.
Statistical analysis: Non-parametric tests were used since data distribution was not normal by Kolmogorov-Smirnov test. CEA patients and controls were compared with Mann-Whitney U test. Wilcoxon Signed Rank test was used to compare data of CEA group patients. Using univariate and multivariate linear regression models, the influence of many factors (coexisting diseases, medications, CCT, demographic data, intra- and post-operative complications, etc.) was evaluated on dependent variables. Also, multivariate linear regression was used to predict CCT. Using logistic multivariate regression models, the influencing factors of shunting were evaluated. Associations between quantitative variables were evaluated with Spearman correlation coefficient. The analyses were conducted by Statistical Package for the Social Sciences (SPSS) Statistics software, version 21.0 (IBM Corporation, USA). No sample size and statistical power calculations were perfomed prior to study. However, post-hoc power analysis showed that with type I error of 5 per cent and current sample sizes (n=54, n=20), the type II error was 100 per cent regarding MMP-9, MMP-9/TIMP-1 and S100B, but regarding TIMP-1 it was found to be only 37 per cent.
Results
Demographics, comorbidities, complications, CCTs, and common medications for the study and control groups are shown in Table I. Laterality of the surgery, contralateral stenosis, gender, pre-existing diseases such as diabetes and hypertension, and nicotine abuse did not significantly influence plasma levels of MMP-9, TIMP-1, or S100B in our study population. The potential effects of aspirin, adenosine diphosphate (ADP) receptor antagonists, and lipid lowering agents were evaluated on MMP-9, TIMP-1 and S100B levels. Patients on ADP receptor antagonists (clopidogrel or ticlopidine) had lower (P<0.05) circulating TIMP-1 levels at baseline (T1). Acetyl salicylic acid had no influence on the measured variables at any time point. Hyperlipidaemia treated with lipid lowering agents was associated with higher (P<0.05) S100B values at the first postoperative day (T3). At reperfusion, lower (P<0.05) S100B levels were noted with intraoperative hypertension, but intraoperative hypotension had no effect. Independent variables (diabetes, intraoperative hypertension, statin and aspirin usage) were selected for final multivariate analysis to predict S100B levels at reperfusion, which showed that 17 per cent of total variability in S100B levels at reperfusion was explained by the selected variables (P<0.05). Intraoperative bleeding and CCT were selected for final linear multivariate analysis regarding MMP-9 levels at T3 and it was noted that 15 per cent of total variability could be explained by the model (P<0.05). Patients requiring temporary shunt insertion had lower (Spearman rho=0.35, P<0.05) TIMP-1 values at baseline (T1). Using stepwise logistic multivariate regression, diabetes, preoperative S100B and TIMP-1 levels were selected for a final model to predict shunting. Using a model including these variables, we were able to predict 100 per cent of shunting (Nagelkerke R2=1; Hosmer and Lemeshow test P=1.00). The results regarding MMP-9, TIMP-1, MMP-9/TIMP-1 and S100B plasma levels are summarized in Table II.
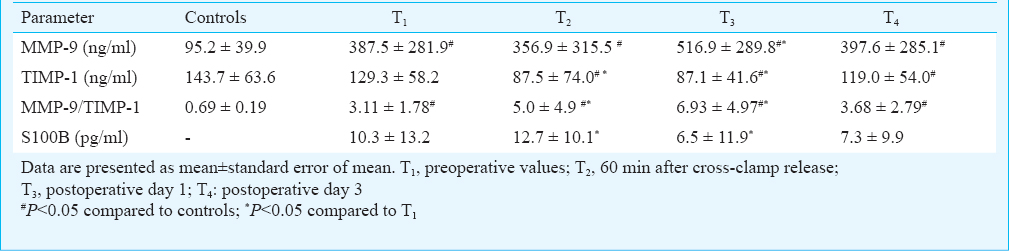
Except at T1 the plasma level of TIMP-1 was significantly lower (P<0.05) compared to controls during the whole study period. Comparing to the preoperative values (T1), after reperfusion (T2) we experienced decreased (P<0.05) TIMP-1 levels and TIMP-1 remained at this significantly lower (P<0.05) level at the first postoperative day (T3), but returned almost to the baseline by T4. Plasma MMP-9 levels were increased (P<0.05) compared to controls at T1 and remained significantly elevated (P<0.05) during the whole investigation. Significant elevation (P<0.05) of MMP-9 levels was noted at T3 compared to T1 then values decreased to approximate T1 levels by T4.
MMP-9/TIMP-1 ratios were markedly increased (P<0.05) at all time points compared to controls. By reperfusion (T2) the ratio of MMP-9/TIMP-1 elevated significantly (P<0.05) and by T3 further elevation (P<0.05) was observed compared to T1. By T4 the MMP-9/TIMP-1 ratio decreased almost to the T1 level.
S100B levels increased (P<0.05) after reperfusion (T2) compared to baseline (T1). Later, at the first postoperative day (T3) a decrease was observed (P<0.05) in S100B levels compared to preoperative samples (T1). S100B in the plasma remained lower comparing to baseline (T1) until the third postoperative day (T4), but this difference was not significant.
Diabetes mellitus (DM) was associated with prolonged CCT (P<0.05). There was a positive correlation between CCT and age of the patients (Spearman rho=0.35, P<0.05). No significant correlation was observed between CCT and the measured variables (MMP-9, TIMP-1, MMP-9/TIMP-1, S100B) at any time point. We selected diabetes, age of patients and nicotine abuse as independent variables for multivariate linear regression analysis, which showed that 19 per cent of total variability in CCT was explained by the selected variables (P<0.05).
A subgroup analysis was performed on patients (n=35) who experienced significant plasma S100B level elevation at reperfusion (T2) and also no correlation observed with CCT and the variables (MMP-9, TIMP-1, MMP-9/TIMP-1) but the kinetics were the same as noted for the entire group.
Discussion
Most studies concerned with the TIMP-MMP system and S100B following CEA assessed changes at a single time point9101112. Our study was aimed to describe the time course of changes in biomarker levels during the perioperative period and to identify factors influencing these changes. Dynamic changes were observed in MMP-9, TIMP-1 and S100B, levels, but strong correlations were not found between the evaluated biomarkers and CCTs. The possible role of TIMP-1 in shunting has emerged, but should be verified in the future studies.
Our study had some limitations. No interventions were performed on controls, thus they received no operation related medications like heparin, bupivacaine, etc. Therefore, comparing postoperative CEA samples to atherosclerotic controls had only limited value. POCD was not assessed. The large difference in sample size between control and study groups might reduce the power of comparison, although Mann-Whitney U test could be used well with unequal sample sizes. No power analysis and sample size calculation were performed prior to study.
From a clinical point of view only advanced age and diabetes were associated with increased CCT in our study, which might be due to advanced atherosclerosis and meticulous surgical procedure during clamping. Among commonly used medications only ADP receptor antagonists and lipid lowering agents altered MMP-TIMP balance and S100B levels.
Decreased preoperative TIMP-1 levels were associated with the need for shunting, but this result was based on a low number of shunted patients in our study. Decreased TIMP-1 might be the sign of plaque instability through increased MMP-TIMP system activity29, although the experienced correlation between MMP-9/TIMP-1 and shunting did not reach the level of significance in our study. If we added preoperative S100B levels and diabetes as predictors to TIMP-1, we could create a good predictive model for shunting. However, the small number of shunted patients might be the limitation of this model also. Thus, future studies are required to clarify these findings.
The mechanism by which ADP receptor antagonists influence TIMP-1 levels is not clear, however, a linear correlation of plasma TIMP-1 levels and platelet count has been demonstrated earlier and it is well known that TIMPs play a role in platelet regulation29. This suggests inhibition of platelet-bound MMPs.
Sanchez-Pena et al30 described reduction of hypoperfusion induced by postoperative vasospasm following intracranial haemorrhage in patients treated with statins, which could be related to their pleiotropic and endothelial protective functions. Elevated S100B following surgery may be a result of decreased intracranial perfusion and distribution of damage-associated protein markers in plasma, while hypertension during surgery may prevent hypoperfusion resulting in tissue damage30. In our study, no direct correlation was observed between S100B and CCT, supporting the importance of microembolization in this complex pathophysiologic process, as besides hypoperfusion, microemboli are the main casues of perioperative ischaemic effects and S100B release. We hypothesize that the decreased S100B on the first postoperative day and thereafter results from improved perfusion and decreased ongoing CNS damage.
Ischaemic damage and later repair of the CNS could result in both increased MMP and decreased TIMP levels in patients with stroke or transient ischaemia3132. The significant decrease of TIMP-1 during our study may be an indicator of increased extracellular matrix turnover following reperfusion3132. A slight, though not significant, increase in TIMP-1 was observed on post-operative day 3 perhaps indicating that the most significant alterations have occurred prior to this.
According to Molloy et al11, patients with transcranial Doppler ultrasound detected emboli express increased MMP-9 levels on the 2nd postoperative day. Our findings indicate that the first postoperative day may be a better time point for MMP-9. The MMP-9/TIMP-1 ratios followed the previously described alterations, indicating increased tissue remodelling. Because of the lack of correlation between MMP-9, TIMP-1, and S100B we suggest measurement of each of these biomarkers in future studies assessing neuronal damage and repair after CEA.
Subtle brain damage and resultant POCD is under-appreciated, under-reported, and poorly understood. The underlying pathophysiologic processes should be elucidated to promote POCD prevention. In this study, we examined MMP-9, TIMP-1, and S100B levels pre-CEA, 1 h post reperfusion, and on post-operative days 1 and 3. Our data will be useful in establishing baseline data for future studies examining biomarkers predictive of POCD. In addition, we propose that TIMP-1 level measurement might help the indication of shunting, thus decreasing POCD incidence after a well powered analysis. Future studies of these and similar biomarkers might provide insight into the causes of POCD and its prevention.
Conflicts of Interest: None.
References
- Incidence and short-term prognosis of transient ischemic attack in a population-based study. Stroke. 2005;36:720-3.
- [Google Scholar]
- Costs and rehabilitation use of stroke survivors: a retrospective study of Medicare beneficiaries. Top Stroke Rehabil. 2009;16:309-20.
- [Google Scholar]
- ESVS guidelines Collaborators. Invasive treatment for carotid stenosis: indications, techniques. Eur J Vasc Endovasc Surg. 2009;37(4 Suppl):1-19.
- [Google Scholar]
- Local versus general anaesthesia for carotid endarterectomy. Cochrane database Syst Rev. 2008;4:CD000126.
- [Google Scholar]
- A controlled prospective study of neuropsychological dysfunction following carotid endarterectomy. Arch Neurol. 2002;59:217-22.
- [Google Scholar]
- Vascular Surgical Society of Great Britain and Ireland: impact of spontaneous embolization on cognitive function. Br J Surg. 1999;86:691.
- [Google Scholar]
- Neuropsychological impairment after carotid endarterectomy correlates with intraoperative ischemia. Cortex. 1984;20:403-12.
- [Google Scholar]
- Postoperative cerebral hyperperfusion associated with impaired cognitive function in patients undergoing carotid endarterectomy. J Neurosurg. 2005;102:38-44.
- [Google Scholar]
- Serum S100B protein levels are correlated with subclinical neurocognitive declines after carotid endarterectomy. Neurosurgery. 2001;49:1076. discussion 1082-3
- [Google Scholar]
- Subtle brain damage cannot be detected by measuring neuron-specific enolase and S-100beta protein after carotid endarterectomy. J Cardiothorac Vasc Anesth. 2000;14:166-70.
- [Google Scholar]
- Elevation in plasma MMP-9 following carotid endarterectomy is associated with particulate cerebral embolisation. Eur J Vasc Endovasc Surg. 2004;27:409-13.
- [Google Scholar]
- MMP-9 levels in elderly patients with cognitive dysfunction after carotid surgery. J Clin Neurosci. 2010;17:436-40.
- [Google Scholar]
- Inflammation and cognitive dysfunction in type 2 diabetic carotid endarterectomy patients. Diabetes Care. 2013;36:3283-6.
- [Google Scholar]
- Dynamic changes of matrix metalloproteinases and their tissue inhibitors in severe sepsis. J Crit Care. 2011;26:550-5.
- [Google Scholar]
- Increases in circulating matrix metalloproteinase-9 levels following fibrinolysis for acute pulmonary embolism. Thromb Res. 2010;125:549-53.
- [Google Scholar]
- Plasma MMP-2-TIMP-2 complex levels measured during follow-up predict a risk of relapse in patients with malignant lymphoma. Eur J Haematol. 2008;80:46-54.
- [Google Scholar]
- Matrix metalloproteinase-9, -10, and tissue inhibitor of matrix metalloproteinases-1 blood levels as biomarkers of severity and mortality in sepsis. Crit Care. 2009;13:R158.
- [Google Scholar]
- Increased brain expression of matrix metalloproteinase-9 after ischemic and hemorrhagic human stroke. Stroke. 2006;37:1399-406.
- [Google Scholar]
- Role for matrix metalloproteinase 9 after focal cerebral ischemia: effects of gene knockout and enzyme inhibition with BB-94. J Cereb Blood Flow Metab. 2000;20:1681-9.
- [Google Scholar]
- Mmp-9 inhibition: a therapeutic strategy in ischemic stroke. Mol Neurobiol. 2014;49:563-73.
- [Google Scholar]
- Neuroprotective effect of bicyclol in rat ischemic stroke: down-regulates TLR4, TLR9, TRAF6, NF-êB, MMP-9 and up-regulates claudin-5 expression. Brain Res. 2013;1528:80-8.
- [Google Scholar]
- The TIMPs tango with MMPs and more in the central nervous system. J Neurosci Res. 2004;75:1-11.
- [Google Scholar]
- Limited clinical value of multiple blood markers in the diagnosis of ischemic stroke. Clin Biochem. 2013;46:710-5.
- [Google Scholar]
- Carotid endarterectomy: general principles and surgical technique. Neurosurg Clin N Am. 2000;11:279-97.
- [Google Scholar]
- Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81-4.
- [Google Scholar]
- Neurological monitoring during carotid artery stenting: the Duck Squeezing Test. J Endovasc Surg. 1999;6:332-6.
- [Google Scholar]
- Plasma S-100b protein concentration in healthy adults is age- and sex-independent. Clin Chem. 1998;44:1056-8.
- [Google Scholar]
- Metalloproteinases and their inhibitors are markers of plaque instability. Surgery. 2005;137:355-63.
- [Google Scholar]
- Atorvastatin decreases computed tomography and S100-assessed brain ischemia after subarachnoid aneurysmal hemorrhage: a comparative study. Crit Care Med. 2012;40:594-602.
- [Google Scholar]
- Role of matrix metalloproteinases in delayed cortical responses after stroke. Nat Med. 2006;12:441-5.
- [Google Scholar]
- Matrix metalloproteinase expression after human cardioembolic stroke: temporal profile and relation to neurological impairment. Stroke. 2001;32:1759-66.
- [Google Scholar]




