
Translate this page into:
Performance of the 2010 American College of Rheumatology/European League against Rheumatism (ACR/EULAR) criteria for classification of rheumatoid arthritis in an Indian population: An observational study in a single centre
Reprint requests: Dr K. Prakashini, Department of Radiology, Kasturba Medical College, Manipal 576 104, Karnataka, India e-mail: docprakashinik@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The 1987 American College of Rheumatology (ACR) criteria were criticised for classifying patients only in the late stage. The 2010 ACR/European League against Rheumatism (ACR/EULAR) classification criteria for rheumatoid arthritis (RA) were thus formulated to recognize the early stage of disease with high sensitivity. This pilot study was designed to estimate and compare the sensitivities of the 1987 ACR and 2010 ACR/EULAR classification criteria for RA.
Methods:
In a tertiary care hospital, the medical records of 97 patients diagnosed with RA were reviewed. Case study forms were filled with relevant clinical data and investigation results after reviewing each medical record. The radiographs of hands were also reviewed. To each case, both the 1987 ACR and the 2010 ACR/EULAR criteria were applied and the results of the classification were noted.
Results:
The sensitivity of the 2010 ACR/EULAR criteria was found to be 79.38 per cent [95% confidence interval (CI) = 71.33-87.43%] and the sensitivity of the 1987 ACR criteria was found to be 63.92 per cent (95% CI = 54.36-73.48%). The difference in the sensitivities was significant (P< 0.01). There was a significant rise in sensitivity of the 2010 ACR/EULAR criteria when patients having anti-cyclic citrullinated peptide (CCP) titres were analysed.
Interpretation & conclusions:
The 2010 ACR/EULAR criteria were found to be more sensitive than the 1987 ACR criteria possibly owing to features of the criteria. Anti-CCP titres were found to increase the sensitivity of the 2010 ACR/EULAR criteria.
Keywords
1987 ACR classification criteria
2010 ACR/EULAR classification criteria
rheumatoid arthritis

Rheumatoid arthritis (RA) is an autoimmune disorder most commonly seen in middle-aged women, characterized by joint swelling, tenderness and destruction of the joints leading to severe disability12345. The crude prevalence of RA in India was estimated to be 0.38 per cent6. The most widely accepted classification criteria for RA before 2010 were the 1987 American College of Rheumatology (ACR) classification criteria which required the presence of established joint damage7, possibly limiting the ability to identify early RA and delaying the initiation of therapy until irreversible damage has occurred8. Later on, studies have shown that early achievement of a low disease activity state is beneficial for the future disease course91011. Due to these advancements, the 1987 ACR classification criteria for RA8 were criticised because using these criteria it was not possible to diagnose RA early in the disease course. This led to the development of the new 2010 ACR/European League against Rheumatism (ACR/EULAR) classification criteria to identify RA at an early stage with greater sensitivity12.
The 2010 ACR/EULAR criteria present a new approach with a specific emphasis on identifying patients with a relatively short duration of symptoms, who may benefit from the early institution of disease-modifying anti-rheumatoid drugs (DMARDs)910 therapy or entry into the clinical trials of promising new agents that arrest the progression of the disease. The 2010 ACR/EULAR criteria employ a score-based algorithm that considers types and number of joints involved, duration of involvement, serology [rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP)] and acute phase reactants (APRs)12.
Although the diagnostic and discriminative abilities of the new criteria are well known, but literature pertaining to their performance in India is limited. Diagnostic algorithms tend to overestimate their effectiveness when only tested in the population they were derived from13. Therefore, the discriminative abilities of such algorithms should be tested in other samples before putting them into practice. In this context, we designed a pilot study to estimate and compare the sensitivities of the 1987 ACR and 2010 ACR/EULAR classification criteria for RA and to see what proportion of patients with early arthritis who did not fulfil the 1987 ACR criteria could, according to the 2010 criteria, be classified as having RA.
Material & Methods
This retrospective, observational study was conducted at Kasturba Hospital, Manipal, India, and cases were selected between March and September 2011. Ninety seven cases were included in the study. Inclusion criteria were patients who were (i) diagnosed with RA in the previous two years based on clinical presentation, follow up and response to therapy, (ii) screened for other alternate diagnosis through either clinical evaluation or investigations and those were found to be RA only, (iii) having radiographs of their hands available (for the 1987 ACR criteria), (iv) having at least one of the serological tests available (anti-CCP and/or RF), (v) having at least one of the APR titres available [erythrocyte sedimentation rate (ESR) and/or C-reactive protein (CRP)] and (vi) having history and examination findings required to compare the patients with the 1987 ACR and 2010 ACR/EULAR criteria. Exclusion criteria were patients whose records did not contain the information necessary to fill the case study form and diagnosis had changed during the disease. The study protocol was approved by the institutional ethics committee.
Collection of clinical data: A case study form was completed using patients’ history, examination findings and investigations that were recorded when they were diagnosed as having RA. The case study form allowed an assessment of the extent to which symptoms, signs and initial results of the investigations conformed to the 1987 ACR and 2010 ACR/EULAR classification criteria sets. Data recorded on the case study form comprised name, age, sex, duration of symptoms, morning stiffness and its duration, joint involvement (left or right proximal interphalangeal, metacarpophalangeal, wrist, elbow, knee, ankle, metatarsophalangeal, shoulder and hip) and symmetry of involvement and presence of rheumatoid nodules. ESR, CRP (estimated using turbidimetry or latex agglutination test), RF and anti-CCP (estimated using ELISA) titres were recorded. The radiographs were viewed and checked for typical changes of RA, such as juxta-articular osteopenia and erosions, by a radiologist. Comparison of the data was made with the 1987 ACR and 2010 ACR/EULAR classification criteria for RA.
A total of 160 medical records of patients diagnosed with RA were reviewed; of which 97 were included in our study after using inclusion and exclusion criteria.
Outcome measures: The outcome measures included sensitivities (the proportion of patients with the disease who were positive for the feature when related to all individuals with the disease) of the 1987 ACR and 2010 ACR/EULAR classification criteria.
Statistical analysis: Data were entered into SPSS version 16.0 (SPSS Inc, Chicago, USA) checked for errors and finally analysed. Chi-square test was used to compare categorical variables whereas student t test was used to compare means of continuous variables.
Results
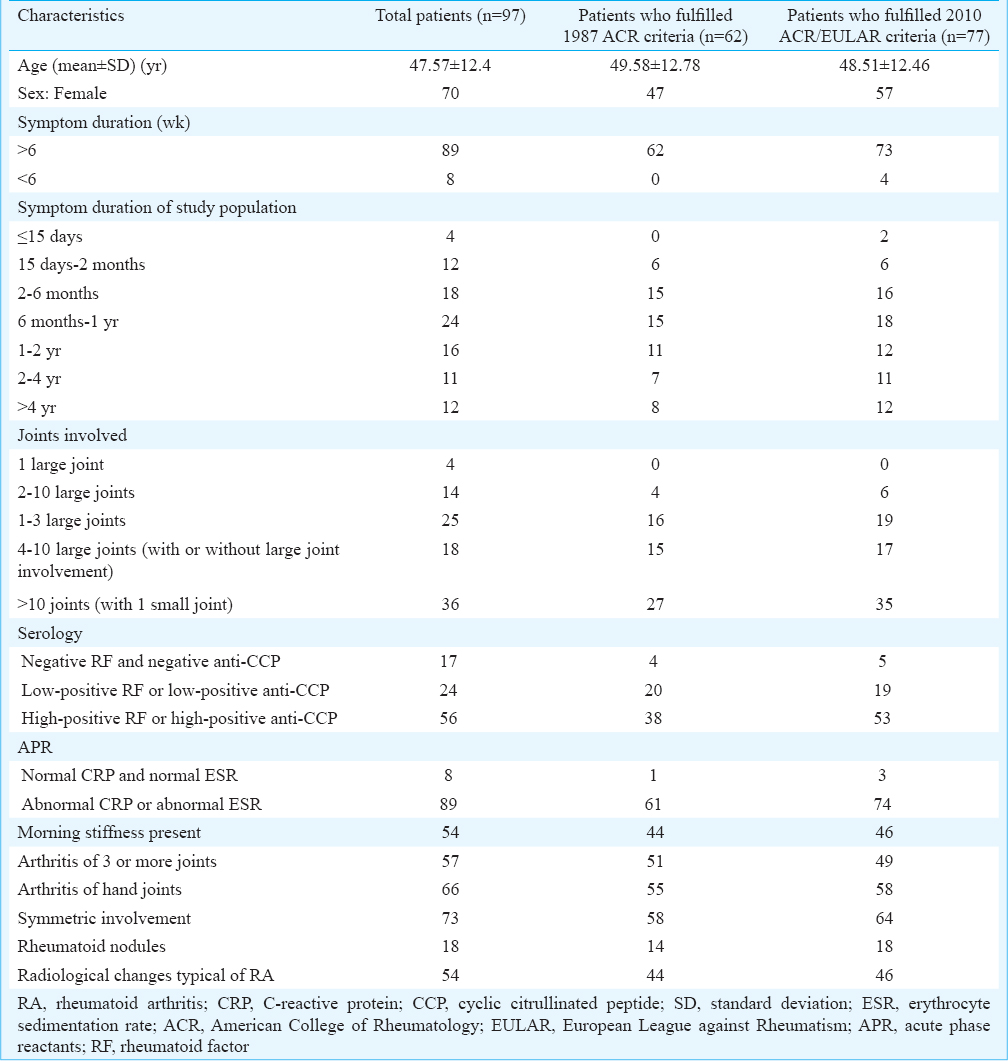
Ninety seven complete case study forms were filled. After analysis, it was found that 62 of them were classified as RA by the 1987 ACR criteria [sensitivity = 63.92 % (95% confidence interval, CI) = 54.36-73.48%)] and 77 were classified as RA by the 2010 ACR/EULAR criteria [sensitivity = 79.38 per cent (95% CI = 71.33-87.43%)]. The difference in the sensitivities was significant (P < 0.01). Twenty patients who were not classified as RA by the 1987 ACR criteria were classified as RA by the 2010 ACR/EULAR criteria, and five patients who were not classified as RA by 2010 criteria were classified as RA by 1987 criteria. The Table shows the characteristics of the study population. There were no significant differences in the characteristics, suggesting the absence of any confounding variable. In the patients whose disease duration was one year or lesser, there were no significant differences in the sensitivities of 2010 ACR/EULAR criteria and 1987 ACR.
In the study population, anti-CCP titres were available only in 50 patients due to financial disabilities of the patients. Of these 50 patients, 31 were positive. In the 31 anti-CCP positive patients, 28 (90.3%) could be classified as RA by the 2010 ACR/EULAR criteria, and only 20 (64.5%) were classified as RA by the1987 ACR criteria. There was a significant rise in sensitivity (P<0.01). In the 47 patients in whom anti-CCP titres were not available, both the 1987 ACR and the 2010 ACR/EULAR criteria were able to classify the same number of cases as RA (n=36).
Discussion
Our findings suggested that the 2010 ACR/EULAR classification criteria for RA were more sensitive than the 1987 ACR criteria. This was similar to the conclusions drawn in other studies141516. There was a significant rise in the sensitivity of the 2010 ACR/EULAR criteria when anti-CCP titres were available. In the patients whose disease duration was one year or lesser, there was no significant difference in the sensitivities between the 2010 ACR/EULAR and 1987 ACR criteria. This was probably due to selection bias (less number of early RA cases) and limited sample size. It can be inferred that the increased sensitivity of 2010 ACR/EULAR criteria shown in this study could be due to other features of the criteria, such as the inclusion of anti-CCP titres and joint count. According to the 2010 ACR/EULAR criteria, joint involvement refers to any tender or swollen joint, whereas the 1987 ACR criteria require swelling of the joint for defining involved joints12. This could lead to increased sensitivity of the 2010 ACR/EULAR criteria.
The cases that were classified as RA by the 1987 ACR criteria but not by the 2010 ACR/EULAR criteria might be attributed to chance as these criteria are classification criteria and not diagnostic in nature and are mainly used for inclusion into various studies.
Limitations of our study included the following: (i) The power of study was limited due to the small sample size; (ii) The study could not suggest that the 2010 ACR/EULAR criteria classified RA at an early stage. This could be due to a limited number of early RA patients in the study; (iii) The patients diagnosed as RA based on clinical presentation, follow up and response to therapy, were included in the study. Hence, the specificities, positive predictive values and negative predictive values could not be ascertained.
The specificity of 2010 ACR/EULAR criteria was lesser than 1987 ACR criteria according to some studies815, but this could not be assessed in our study as non-RA patients were not included. One such study17 conducted in New York showed that specificity of the 2010 criteria in classifying RA was 55 per cent compared with 76 per cent by the 1987 ACR criteria and 66.7 per cent of systemic lupus erythematosus patients, 50 per cent of osteoarthritis, 37.5 per cent of psoriatic arthritis and 27.2 per cent of others fulfilled the new criteria and could have been classified as RA. In another study15, there was a high proportion of patients who were mis-classified as RA by the 2010 ACR/EULAR criteria. Thus, overdiagnosis remains a concern with the new 2010 ACR/EULAR criteria.
In conclusion, the findings of our pilot study show that the 2010 ACR/EULAR criteria provide a more sensitive method to classify RA than the 1987 ACR criteria. However, care has to be taken to rule out other diseases before applying the 2010 ACR/EULAR criteria. The 2010 ACR/EULAR criteria can be used to include patients in studies focussing on early initiation of treatment. Long-term prospective trials are required to evaluate the benefit of the 2010 ACR/EULAR criteria and ascertaining the benefit with early treatment.
Acknowledgment
Authors thank Drs Sudha Vidyasagar V. R. K. Rao, Asha Kamath & Ananth Pai for their guidance and helping in statistical analysis.
Conflicts of Interest: None.
References
- Long-term outcome of treating rheumatoid arthritis: Results after 20 years. Lancet. 1987;1:1108-11.
- [Google Scholar]
- Survival, prognosis, and causes of death in rheumatoid arthritis. Arthritis Rheum. 1986;29:706-14.
- [Google Scholar]
- Severe functional declines, work disability, and increased mortality in seventy-five rheumatoid arthritis patients studied over nine years. Arthritis Rheum. 1984;27:864-72.
- [Google Scholar]
- Global Health Epidemiology Reference Group (GHERG). Prevalence of rheumatoid arthritis in low– and middle-income countries: A systematic review and analysis. J Glob Health. 2015;5:010409.
- [Google Scholar]
- The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315-24.
- [Google Scholar]
- Classification of rheumatoid arthritis: Comparison of the 1987 American College of Rheumatology criteria and the 2010 American College of Rheumatology/European League Against Rheumatism criteria. Arthritis Rheum. 2011;63:37-42.
- [Google Scholar]
- Benefit of very early referral and very early therapy with disease-modifying anti-rheumatic drugs in patients with early rheumatoid arthritis. Rheumatology (Oxford). 2004;43:906-14.
- [Google Scholar]
- Retardation of joint damage in patients with early rheumatoid arthritis by initial aggressive treatment with disease-modifying antirheumatic drugs: Five-year experience from the FIN-RACo study. Arthritis Rheum. 2004;50:2072-81.
- [Google Scholar]
- The long-term impact of early treatment of rheumatoid arthritis on radiographic progression: A population-based cohort study. Rheumatology (Oxford). 2011;50:1106-10.
- [Google Scholar]
- 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010;69:1580-8.
- [Google Scholar]
- Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. 1996;15:361-87.
- [Google Scholar]
- The clinical picture of rheumatoid arthritis according to the 2010 American College of Rheumatology/European League against Rheumatism criteria: Is this still the same disease? Arthritis Rheum. 2012;64:389-93.
- [Google Scholar]
- Validation of the 2010 ACR/EULAR classification criteria for rheumatoid arthritis: Slight improvement over the 1987 ACR criteria. Ann Rheum Dis. 2011;70:1468-70.
- [Google Scholar]
- Diagnostic performance of the ACR/EULAR 2010 criteria for rheumatoid arthritis and two diagnostic algorithms in an early arthritis clinic (REACH) Ann Rheum Dis. 2011;70:1645-7.
- [Google Scholar]
- Utility of the new rheumatoid arthritis 2010 ACR/EULAR classification criteria in routine clinical care. BMJ Open 2012 2 pii: E001117
- [Google Scholar]




