
Translate this page into:
Palpable crepitus as a rare clinical presentation of emphysematous pyelonephritis
*For correspondence: minks_77@rediffmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 41 yr old diabetic and hypertensive woman† presented to the emergency department of Jawaharlal Institute of Postgraduate Medical Education & Research, Puducherry, India, in October 2016 with complaints of abdominal pain, fever and breathlessness for the past one week. On examination, she had left flank tenderness with palpable crepitus occupying the entire flank region extending on to the gluteal region. Her urine microscopy demonstrated pyuria with bacteriuria. Urine culture showed Escherichia coli and Enterococcus species. Total leucocyte counts were 33,340/μl, random blood sugar was 547 mg/dl and serum creatinine was 11.04 mg/dl. X-ray and computerized tomography of the abdomen showed emphysematous pyelonephritis of the left kidney with extensive parenchymal destruction, pneumoretroperitoneum and subcutaneous emphysema (Figs 1–3). After initial resuscitation with intravenous antibiotics and haemodialysis, four percutaneous drains were placed in the renal parenchyma and paranephric space under ultrasonographic guidance. The patient recovered well after drainage of foul-smelling pus and gas. Subcutaneous emphysema resolved spontaneously. The patient underwent delayed nephrectomy four weeks after effective control of blood sugar levels. In this patient, the extensive subcutaneous emphysema led to the clinical suspicion of emphysematous pyelonephritis which was confirmed by imaging. The patient reported for the last follow up three months after the surgery with a nadir serum creatinine of 2 mg/dl.
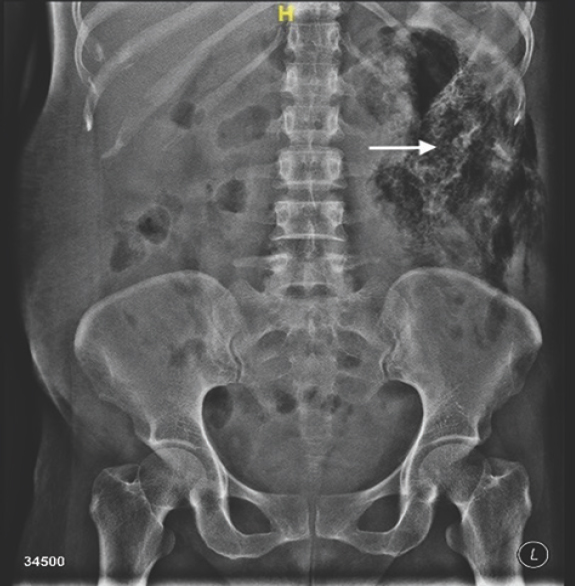
- X-ray kidney ureter bladder showing gaseous radio-dense shadow occupying left side of abdomen (arrow).
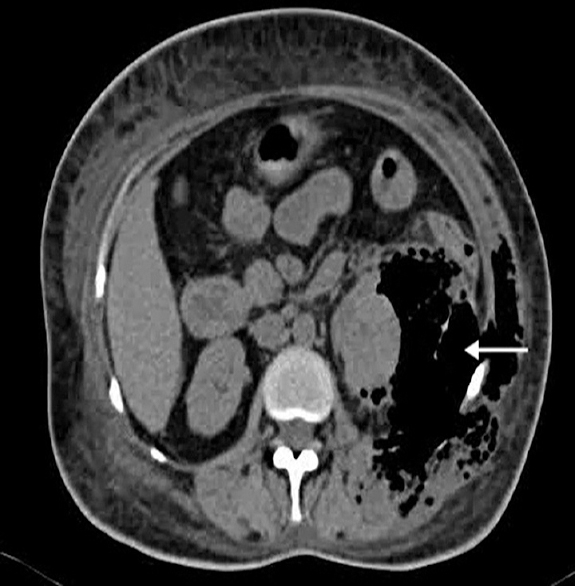
- Cross-section computed tomographic images showing gas in perinephric space (arrow).
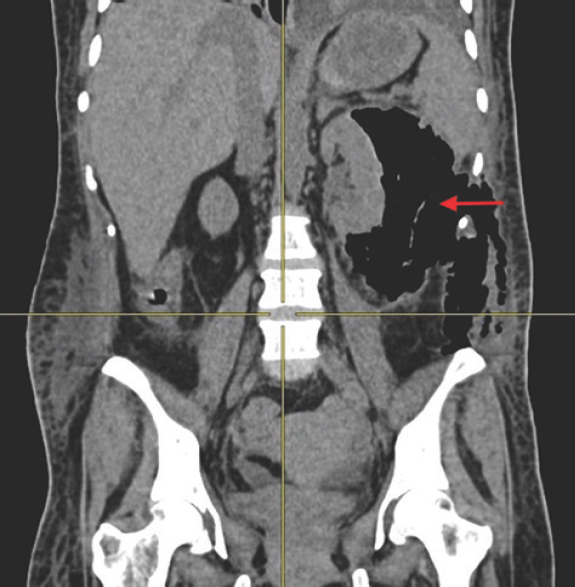
- Coronal reformatted computed tomographic image showing destruction of the left kidney with emphysematous changes, retropneumoperitoneum and subcutaneous emphysema (arrow).
Conflicts of Interest: None.




