
Translate this page into:
Osseous sarcoidosis with lupus pernio
*For correspondence:: alicesam2509@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 60 yr old woman presented to the department of General Medicine, Christian Medical College and Hospital, Vellore, India, in April, 2016 with an 18-month history of purple discolouration and painless swelling of the right index finger, right second toe and bridge of nose. Physical examination revealed a violaceous indurated plaque on the bridge of nose, along with dactylitis of the involved digits, with no fingernail changes (Fig. 1A-C). Radiographs showed osteolytic lesions in the phalanges with a reticular pattern (Fig. 2A, B) and hilar lymph node enlargement (Fig. 2C). Serum angiotensin-converting enzyme levels were elevated (69 U/l, normal 8-52 U/l) while thoracoabdominal computed tomography scan showed mediastinal, hilar and abdominal lymphadenopathy (Fig. 3). There was no clinical or laboratory evidence of multiple myeloma. Biopsy from the skin and bone lesions showed non-necrotizing granulomas containing giant cells, with no evidence of mycobacterial or fungal infection (Fig. 4A, B). A diagnosis of lupus pernio with osseous sarcoidosis was made. The patient was treated with prednisolone (1 mg/kg) for two weeks with tapering to 10 mg/day over six weeks, hydroxychloroquine (400 mg/day) and topical mometasone ointment for two months. At follow up after four days, the lesions demonstrated partial resolution (Fig. 5A, B).

- (A) Photograph of the hand showing dactylitis of the right index finger (black arrow). (B) Violaceous indurated plaque on the bridge of nose (black arrow). (C) Dactylitis of the right second toe (black arrow).
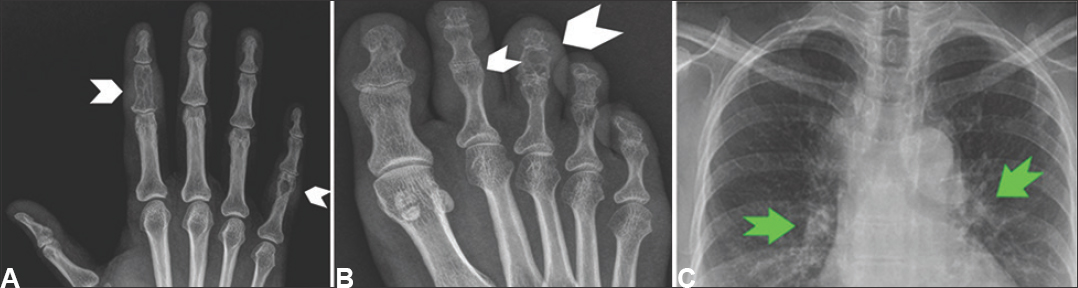
- (A) X-ray of the right hand showing osteolytic lesions in the involved phalanges with a reticular pattern (white arrowheads). (B) X-ray of the right foot showing osteolytic lesions in the involved phalanges (white arrowheads). (C) X-ray chest with bilateral hilar lymph node enlargement (green arrows).
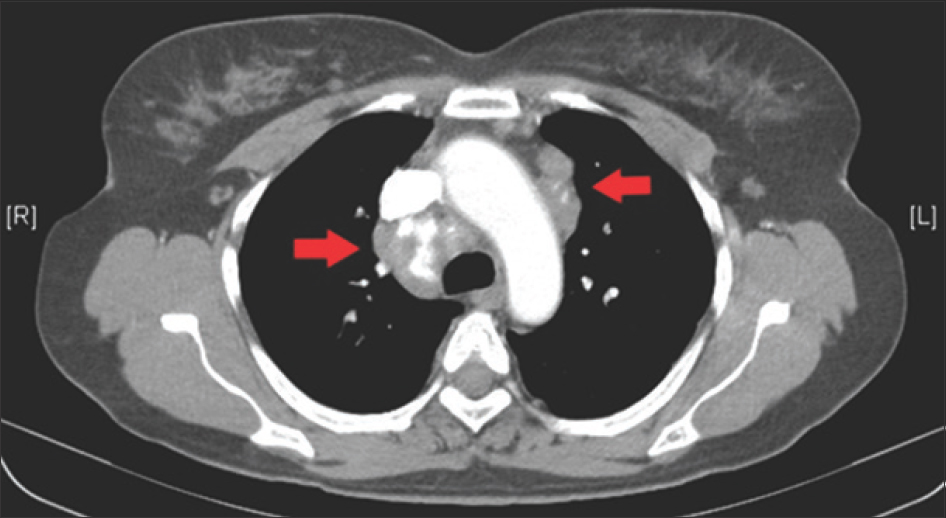
- Computed tomography scan of the thorax showing bilateral mediastinal lymphadenopathy (red arrows), including calcified lymph nodes on the right.
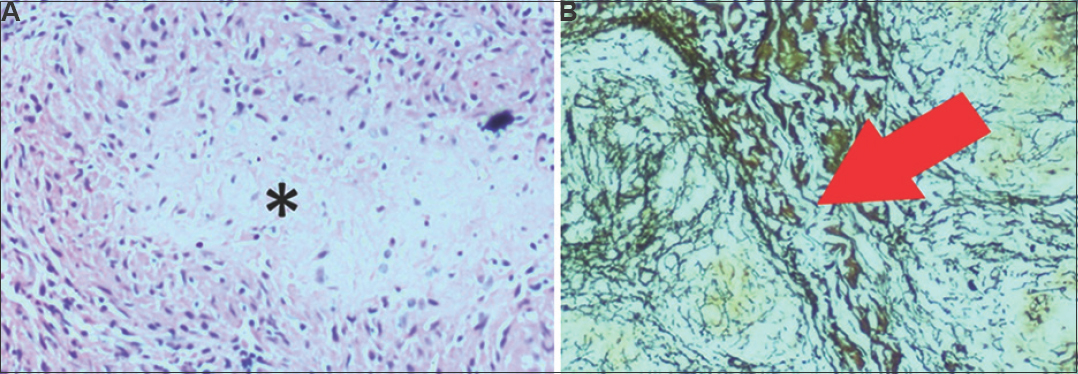
- (A) Bone biopsy demonstrating granulomas, marked asterisk (*) (H & E, ×20). (B) Skin biopsy demonstrating non-necrotizing granulomas (red arrow) reticulin stain, ×10.
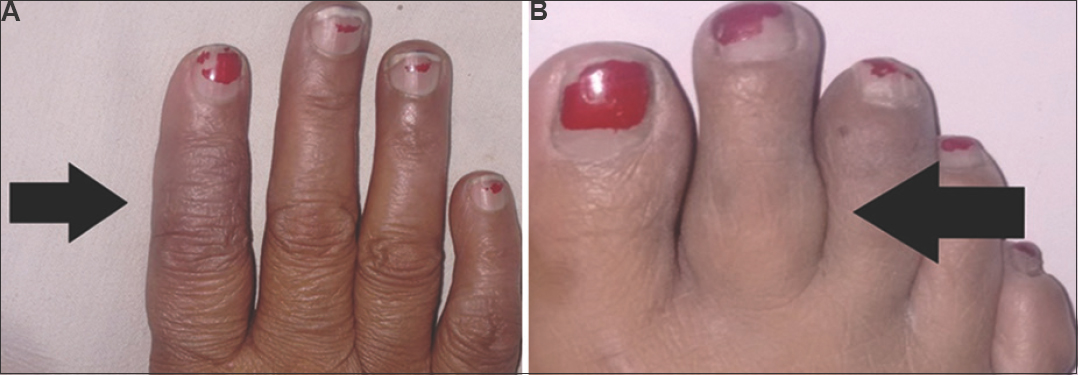
- (A) Hand lesion demonstrating partial resolution after 4 days of therapy (black arrow). (B) Right foot lesion demonstrating partial resolution after 4 days of therapy (black arrow).
Osseous sarcoidosis occurs usually in patients with multivisceral involvement and has a predilection for small bones of the hand and feet. Skeletal lesions are often associated with cutaneous manifestations, most commonly lupus pernio, as in this patient. Differentials such as skeletal metastases, multiple myeloma and chronic osteomyelitis should be considered and ruled out before the treatment. Non-steroidal anti-inflammatory drugs, corticosteroids and hydroxychloroquine are the mainstay of therapy.




