
Translate this page into:
Ocular manifestations in patients attending antiretroviral therapy centre at a tertiary care hospital in Himachal Pradesh, India
For correspondence: Dr Anil Chauhan, Department of Ophthalmology, Dr. Rajendra Prasad Government Medical College, Tanda 176 001, Kangra, Himachal Pradesh, India e-mail: dr.a.chauhan@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Ocular manifestations in HIV/AIDS patients range from adnexal disorders to the posterior segment disease. This study was aimed to evaluate the ocular manifestations, including vision-threatening manifestations in HIV-positive patients attending an antiretroviral therapy centre (ART) of a tertiary care hospital in north India and its association with the CD4+ cell count.
Methods:
This cross-sectional study was conducted in the department of Ophthalmology in collaboration with the ART centre. An equal number of patients were selected from each year i.e., 30 patients each from those registered in the year 2010 till 2015. These patients were selected randomly from the register using systematic randomization. Hence, a total of 150 patients were examined for ocular manifestations. All the patients included in this study were on highly active ART.
Results:
Of the 150 patients examined, 53 per cent were females and 47 per cent were males. Heterosexual transmission was the most common mode of transmission in 126 (84%) patients. Maximum number of patients was in the age group of 31-40 yr. Ocular manifestations were present in 53 [35.3%; 95% confidence interval (CI): 28-43%] patients. Twelve (8%; 95% CI: 4-12%) patients had lid and adnexal manifestations. Anterior-segment manifestations were present in 20 (13.3%; 95% CI: 8-19%) patients. Posterior-segment manifestations were present in 21 (14%; 95% CI: 8-20%) and vision-threatening posterior-segment ocular lesions were present in 14 per cent of the patients. Univariate logistic regression showed a significant (P <0.001) inverse association of CD4+T-cell count with the vision-threatening posterior-segment ocular lesions.
Interpretation & conclusions:
Routine ocular examination may be done in all the HIV/AIDS patients to detect and treat vision-threatening ocular lesions at the earliest.
Keywords
Adnexal manifestation
CD4+T-cell count
CMV retinitis
HIV
ocular lesions

The clinical course of HIV infection progresses from acute HIV syndrome to asymptomatic phase, with or without persistent generalised lymphadenopathy, and finally the advanced stage of AIDS, resulting in opportunistic infections and malignancies ultimately leading to death1. The lifetime cumulative risk of developing at least one abnormal ocular lesion among HIV positives ranges from 52 to 100 per cent2. The ocular adnexal manifestations involve the eyelids, conjunctiva and the lacrimal drainage system. These manifestations range from the innocuous trichomegaly to life-threatening lymphoma. Common adnexal manifestations include Herpes zoster ophthalmicus (HZO), molluscum contagiosum, blepharitis, Stevens-Johnson syndrome, Kaposi's sarcoma and conjunctival microvasculopathy. Purushottam et al3 reported conjunctivitis in four, blepharitis in two and molluscum contagiosum, stye and HZO in one patient each in a total of 103 HIV infected patients.
Microvasculopathy is the most common ocular manifestation of AIDS, seen in about 40-60 per cent of HIV-positive patients. Most patients with microvasculopathy are asymptomatic. It clinically manifests as cotton wool spots (CWS), intraretinal haemorrhages and microaneurysms, particularly around the posterior pole. The likelihood of formation of CWS is significantly higher in patients with lower CD4+T-cell count4. Kumar et al5 conducted a study on 125 patients in a tertiary eye care centre. They reported that 53.23 per cent of the patients with CD4+T-cell count <200 cells/μl and 15.87 per cent of patients with CD4+T-cell count >200 cells/μl had ocular manifestations. Bekele et al6 also observed that ocular lesions were more common in patients with CD4+T-cell counts <200 cells/μl and that low CD4+T-cell count was an independent risk factor in the development of ocular manifestations in HIV/AIDS. This study was undertaken to determine various ocular manifestations in HIV positive patients attending an ART centre in north India, and also evaluate the association between CD4+T cell count and ocular manifestations.
Material & Methods
This was a cross-sectional study conducted in the department of Ophthalmology in Dr. Rajendra Prasad Government Medical College (Dr. RPGMC), Kangra at Tanda, Himachal Pradesh, India, in collaboration with the antiretroviral therapy (ART) centre. The ART centre in Dr. RPGMC, Kangra at Tanda was opened in 2010. Till the start of this study, in 2014, about 1000 HIV patients were registered with the centre. All the patients included in our study were on highly active ART (HAART). A method of systematic randomization was devised in which HIV-positive patients registered with the centre were enrolled with effect from 2010 till 2015. An equal number of patients were selected from each year i.e., 30 patients each from those registered in 2010 till 2015. Hence, a total of 150 patients were included in this study. The patients who were not willing to participate were excluded and the next patient was enrolled.
Written informed consent was taken from all participants prior to the examination, and study was approved by the ethics committee of the medical college. The detailed history was taken and complete ocular examination was done thereafter. The ocular examination included visual acuity, pupillary reflexes, ocular motility, slit-lamp biomicroscopy and detailed fundus examination using indirect ophthalmoscope.
Laboratory investigations: Complete haemogram, fasting blood sugar, Mantoux test, chest X-ray Toxo/Rubella/cytomegalovirus (CMV) IgG and IgM titres were done as per relevance.
CD4+T-cell count was obtained in all the patients and on the basis of range of CD4+T-cell count in cells/μl, the patients were divided into five groups: group 1 (0-50), group 2 (51-100), group 3 (101-150), group 4 (151-200) and group 5 (>200).
Statistical analysis: The categorical variables were expressed as proportions and 95 per cent confidence intervals (CI), and the continuous variables were expressed as mean±standard deviation. Association between CD4+T-cell count and the vision-threatening posterior-segment ocular manifestations of HIV/AIDS was analysed using univariate logistic regression and expressed as Exp(B) and 95 per cent CI.
Results
Out of the 150 HIV-positive patients examined for ocular manifestations, 78 (53%) were women and 72 (47%) were men. Median age was 36 yr and the most common age group was 31-40 yr in 38 per cent of the patients. Heterosexual transmission was the most common mode of transmission in 126 patients (84%), followed by vertical transmission in 21 (14%), iatrogenic in two (1.3%) and homosexual transmission in one patient. As far as occupation was concerned, drivers constituted 27 (37%) of the males while 60 (78%) of the females were homemakers. Other patients were in private job (n=14, 9%), business (n=5, 3%), government job (n=9, 6%), skilled workers (n=35, 23%) and agriculturists (n=6, 4%). Students accounted for 15 per cent of the patients in our study. Diminution of vision was the chief complaint in 42 (28%) patients while 14 (9.3%) presented with redness, itching and watering. Pain, photophobia and blurring of vision were present in eight (5.3%) of the patients. Eighty six (57.3%) patients had no ocular complaint.
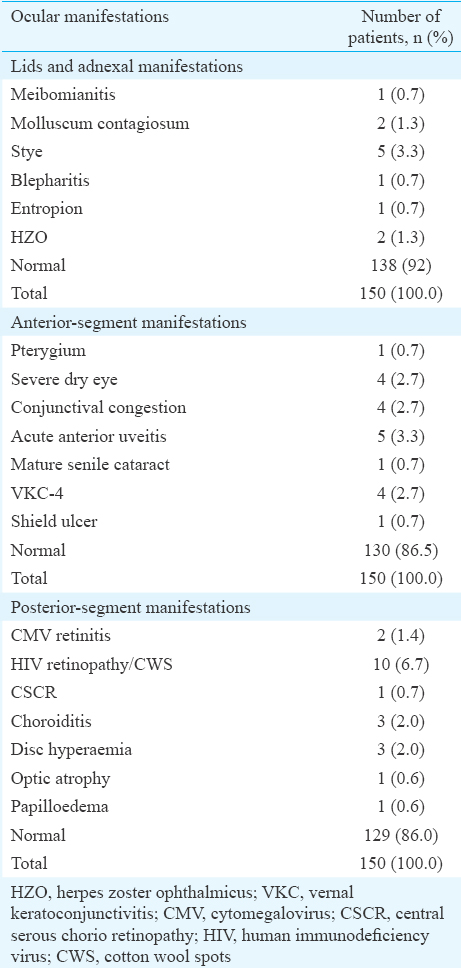
Ocular manifestations were present in 53 (35.3%; 95% CI: 28-43%) patients. Twelve (8%; 95% CI: 4-12%) patients had lid and adnexal manifestations. Stye was present in five (3.3%) patients and molluscum contagiosum and HZO in two (1.3%) patients each. Meibomitis, blepharitis and entropion were present in one patient each. Anterior-segment manifestations were present in 20 (13.3%; 95% CI: 8-19%) patients and were in the form of pterygium in one patient, severe dry eye, vernal keratoconjunctivitis and conjunctival congestion in four (2.7%) patients each. Shield ulcer was present in one patient while anterior uveitis in five (3.3%) patients. Mature cataract was present in one patient and he was operated for the same. Posterior-segment manifestations were present in 21 (14%; 95% CI: 8-20%) patients and were in the form of HIV retinopathy in 10 (6.7%), choroiditis and hyperaemic disc in three (2%) each. CMV retinitis was present in two (1.4%) patients and central serous retinopathy, papilloedema and optic atrophy in one patient each. Figs 1 and 2 show the posterior-segment manifestations in the form of CWS and CMV retinitis. Details of the ocular lesions are shown in Table I.
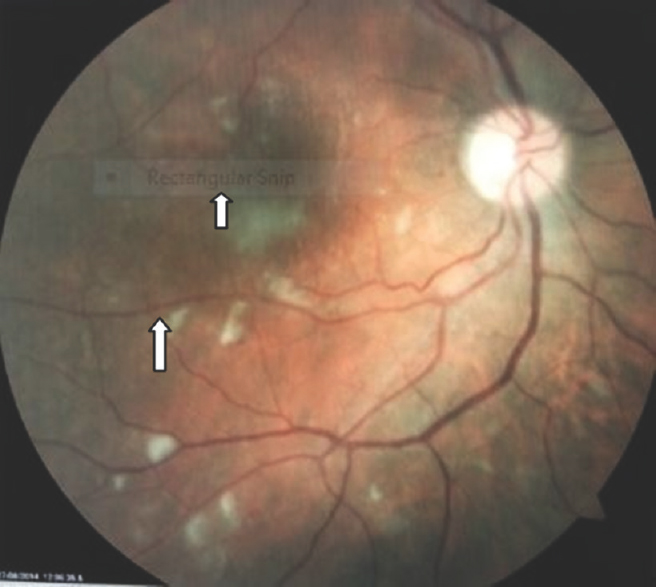
- Multiple cotton wool spots in a patient with HIV retinopathy (arrows).
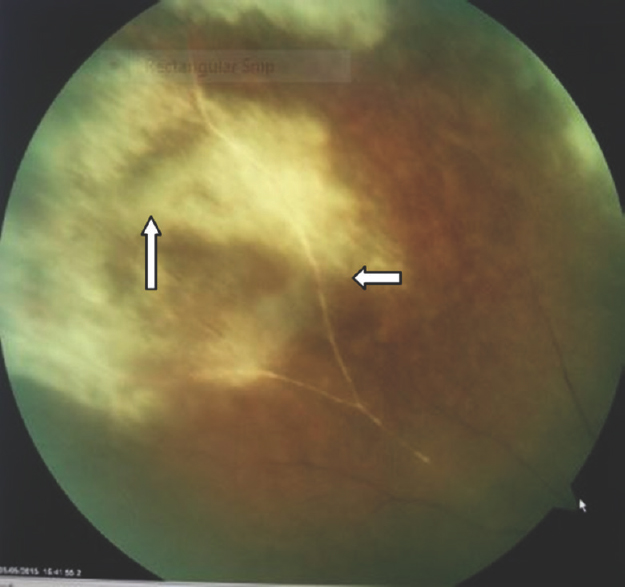
- Cytomegalovirus retinitis in a patient with HIV. Arrows point towards extensive area of retinal necrosis. Also visible is the typical frosted branch angitis appearance of the vessel.
The patients were grouped into five groups on the basis of CD4+T-cell count. The patients in these groups with vision-threatening and general eye findings are shown in Table II. Using univariate logistic regression, the odds ratio for CD4+T cell counts with posterior-segment lesions were compared and a significant inverse association, [Exp(B)=0.985 (95% CI: 0.978 to 0.992), P <0.001] was found. Thus, CD4+T cell count had an inverse association with vision-threatening posterior-segment lesions in our study (Fig. 3) and thus had worse prognosis.


- Association between the number of patients with ocular manifestations and the CD4+T-cell count.
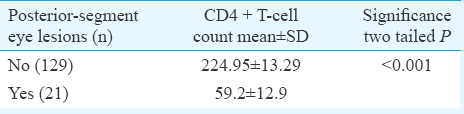
Independent sample t test to compare CD4+T cell count distribution in patients with and without posterior-segment eye lesions is shown in Table III. CD4+T cell count was low in the posterior-segment lesion patients as compared to their counterparts (P <0.001).
Discussion
According to the UNADS Global Report, there were 35.3 million people living with HIV at the end of the year 20127. According to the NACO, India has 2.5 million HIV-positive cases8. The lifetime cumulative risk of developing at least one abnormal ocular lesion among HIV positives ranges from 52 to 100 per cent2. Ocular adnexal involvement occurs in up to 25 per cent of the patients. Common adnexal lesions are HZO, molluscum contagiosum, conjunctival microvasculopathy and Kaposi's sarcoma9. In our study, five (3.3%) patients had stye, two (1.3%) had molluscum contagiosum while two (1.3%) had HZO. Anterior-segment disorders have been seen in up to 50 per cent of HIV-positive patients and include infectious keratitis (bacterial, viral, fungal, protozoal), iridocyclitis keratoconjunctivitis sicca and neoplasia10. In this study, 20 (13.3%) patients had anterior-segment lesions in the form of anterior uveitis in five (3.3%) and severe dry eyes in four (2.7%) patients. Posterior-segment manifestations are the most common, occurring in >50 per cent of the patients. Retinal microvasculopathy manifests as CWS, haemorrhages and telangiectasias11. Posterior-segment opportunistic infections include retinitis, most commonly CMV retinitis4. Only two (1.4%) patients in our study had CMV retinitis while 10 (6.7%) had CWS. Another nine (6.0%) patients had posterior-segment lesions in the form of choroiditis, optic atrophy, papilloedema and central serous retinopathy.
Both the patients with CMV retinitis had CD4+T cell count <50 cells/μl. Moreover, most of the patients with other ocular lesions fall in the groups 2-4. Group 5 included the patients with anterior-segment and adnexal manifestations. Shivayogi and Gururaj12 conducted a study of ocular manifestations of HIV/AIDS and its correlation with CD4+T cells and showed that 46 per cent of HIV-positive patients had ocular manifestations. HIV retinopathy was present in 12 per cent and CMV retinitis in seven per cent patients. Higher odds of ocular manifestations with lower CD4+T-cell count were observed in this study. Biswas et al13 evaluated ocular lesions in 100 consecutive patients at a referral eye clinic in India over a period of five years and found CMV retinitis - (17%) and HIV retinopathy (15%) as the most common HIV-associated ocular lesions. According to a study conducted on 1000 consecutive patients by Sudharshan et al14, CMV retinitis was the most common opportunistic infection. Attili et al15 analysed 460 patients for ocular manifestations of HIV/AIDS and found 88 (19%) having same eye manifestations and 54 with HIV retinopathy.
In conclusion, about 35 per cent HIV-positive patients had ocular manifestations. CD4+T cell count showed a significant inverse association with posterior segment lesions. It would be appropriate if the HIV positive individuals are subjected to routine ophthalmic examination.
Financial support & sponsorship: None.
Conflicts of Interest: None.
References
- Human immunodeficiency virus diseases: AIDS and related disorders. In: Fauci AS, Braunwald E, Kasper DL, eds. Harrison's principles of internal medicine (17th ed). Baltimore: McGraw Hill; 2008. p. :1137-46.
- [Google Scholar]
- Acute panuveitis with haemorrhagic hypopyon as a presenting feature of acquired immunodeficiency syndrome (AIDS) Indian J Ophthalmol. 2000;48:311-2.
- [Google Scholar]
- Ocular manifestations in HIV positive and AIDS patients in Nepal. Int J Clin Med. 2012;3:14-21.
- [Google Scholar]
- Posterior segment manifestations of human immunodeficiency virus/acquired immune deficiency syndrome. Indian J Ophthalmol. 2008;56:377-83.
- [Google Scholar]
- CD4 counts: A strong indicator of retinal and ocular lesions in HIV disease. Med J Armed Forces India. 2011;67:354-7.
- [Google Scholar]
- Ocular manifestation of HIV/AIDS and correlation with CD4+ cells count among adult HIV/AIDS patients in Jimma town, Ethiopia: A cross sectional study. BMC Ophthalmol. 2013;13:20.
- [Google Scholar]
- UNAIDS. Global Report: UNAIDS report on the global AIDS epidemic. 2013. Available from: http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Global_Report_2013_en_1.pdf
- [Google Scholar]
- National AIDS Control Organisation & ICMR-National Institute of Medical Statistics. Technical Report: India HIV Estimation. 2015. Available from: http://www.naco.gov.in/sites/default/files/India%20HIV%20Estimations%202015.pdf
- [Google Scholar]
- Ophthalmic manifestations of HIV in the highly active anti-retroviral therapy era. West Indian Med J. 2013;62:305-12.
- [Google Scholar]
- Anterior segment manifestations of human immunodeficiency virus/acquired immune deficiency syndrome. Indian J Ophthalmol. 2008;56:363-75.
- [Google Scholar]
- Retinal microvasculopathy is common in HIV/AIDS patients : A cross sectional study at tha Cape Coast Teaching Hospital, Ghana. J Ophthalmol. 2016;2016:8614095.
- [Google Scholar]
- Clinical study of ocular manifestations in HIV/AIDS and its correlation with CD4+ T cells. Int J Biol Med Res. 2013;4:3284-9.
- [Google Scholar]
- Ocular lesions associated with HIV infection in India: A series of 100 consecutive patients evaluated at a referral center. Am J Ophthalmol. 2000;129:9-15.
- [Google Scholar]
- Ocular lesions in 1,000 consecutive HIV-positive patients in India: A long-term study. J Ophthalmic Inflamm Infect. 2013;3:2.
- [Google Scholar]
- Ocular manifestations and human immunodeficiency virus retinopathy in patients with acquired immunodeficiency syndrome in North India. Asian J Ophthalmol. 2006;8:139-42.
- [Google Scholar]




