
Translate this page into:
Nucleophosmin mutation analysis in acute myeloid leukaemia: Immunohistochemistry as a surrogate for molecular techniques
Reprint requests: Dr Rajive Kumar, DII/44, AIIMS campus, Ansari Nagar, New Delhi 110 029, India e-mail: rajive.kumar@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Mutation of nucleophosmin (NPM1) gene in the absence of FLT3-ITD (FMS related tyrosine kinase 3 - internal tandem duplications) mutation carries a good prognosis in cytogenetically normal acute myeloid leukaemia (AML). NPM1, a multifunctional nucleolar phosphoprotein that shuttles between nucleus and cytoplasm, gets trapped in the cytoplasm when mutated. Immunohistochemical (IHC) demonstration of its aberrant cytoplasmic location (NPMc+) has been suggested as a simple substitute for the standard screening molecular method. This study was aimed to assess the diagnostic utility of IHC on formalin fixed bone marrow biopsies in comparison with the reference molecular method (allele specific oligonucleotide - polymerase chain reaction; ASO-PCR) to predict NPM1 mutation status in AML patients.
Methods:
NPM protein IHC was performed using mouse anti-NPM monoclonal antibody on 35 paraffin-embedded bone marrow biopsies of patients with primary AML of any French-American-British (FAB) subtype. Results of IHC were compared with those of ASO-PCR.
Results:
Of the 35 AML patients, 21 (60%) were positive for NPM1 exon 12 gene mutation by ASO-PCR, 19 (90.47%) of these 21 were NPMc+. Thirteen of the 35 patients were negative by both the methods. One NPMc+ patient was not detected by ASO-PCR. IHC had a sensitivity and specificity of 90 and 93 per cent, respectively, compared to the molecular screening gold standard.
Interpretation & conclusions:
Mutation of NPM1 determined by the widely available and inexpensive IHC agrees closely with results of the standard molecular methods. Thus, technically and financially not well endowed laboratories can provide the prognostically and potentially therapeutically important information on NPM1 mutation using IHC.
Keywords
AML
ASO-PCR
exon 12 mutation
immunohistochemistry
molecular surrogate
NPM1

Acute myeloid leukaemia (AML) constitutes 15-20 per cent of childhood and approximately 35 per cent of adult leukaemia1. Though morphology, cytochemistry and immunophenotype provide essential initial information about AML, it has become apparent, as is evident from the WHO classification, that the study of AML is not complete without cytogenetic and molecular evaluation2. Approximately 40-50 per cent AML cases have normal karyotype (AML-NK). Molecular analysis has identified many mutations, the frequent ones being NPM1 (Nucleophosmin1) and FLT3 (FMS related tyrosine kinase 3) and the less common ones being CEBPA gene (encoding the CCAAT/enhancer binding protein-α), C-KIT (CD117), NRAS, etc234. NPM1 gene mutations are the most common mutations and target 50 to 60 per cent of adult AML-NK2345.
Mutations in NPM1 lead to aberrant accumulation of nucleophosmin protein (NPM1) in the cytoplasm. Patients with AML with mutated NPM1 have a unique gene expression profile, distinct microRNA signature and reduced CD34 expression6. In addition, these patients are associated with increased incidence of FLT3 internal tandem duplications (ITD) in approximately 40 per cent of cases and a good response to standard chemotherapy in FLT3-ITD negative cases47. Because of these unique biological and clinical features, NPM1 mutated AML has been accorded a distinct provisional entity in the 2008 WHO classification of myeloid neoplasms and is recommended to be tested not only in clinical trials but also in routine practice2.
Molecular assays are the standard method of demonstrating NPM1 mutations. However, the requirement of sophisticated equipment and high costs are a major hindrance in their routine use in developing countries. The property of the NPM protein to get aberrantly localized to the cytoplasm of blast cells, when mutated, has been exploited to show its presence by various techniques like immunohistochemistry (IHC) and flowcytometry478.
This study was undertaken to investigate the abnormal cytochemical localization of the mutated NPM1 protein (NPMc+) in bone marrow biopsies of AML patients by IHC and correlate the results with allele-specific oligonucleotide polymerase chain reaction (ASO-PCR), one of the standard methods of assessing NPM mutation.
Material & Methods
Thirty five consecutive untreated patients diagnosed on morphology, cytochemistry and flow cytometry with AML were studied in All India Institute of Medical Sciences, New Delhi, India, during July 2012 to June 2013. Assuming anticipated sensitivity and specificity as 90 per cent and absolute precision of 10 per cent with 95 per cent confidence level (i.e. 95% confident of detecting the true sensitivity and specificity of IHC with ASO-PCR between 75-100%); we required 15 confirmed cases and 15 confirmed controls.
Bone marrow biopsies for IHC and either peripheral blood or bone marrow aspirates for ribonucleic acid (RNA) isolation were collected after obtaining informed consent. The study protocol was approved by the AIIMS medical ethics committee.
Immunohistochemistry for NPM protein localization using mouse anti-NPM monoclonal antibodies (Isotype IgG1, lambda, clone 376: DAKO, Denmark) was performed on the bone marrow biopsies of all the patients by the standard protocol9. The dilution of the antibody used was 1:100. Nucleus restricted NPM immunostain was considered as negative for NPM1 gene mutation while cytoplasmic localization of the immunostain was considered as a positive result. Nuclear staining of NPM immunostain served as an internal control in the study population. These antibodies recognize both the wild-type NPM and the NPM leukaemic mutants47.
NPM1 gene mutation was detected on bone marrow or peripheral blood samples by ASO-PCR as described by Ottone et al10. Briefly, total RNA was extracted from Ficoll-Hypaque-isolated mononuclear cells (bone marrow aspirate or peripheral blood, if the latter had >40% blasts) by TriZol reagent (Thermo Fisher Scientific, India) according to the manufacturer's instruction. RNA was reverse-transcribed to cDNA for using as template and PCR reaction was performed. A 320-bp fragment was amplified from 2 μl of cDNA in a total volume of 25 μl of the reaction mixture containing 10 pmol of each primer, NPM-A and NPM-REV-6, 1x PCR buffer, 2.5 mmol/l MgCl2, 5 mmol/l deoxynucleo-side-5’-triphosphates and 2.5 U of Taq polymerase (Thermo Fisher Scientific, Fermantas, Vilinus, Lithuania). The forward NPM-A primer and reverse NPM-REV-6 primer used in the study were 5’-CCAAGAGGCTATTCAAGATCTCTCTC-3’ and 5’-ACCATTTCCATGTCTGAGCACC-3’, respectively. ABL1 (Abelson murine leukaemia viral oncogene homologue 1) amplification with the same ASO-reverse transcription (RT)-PCR conditions was used as internal PCR control. The forward ABL-A2B-5’ primer and reverse ABL-A3E-3’ primer used were 5’-GCATCTGACTTTGAGCCTCAG-3’ and 5’-TGACTGGCGTGATGTAGTTGCTT-3’, respectively10.
Preheating of the mixture at 95°C for seven min was followed by 35 cycles of 30 sec at 95°C, 45 sec at 67°C, and 45 sec at 72°C. A final extension of seven min was performed at 72°C on a Veriti Thermal Cycler (Applied Biosystems, USA). The amplified products were visualized by UV light on ethidium bromide stained 2 per cent (w/v) agarose gel electrophoresis. All recommended precautions were taken to avoid contaminations. The NPM1 exon 12 gene mutation was detected when a sharp band of 320 bp was present. ABL amplification led to a discrete band at 258 bp.
Statistical analysis: The diagnostic utility of IHC was deduced by taking ASO-PCR as the gold standard test and standard statistical formulae for sensitivity, specificity, positive and negative predictive values were applied. Kappa correlation was computed to see the concordance of results between IHC and ASO-PCR. Also, Fisher's exact test was used to detect concordance between NPM1 mutational status by ASO-PCR and FAB (French-American-British) classification2.
Results
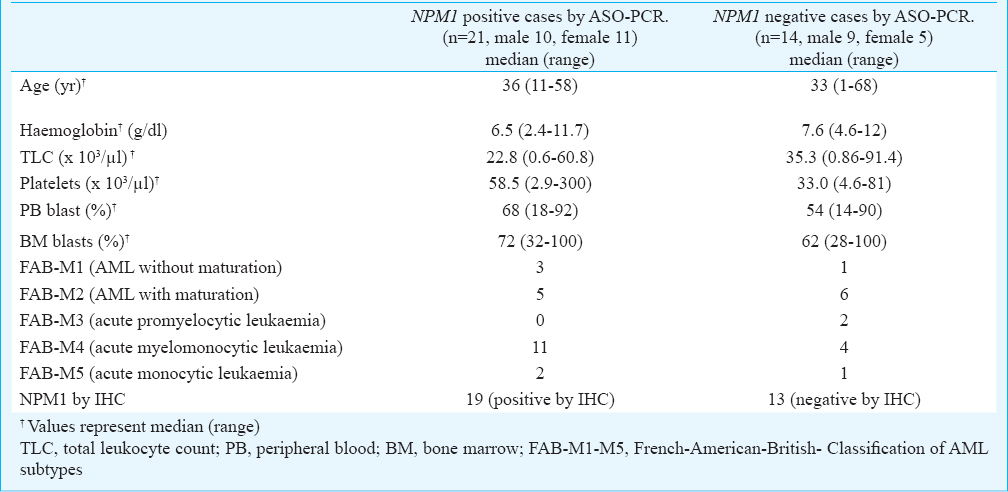
Thirty five patients (19 male/16 female; 12 children / 23 adults) were evaluated for NPM mutation in this study. The patients had a wide age-group ranging from one year old child to 68 yr old adult (median 33; range 1-68 yr). Of these, 21 (60%) were positive for NPM1 exon 12 gene mutation as detected by ASO-PCR (Fig. 1). Both the NPM1 positive and negative groups were heterogeneous with respect to patient profile and there was no significant correlation between the demographic details (gender distribution, age, haemoglobin, total leukocyte count, platelet count, blast percentage both in peripheral blood and bone marrow and FAB classification) and the NPM1 mutation status (Table).
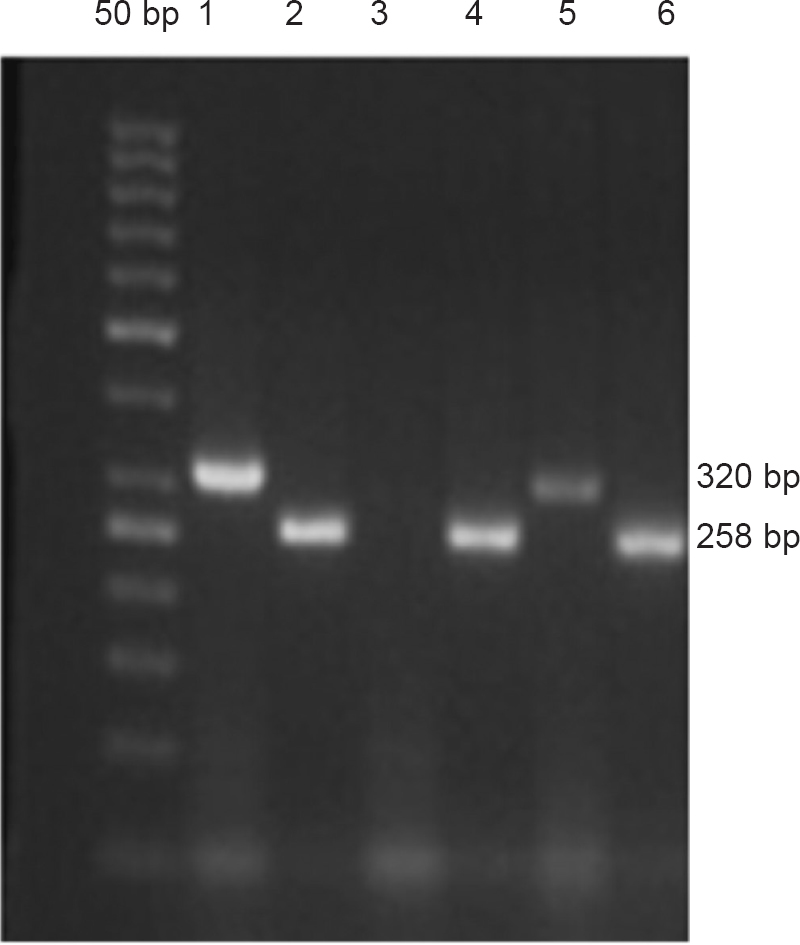
- Agarose gel (2%) electrophoresis of ASO-PCR amplified products: An amplification band of 320 bp containing the NPM1A mutation is visualized in two patient samples (lanes 1 and 5), whereas no amplification signal is visible in one patient sample (lane 3). Successful amplification of the ABL gene was used in all cases as internal PCR control (lanes 2, 4 and 6).
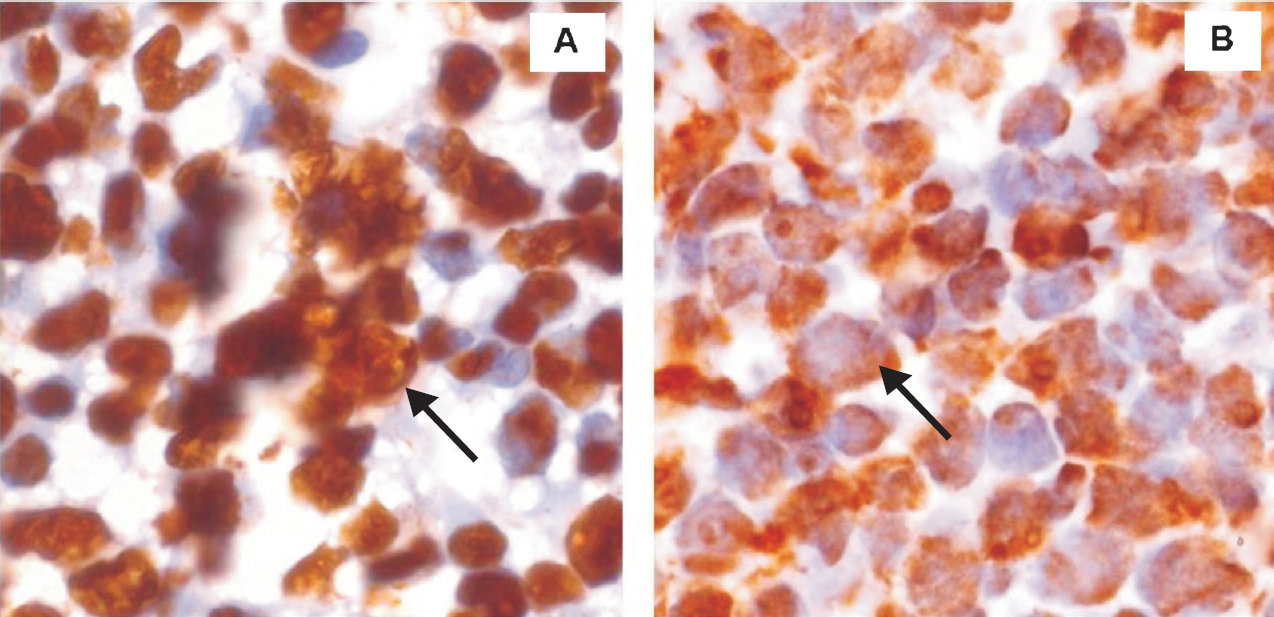
Nineteen of the 21 patients (90.47%) positive by ASO-PCR also demonstrated NPMc+ by IHC (Fig. 2). Only two patients who were positive for NPM1 exon 12 gene mutation by molecular studies were missed by immunohistochemistry technique. One patient who was IHC positive was not picked up by ASO-PCR. Judging against ASO-PCR as the standard gold standard test for detection of NPM1 gene mutation, IHC had a sensitivity of 90 per cent [confidence interval (CI): (69.6 - 98.8)], specificity 93 per cent (CI: 66.1 - 99.8), positive predictive value 95 per cent (CI: 75.1 - 99.8) and negative predictive value of 87 per cent (CI: 57.2 - 98.2). Thirteen patients were negative by both PCR and IHC. Kappa statistics revealed almost complete agreement (κ=0.8235; 95% confidence interval: 0.6326-1) between IHC and ASO-PCR for NPM1 mutation status.
-
(A). Leukaemic cells from bone marrow biopsy of patient with acute myeloid leukaemia with wild-type NPM1 show nucleus-restricted NPM staining (arrow) (x1000). (B). Bone marrow biopsy from an NPMc+ patient with AML bearing NPM mutation A. Leukaemic cells show cytoplasmic expression of NPM (arrow) (x1000).
Discussion
In our study, a good agreement was found between NPMc+ by IHC and the presence of exon-12 NPM mutations by ASO-PCR. Our results were consistent with previous studies911. They reported 100 per cent specificity and sensitivity of IHC to detect NPM1 gene mutation. In our study, there was discordance in three cases between the two test results. One case was positive by IHC but not by ASO-PCR. This can be explained by the fact that ASO-PCR is a highly analytically specific test and can detect mutant clones that represent as little as 0.001 per cent of the population. However, this assay detects only the NPM1A mutation10, which although is most common (75 to 80% of cases) but is not seen in approximately 20 per cent of the cases10. NPMc+ by IHC besides being caused by the NPM1A mutation can also be caused by other variants of NPM1 mutations1213. In this patient, more extended exon screening test was required but due to cost constraints this could not be done. Two patients positive by PCR assay were not detected by IHC. This could be because mutated NPM1 does not always reveal overt cytoplasmic staining of NPM1 on formalin fixed bone marrow biopsies12. The NPM1c+ detection can be improved by analyzing thin 2-3 μm sections and using B5 fixative instead of formalin12. However, the potential toxicity of mercuric chloride containing B5 fixative and waste disposal hazards are major disadvantages. Such discrepancies have been recorded and studied extensively by Woolthuis et al12. They detected discordant results between the two tests in 6 of 119 (5%) patients and concluded that detection of NPM1 mutations for routine screening of newly diagnosed AML patients should optimally be based on both IHC and molecular analyses. Konoplev et al13 who analyzed mutations by DNA sequencing found discordant results in 18 of 104 (16.6%) cases and concluded that DNA sequencing was not be replaced by IHC. Also, IHC assessment for cytoplasmic NPM localization did not predict prognosis in their patients. The present study showed a discrepancy in three among all (8.6%) cases.
In this study, 60 per cent patients were positive for NPM1 exon 12 gene mutation as detected by ASO-PCR. This percentage was higher than that reported previously127 but could be explained by the fact that the patients were randomly chosen in whom bone marrow biopsy were available for this study. Thus, the frequency of the NPM1 gene mutation as detected in this study would not be truly reflective of the disease prevalence.
NPM1 gene mutations are associated with increased incidence of FLT3-ITD and a good response to standard chemotherapy in FLT3-ITD negative cases247. Surrogates for molecular studies are expected to be particularly useful in older patients where NPM1 mutations appear to play a prognostic role independently of the FLT3 gene status14. For younger patients, whose favourable prognosis is associated with the NPM1-mutated/FLT3-ITD negative genotype415, inexpensive assays are needed which can allow assessment of the FLT3 gene status.
Immunohistochemistry has a high specificity and sensitivity to detect mutated NPM1 gene when performed on formalin fixed bone marrow biopsies. The unique IHC pattern in bone marrow biopsies seems to be an excellent surrogate marker for molecular studies. Advantages include being fully predictive of NPM1 mutations for both the exon 12 as well as the other less common ones. Additionally, IHC is critical for diagnosis of AML cases presenting with dry tap or as myeloid sarcoma12. Though discordance of results was seen in our study, in the context of developing countries, IHC is widely available bringing NPM1 mutation testing within the reach of even less well-endowed laboratories. For the same reason, more physicians treating AML can better assess their patients with respect to the disease process. However, further studies are needed to elucidate the relevance of different factors that might contribute to discordant results between both the techniques.
Conflicts of Interest: None.
References
- Nucleophosmin (NPM1) mutations in adult and childhood acute myeloid leukaemia: towards definition of a new leukaemia entity. Hematol Oncol. 2009;27:171-81.
- [Google Scholar]
- Acute myeloid leukemia with recurrent genetic abnormalities. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, eds. WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon. France: IARC; 2008. p. :110-22.
- [Google Scholar]
- Molecular genetics of adult acute myeloid leukemia: prognostic and therapeutic implications. J Clin Oncol. 2011;29:475-86.
- [Google Scholar]
- Acute myeloid leukemia carrying cytoplasmic/mutated nucleophosmin (NPMc+ AML): biologic and clinical features. Blood. 2007;109:874-85.
- [Google Scholar]
- Molecular heterogeneity and prognostic biomarkers in adults with acute myeloid leukemia and normal cytogenetics. Curr Opin Hematol. 2005;12:68-75.
- [Google Scholar]
- CD34+ cells from AML with mutated NPM1 harbor cytoplasmic mutated nucleophosmin and generate leukemia in immunocompromised mice. Blood. 2010;116:3907-22.
- [Google Scholar]
- NPM1 mutations and cytoplasmic nucleophosmin are mutually exclusive of recurrent genetic abnormalities: a comparative analysis of 2562 patients with acute myeloid leukemia. Haematologica. 2008;93:439-42.
- [Google Scholar]
- Rapid flow cytometric detection of aberrant cytoplasmic localization of Nucleophosmin (NPMc) indicating mutant NPM1 gene in acute myeloid leukemia. Leukemia. 2010;24:1813-6.
- [Google Scholar]
- Immunohistochemistry predicts nucleophosmin (NPM) mutations in acute myeloid leukemia. Blood. 2006;108:1999-2005.
- [Google Scholar]
- An allele-specific rt-PCR assay to detect type A mutation of the nucleophosmin-1 gene in acute myeloid leukemia. J Mol Diagn. 2008;10:212-6.
- [Google Scholar]
- Cytoplasmic expression of nucleophosmin accurately predicts mutation in the nucleophosmin gene in patients with acute myeloid leukemia and normal karyotype. Am J Clin Pathol. 2010;133:34-40.
- [Google Scholar]
- A single center analysis of nucleophosmin in acute myeloid leukemia: value of combining immunohistochemistry with molecular mutation analysis. Haematologica. 2013;98:1532-8.
- [Google Scholar]
- Cytoplasmic localization of nucleophosmin in bone marrow blasts of acute myeloid leukemia patients is not completely concordant with NPM1 mutation and is not predictive of prognosis. Cancer. 2009;115:4737-44.
- [Google Scholar]
- Favorable prognostic impact of NPM1 mutations in older patients with cytogenetically normal de novo acute myeloid leukemia and associated gene- and microRNA-expression signatures: a cancer and leukemia group B study. J Clin Oncol. 2010;28:596-4.
- [Google Scholar]
- Mutations and treatment outcome in cytogenetically normal acute myeloid leukemia. N Engl J Med. 2008;358:1909-18.
- [Google Scholar]




