
Translate this page into:
Multisystem Langerhans cell histiocytosis: A diagnostic chameleon
*For correspondence: diptigothi@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 32 yr old non-smoker female† reported to the department of Dermatology, ESI-PGIMSR (Employee State Insurance-Postgraduate Institute of Medical Sciences & Research), New Delhi, India, in November 2018, for remitting and relapsing rashes all over the body for the last two years (Fig. 1A and B) with low-grade fever, malaise and weight loss. Routine haematological investigations were normal. The skin biopsy of the thigh region showed epithelioid cell granuloma with necrosis. The patient was started on anti-tubercular therapy. She was referred to the Pulmonary Medicine department for cough and abnormal chest radiograph (Fig. 2A) and the high-resolution computed tomography (HRCT) of the chest (Fig. 2B and C). The sputum was negative for acid-fast bacilli. The skin biopsy of the patient was re-evaluated as the radiological findings were not indicative of tuberculosis. On immunohistochemical staining, it was positive for S-100 and CD1a (Fig. 3A and B) confirming the diagnosis of systemic Langerhans cell histiocytosis. The patient had near-normal lung function on spirometry with 48 per cent diffusion capacity of carbon monoxide. At six months of follow up, the forced vital capacity dropped by 200 ml, but still was 77 per cent predicted. The patient is continued on oral prednisolone of 5 mg/day, with her symptoms controlled.
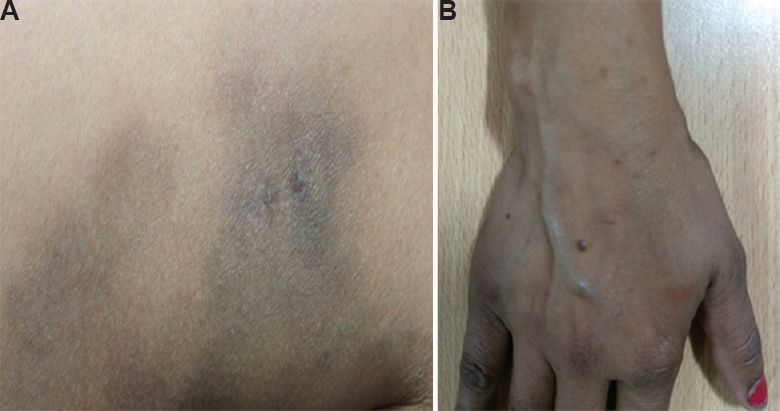
- (A) Hyperpigmented ill-defined macular rash on medial aspect of the right thigh. (B) Petechial rashes on the hand and forearm.
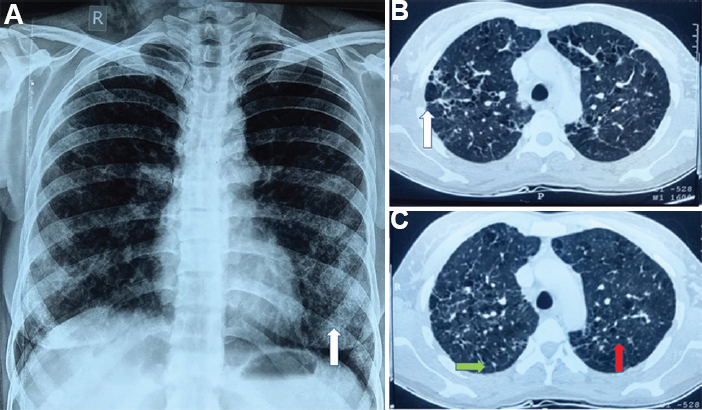
- (A) X-ray chest posteroanterior view showing bilateral reticular opacity (white arrow). (B & C) High-resolution computed tomography chest lung window showing septal thickening (green arrow), randomly distributed bizarre cysts (white arrow) and multiple centrilobular nodules (red arrow).
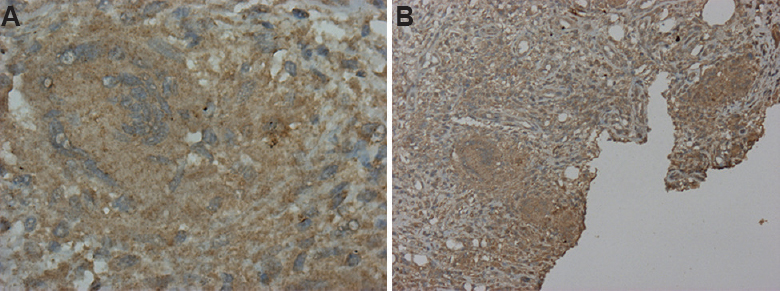
- (A) Photomicrograph of skin biopsy (×10); positive for CD1a. (B) Photomicrograph of skin biopsy showing epithelioid cell granuloma positive for CD1a (×40).
Acknowledgment:
Authors acknowledge Dr Ritu Kulshreshtha, department of Pathology, Vallabhbhai Patel Chest Institute, New Delhi, for providing illustrated histopathological images and their interpretations.
Conflicts of Interest: None.




