
Translate this page into:
Melioidosis
* For correspondence: ak_md2000@yahoo.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 21 yr old woman† from an urban locality with no travel history presented to the Emergency department at Vadamalayan Hospital, Madurai, India, in August 2015, with intermittent fever for two months. She had type 2 diabetes mellitus (body mass index 28 kg/m2, presence of acanthosis) for six months with a poor preceding glycaemic control (glycated haemoglobin, HbA1c - 10.6%). She was delirious, icteric, tachycardic and hypotensive. Investigations revealed anaemia, leucocytosis, hyperbilirubinaemia and hyperglycaemia. Infectious screens for malaria, leptospirosis, hepatitis and dengue were negative. Half-Fourier Acquisition Single-Shot Turbo Spin-Echo coronal and axial abdomen magnetic resonance imaging revealed hepatic and splenic bright signals suggestive of abscesses (Fig. A and B). Although uncommon, the history of visceral abscesses in a young individual with diabetes is suggestive of melioidosis. This was confirmed on splenic pus aspirate Gram stain (Fig. C and D), culture and blood culture. The patient recovered completely with intravenous ceftazidime (2 g thrice daily) for two weeks followed by oral co-trimoxazole and sulphamethoxazole for 12 wk. The patient recovered completely with complete regression of the visceral abscesses on further follow up after three months.
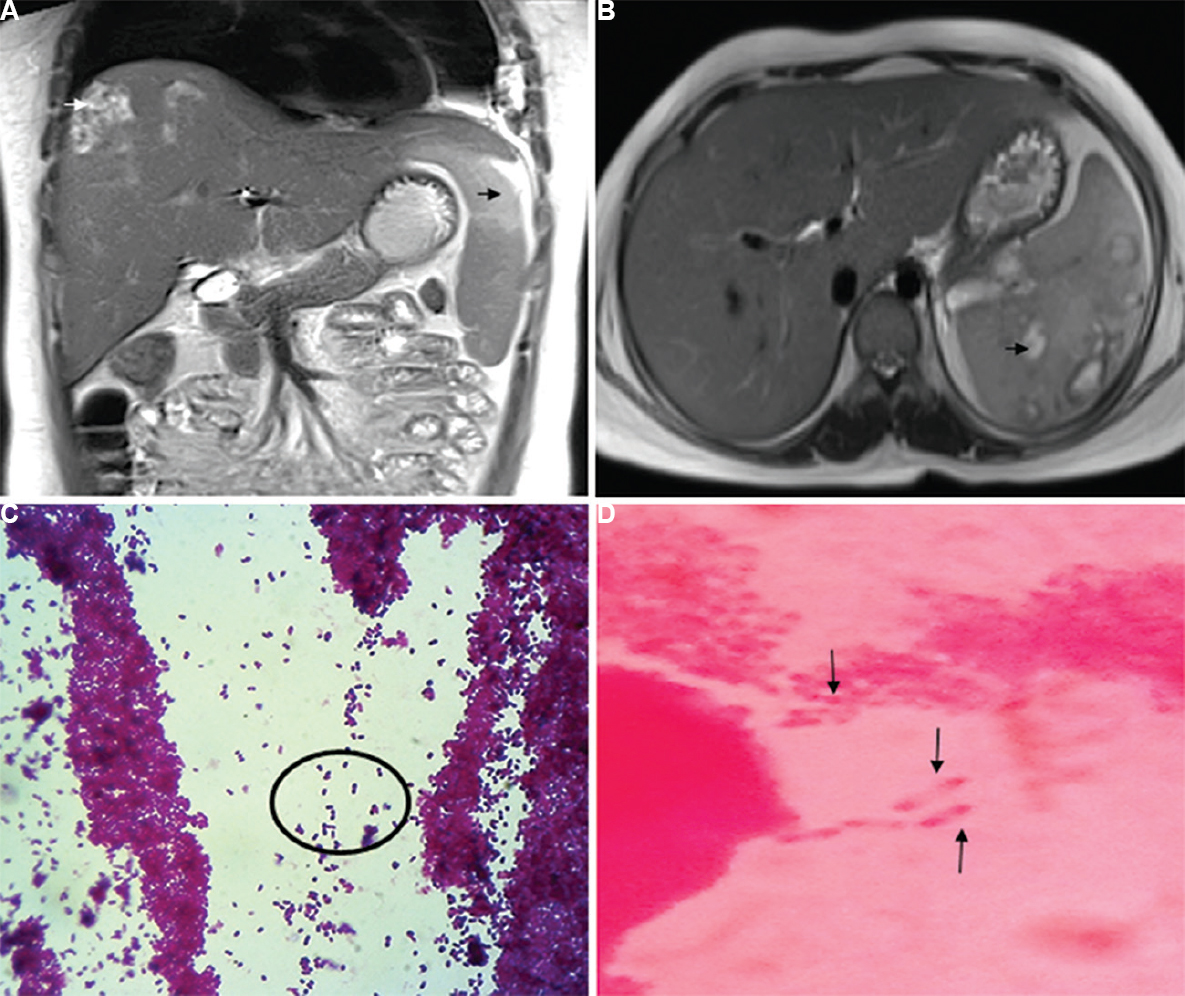
- (A) Half-Fourier Acquisition Single-Shot Turbo Spin-Echo coronal abdomen magnetic resonance imaging showing hepatic and splenic bright signal intensities suggestive of abscesses (black and white arrows). (B) Half-Fourier Acquisition Single-Shot Turbo Spin-Echo axial abdomen magnetic resonance imaging showing hepatic and splenic bright signal intensities suggestive of abscesses (arrow). (C) Gram stain of splenic pus aspirate (×40) showing Gram-negative bacilli, bipolar stained with a safety pin appearance (circle). (D) Splenic aspirate pus Gram stain (×100) oil immersion field shows many bipolar-stained (pink-coloured) Gram-negative bacilli giving a safety pin appearance.
Disseminated melioidosis has a high fatality rate and could be caused by inhalation, ingestion or percutaneous inoculation of a Gram-negative bacterium Burkholderia pseudomallei present in the soil. Diabetes has been described as a major risk factor of melioidosis in up to 60 per cent of cases. It is important to highlight that a clinical suspicion of melioidosis is necessary in an individual with fever, multiple visceral abscesses and predisposing risk factors like diabetes even in a non-endemic area.
Conflicts of Interest: None.




