
Translate this page into:
Maternal demography, clinical characteristics, & outcomes at an obstetric intensive care unit of a tertiary-care teaching maternity hospital in the Kashmir Valley
For correspondence: Dr Elias Mir, Department of Chest Medicine, Sher-i-Kashmir Institute of Medical Sciences Medical College, Srinagar 190 017, Jammu and Kashmir, India e-mail: eliasjnmc@gmail.com
-
Received: ,
Accepted: ,
Abstract
Background & objectives
Obstetric patients often need admission to intensive care units (ICUs). The data on these patients are scarce and heterogeneous. We studied the profile of obstetric patients admitted to our ICU.
Methods
The records of obstetric patients admitted to the ICU at the Government Lalla Ded Hospital, Srinagar, Jammu and Kashmir, India, dedicated to obstetrics and gynaecology patients, were analysed retrospectively from March 2022 to February 2023.This included demography, co-morbidities, pre-admission surgeries/procedures, clinical characteristics, and outcomes (death/discharge/transfer).
Results
Out of 525 obstetric ICU patients, the majority were admitted for obstetric causes (94.66%) and after surgery (84.38%), mostly (66.59%) after caesarean section (CS). Hypertension (35.23%) and anaemia (32.76%) were the most common co-morbidities. The majority were admitted for hypertensive disorders of pregnancy (HDP; 34.47%) or post-partum haemorrhage (PPH; 24.71%) or complications. Only two per cent of CS and one per cent of vaginal delivery (VD) patients needed ICU admission. The maternal ICU mortality rate was 6.53 per cent (0.15% of total deliveries). Only 6.66 per cent needed transfer to non-obstetric or multi-specialty care. Admission with heart disease [Hazard ratio; HR=8.26, 95% Confidence interval (CI)=0.01-67.17,P<0.05], after intra-uterine foetal death (IUFD; HR=5.17, 95% CI=1-26.75, P<0.05), or after laparotomy for ectopic pregnancy (EP; HR=50.2, CI=1.43-1766.87, P<0.05) and need for invasive mechanical ventilation (IMV; HR=35.5, CI=3.14-401.75, P<0.05) or inotropic support (IS; HR=12.06, CI=1.96-74.19, P<0.05) increased while admission after VD (HR=0.10, CI=0.01-0.73, P<0.05) decreased mortality risk.
Interpretation & conclusions
HDP and PPH were the most common maternal presentations in obstetric ICUs. Maternal mortality was low. Patients with heart diseases, IMV/IS requirement, and those admitted after IUFD or laparotomy for EP had increased, while patients admitted after VD had decreased mortality risk in the ICU.
Keywords
Ectopic pregnancy
intrauterine foetal death
maternal mortality
maternal near-miss
obstetric critical care
obstetric ICU

Females undergo profound anatomical and physiological changes during pregnancy and puerperium. These changes are adapted by the female body to sustain foetal development during pregnancy and subsequent delivery at term1. However, this increased metabolic load may unmask underlying diseases and co-morbidities and make the mother’s body vulnerable to complications2. Frequent requirement of invasive interventions also exposes these mothers to surgical and anaesthetic complications2-4. Obstetric patients are, therefore, at greater risk of potentially fatal complications than normal adult population2,3. Consequently, many obstetric patients require invasive mechanical ventilation (IMV), inotropic support (IS), and blood transfusions among other interventions, which require admission to intensive care units (ICUs)2-4. With advances in the management of many chronic diseases, more high-risk patients with co-morbidities are conceiving and surviving pregnancies. This is further expected to increase the number of obstetric patients in ICUs5,6.
In recent times, globally enhanced quality and availability of healthcare has improved maternal-foetal outcomes4-6. However, there is still a tremendous disparity in the human and material resources available worldwide for such needs3-6. This disparity is seen even among different areas of the developed countries3-6. High maternal and foetal morbidity and mortality persist in certain parts of the world3. Reducing maternal mortality rate is therefore an important goal of the ‘The 2030 Agenda for Sustainable Development’ envisioned by the United Nations in 20157.
In recent times, severe acute maternal morbidity (SAMM) and maternal near-miss have gained recognition as measures of quality of obstetric health care4. These include critically ill patients who narrowly escape death due to obstetric or non-obstetric complications but do not contribute to the maternal mortality ratio. However, these patients may be left with severe morbidities requiring admission to ICUs and, at times, prolonged health infrastructure support2-6.
The available data on obstetric patients requiring ICU admission are scarce and heterogeneous8-23. Among the published studies, the difference in the quality of centres, studied populations, characteristics of the admitted patients, and clinical outcomes is remarkable8-23. The causes of ICU admissions in obstetric patients, however, remain uniform across the globe, with hypertensive disorders of pregnancy (HDP) and its complications, obstetric haemorrhage (OH), and sepsis forming the bulk8-23. The maternal ICU mortality rates vary significantly from less than two per cent in developed countires21-23 to almost 50 per cent in certain centres14,16 in developing country settings. Considering this paucity and heterogeneity of information, and a requirement for a continuous update on these data, we conducted a retrospective study of the demography, clinical characteristics, and outcomes of obstetric patients who needed admission to ICU at our centre.
Materials & Methods
The study was done at the department of Obstetrics and Gynaecology (OBG), Government Lalla Ded Hospital, a teaching tertiary-care maternity hospital, Government Medical College, Srinagar, Jammu and Kashmir, India. The centre, dedicated to the patients of OBG, is located in the picturesque Kashmir Valley in the Northern Himalayan region of South Asia. In addition to the Kashmir Valley, the hospital also receives referrals from the adjoining Chenab Valley and the Pir Panjal region of the Jammu division as well as the Union territory of Ladakh. This region has a population of approximately 10 million and consists of both urban centres as well as rural areas that include places deep within the Himalayas with difficult mountainous terrain. This study was a retrospective cohort study initiated after obtaining Institutional approval from the Institutional Review Board, Government Medical College, Srinagar, Jammu, and Kashmir, from March 2022 to February 2023.
On average, the hospital attends to approximately 500 patients of OBG per day in the outpatient department (OPD). The OBG admissions vary between 80 to 150 patients daily. The in-patient department (IPD) has a capacity of 750 beds with occupancy of at least 80 per cent throughout the year. The hospital has 24-h emergency service, including operation theatres, a blood bank, and an ICU with four beds dedicated to the patients of OBG. The ICU is level 324, semi-open, and attended by the department of Anaesthesia and Critical Care (ACC) and the department of OBG. Specialists from other medical and surgical departments are available on call round the clock whenever needed. The centre also has a high-dependence unit with 12 beds used as an intermediate level of care between IPD and ICU. Patients are admitted to ICU only after a collective decision by intensivists and OBG specialists. In case patients require specific procedures or care not available at the centre, intensive care ambulances are used to transport the patients to other centres of the Government Medical College, Srinagar, located in the same city within a distance of 5 km. The hospital also has an in-house neonatal ICU.
Study sample
The records of all obstetric patients admitted to our centre’s ICU from March 2022 to February 2023 were retrieved using the hospital record system including ICU registers, ICU charts, IPD registers, operation theatre records and the individual case files of the patients. All the patients admitted to the ICU during pregnancy or within 42 days of delivery were included in the study. A senior OBG specialist recorded the data with the help of a resident doctor. At least 90 per cent of the data was cross-checked by another Critical Care specialist.
Variables studied
The data compiled included demographic characteristics, co-morbidities, diagnosis at admission, and type of surgery (in case of post-operative patients) done before admission to the ICU. Interventions in the ICU, like endo-tracheal intubation, IMV, non-invasive ventilation (NIV), inotropic support, and blood transfusion were also recorded. The outcome data comprised of the duration of stay in ICU in hours, referral to other centres for non-OBG or multi-specialty care, death, discharge from the hospital, or shift to a lower level of care like HDU or IPD. In addition, the total number of OPD patients seen, patients admitted to IPD, patients admitted to ICU, surgeries done and vaginal deliveries (VD) conducted by the hospital during the study period was also retrieved.
Statistical analysis
The categorical variables were recorded as numbers and percentages of the total were estimated. The continuous variables were summarised as mean±standard deviation (SD). Multivariate cox regression analysis was used to determine the association of variables with the mortality risk. For the significance of this model likelihood ratio test was used. R software version 4.4.0 was used to fit the cox regression proportional model using survival package25.
Results
During the study period, our centre attended to 1,59,839 patients in OPD and admitted 32,665 patients to the IPD. Of the admitted patients, 22,745 (69.63%) belonged to rural areas, and 9920 (30.36%) belonged to urban centres. A total of 20,676 deliveries were conducted during the study period, out of which 14,100 (68.19%) had caesarean sections (CS) and 6576 (31.8%) had VD (Table I). A total of 583 patients were admitted to the ICU during the given time frame (Table I). Out of these, 525 (90.05%) were obstetric patients and the rest were gynaecology patients. A majority (76%) of the obstetric patients admitted to the ICU belonged to rural areas (Table I). Only three (0.57%) patients were unmarried (Table I).
| Variable studied | n (%) |
|---|---|
| Number of patients seen in OPD | 159839 |
| Number of patients admitted in IPD (P) | 32665 |
| Patients admitted residing in rural areas | 22745 (69.63%) |
| Patients admitted residing in urban areas | 9920 (30.36%) |
| Total deliveries conducted (Q) | 20676 |
| Deliveries by caesarean section | 14,100 (68.19%) |
| Deliveries by vaginal delivery | 6,576 (31.81%) |
| Total patients admitted to ICU (R) | 583 |
| Total gynaecology patients admitted to ICU | 58 (9.94) |
| Total obstetric patients admitted to ICU (N) | 525 (90.05) |
| Age (mean±standard deviation) | 30.07 ± 4.58 |
| Age (yr; min–max) | 18 – 43 |
| 10-29 | 243 (46.29) |
| 30-39 | 274 (52.19) |
| 40-49 | 8 (1.52) |
| Married | 522 (99.42) |
| Rural | 399 (76) |
| Urban | 126 (24) |
| Hypertension | 189 (35.23) |
| Anaemia | 172 (32.76) |
| Diabetes | 65 (12.38) |
| Heart disease | 49 (9.33) |
| Epilepsy | 25 (4.76) |
| Kidney disease | 19 (3.61) |
| Lung disease | 24 (4.57) |
| Liver disease | 35 (6.66) |
OPD, out-patient department; IPD, in-patient department; ICU, intensive care unit
Hypertension, including both essential hypertension and hypertensive disorders of pregnancy (HDP; including pre-eclampsia, eclampsia, and pregnancy-induced hypertension), was the most common co-morbidity seen in 35.23 per cent of patients, followed by anaemia (32.76%) and diabetes (12.38%; Table II).
| Variable studied | n (%) |
|---|---|
| Total number of patients admitted to intensive care unit (N) | 525 |
|
Diagnosis in patients admitted for obstetric reasons- total (percent of N) (one patient can have more than one condition) |
499 (95.04) |
| Hypertensive disorder of pregnancy and complications | 159 (30.28) |
| Post-partum haemorrhage | 130 (24.76) |
| Placenta praevia | 79 (15.04) |
| Eclampsia | 65 (12.38) |
| Intra-uterine foetal death | 50 (9.52) |
| Abortion | 46 (8.76) |
| Abruption | 43 (8.19) |
| Twin delivery | 37 (7.04) |
| Ectopic pregnancy | 33 (6.61) |
| Post-operative/obstetric sepsis | 23 (4.38) |
| Uterine rupture | 4 (0.76) |
| Diagnosis in patients admitted for non-obstetric reasons - number (percent of N) | 26 (4.95 %) |
| Anaphylaxis | 2 (0.38) |
| Pulmonary complications | 7 (1.33) |
| Community-acquired pneumonia | 3 (0.57) |
| Hospital-acquired pneumonia | 1 (0.19) |
| Status asthmaticus | 2 (0.38) |
| Interstitial lung disease | 1 (0.19) |
| Cardiac causes | 8 (1.52) |
| Valvular heart disease | 3 (0.57) |
| Arrhythmia | 2 (0.38) |
| Cardiomyopathy | 3 (0.57) |
| Diabetic keto-acidosis | 3 (0.57) |
| Acute kidney failure | 2 (0.38) |
| Portal hypertension with gastric bleed | 1 (0.19) |
| Status epileptics | 1 (0.19) |
| Anaesthesia related complications | 2 (0.38) |
Most (95.04%) patients were admitted to the ICU due to obstetric causes (Table II). HDP (30.28%) along with post-partum haemorrhage (PPH; 24.76%) were the two most common conditions seen in obstetric patients needing admission to ICU. Other causes of obstetric haemorrhage (OH), like placenta praevia (15.04%), abruption (8.19%), and uterine rupture (0.76%), were also recorded (Table II). Other critical clinical conditions in these patients were intra-uterine foetal death (IUFD; 9.52%), twin pregnancy (7.04%), and post-operative sepsis (4.38%; Table II). Patients admitted for eclampsia were 12.38 per cent of these patients (Table II).
Non-obstetric medical and surgical causes were responsible for only 4.95 per cent of the admissions to the ICU. These included patients who presented with anaphylaxis (0.38%), pulmonary (1.33%), cardiac (1.52%), renal (0.38%), neurological (0.19%), hepatic (0.19%), and diabetic (0.57%) complications (Table II).
Most obstetric patients (84.38%) were admitted to ICU after surgery (Table III). Of these 357 (80.58%) were emergency and 86 (19.41%) were elective surgeries. CS was the most common (66.59%) surgery done in these patients. Of the 14,100 CS done at the hospital, only 2.09 per cent of patients needed ICU admission (Tables I and III). These formed 56.19 per cent of all obstetric ICU admissions. Hysterectomy done at the time of caesarean section comprised 11.28 per cent of the surgical obstetric cases needing ICU admission (Tables I and III). Of the 6576 vaginal deliveries conducted at our hospital during this period, only 66 (approximately 1%) were admitted to ICU. These formed 12.57 per cent of the total obstetric patients admitted to ICU (Tables I and III). Laparotomy for ectopic pregnancy (EP; 6.77%) was another common surgery done in these patients before ICU admission (Table III).
| Variable studied | n (%) |
|---|---|
| Total number of patients admitted to intensive care unit (N) | 525 |
| Vaginal delivery | 66 (12.57) |
| Total surgeries | 443 (84.38) |
| Elective | 86 (19.41) |
| Emergency | 357 (80.58) |
| Caesarean section | 295 (66.59) |
| Caesarean hysterectomy | 50 (11.28) |
| Laparotomy for ectopic pregnancy | 30 (6.77) |
| Exploratory laparotomy | 27 (6.10) |
| Dilatation and curettage | 23 (5.19) |
| Manual removal of placenta | 14 (3.16) |
| Caesarean myomectomy | 1 (0.22) |
| Laparoscopy for ectopic pregnancy | 3 (0.67) |
In the ICU 22.28 per cent of patients needed invasive mechanical ventilation (IMV), whereas only six per cent were managed by NIV. Inotropic support (IS) was required in 98 (18.66%) patients. Blood transfusion was needed in 50 per cent of the patients. Most patients (87.23%) were successfully discharged or shifted to a lower level of care like ward or HDU. Only 35 (6.66%) of the obstetric patients in ICU needed transfer to another centre for non-OBG or multi-specialty care which was not possible at our centre (Table IV).
| Variable studied | n (%) |
|---|---|
| Total number of patients admitted (N) | 525 |
| Invasive mechanical ventilation | 117 (22.28) |
| Non-invasive ventilation | 32 (6.09) |
| Oxygen supplementation | 219 (41.71) |
| Inotropic support | 98 (18.66) |
| Blood (component) transfusion | 263 (50.09) |
| ICU duration in h (range: Min - Max) | 4 - 336 |
| ICU duration in h; mean (standard deviation) | 33.02 (70.99) |
| Death* | 32 (6.53) |
| Transfer out (for non-obstetric/multi-specialty care) | 35 (6.66) |
| Downgraded care (shifted to ward/discharged) | 458 (87.23) |
A total of 32 obstetric patients died in our ICU during the study period. After excluding the patients transferred out, the net ICU mortality rate for obstetric patients admitted to our ICU was 6.53 per cent (Table IV). We did not have the mortality data of the patients transferred out of our centre.
Both antepartum and post-partum obstetric haemorrhage, was the main obstetric condition in patients who died after admission to ICU. Most of the patients died after emergency surgeries, the most common of which was the caesarean section done with (12.48%) or without hysterectomy (31.25%). Six patients (18.72%) died after exploratory laparotomy out of which 2 had ruptured ectopic pregnancy. Six patients (18.72%) died due to sepsis. Intrauterine death occurred in 1/3rd of the patients before death (Table V).
| Total no. of deaths (n) = 32 | ||
|---|---|---|
| Obstetric/non-obstetric diagnosis | n (%) | |
| Obstetric causes/conditions | Intra-uterine death | 10 (31.2) |
| Twin pregnancy | 1 (3.12) | |
| Eclampsia | 5 (15.6) | |
| Abruption | 3 (9.36) | |
| Placenta praevia | 2 (6.24) | |
| Post-partum haemorrhage | 9 (28.08) | |
| Ruptured ectopic pregnancy | 2 (6.24) | |
| Non-obstetric causes/comorbidities | Hypertension | 13 (40.56) |
| Anaemia | 12 (37.44) | |
| Heart disease | 4 (12.48) | |
| Lung disease | 3 (9.36) | |
| Diabetes | 2 (6.24) | |
| Liver diseases | 2 (6.24) | |
| Kidney disease | 1 (3.12) | |
| Sepsis | 6 (18.72) | |
| Surgeries done in patients prior to death | Total number of post-operative patients who died | 21 (65.52) |
| Emergency surgery | 20 (62.5) | |
| Elective surgery | 1 (3.12) | |
| LSCS | 10 (31.25) | |
| Caeserean hysterectomy | 4 (12.48) | |
| Examination under anaesthesia and proceed | 1 (3.12) | |
| Exploratory laparotomy | 4 (12.48) | |
| Laparotomy for ectopic pregnancy | 2 (6.24) | |
Multivariate cox regression analysis of mortality revealed statistically significant (P<0.05) increased risk of death in patients with heart disease (Hazard ratio [HR)=8.26, 95 per cent Confidence Interval (CI)=0.01-67.17, P<0.05), who required IMV (HR=35.5, CI= 3.14-401.75, P<0.05) or IS (HR=12.06, CI=1.96-74.19, P<0.05) and those admitted after IUFD (HR=5.17, CI=1-26.75, P<0.05) or admitted after undergoing laparotomy for EP (HR=50.2, CI=1.43-1766.87, P<0.05). The analysis also revealed a decreased risk of death for those admitted after VD (HR=0.1, CI=0.01-0.73, P<0.05; Table VI). Time survival plot shows that more than 3/4th of maternal mortalities happened within first 72 h of admission (Figure).
| Hazard ratio | P value | 95% confidence Interval | |
|---|---|---|---|
| Maternal age | 0.96 | 0.065 | 0.89-1.03 |
| Rural residence vs urban residence | 2.02 | 0.49 | 0.7-0.79 |
| Intra-uterine foetal death* | 5.17 | 0.049 | 1-26.75 |
| Twin pregnancy | 4.2 | 0.351 | 0.2-86.29 |
| Anaemia | 1.28 | 0.820 | 0.22-6.59 |
| Diabetes | 4.4 | 0.206 | 0.44-43.84 |
| Hypertension | 1.06 | 0.942 | 0.23-4.73 |
| Eclampsia | 0.38 | 0.229 | 0.07-1.83 |
| Abruption | 0.39 | 0.287 | 0.03-2.62 |
| Placenta praevia | 1.23 | 0.897 | 0.05-29.34 |
| Heart disease* | 8.26 | 0.048 | 0.01-67.17 |
| Kidney disease | 0.93 | 0.967 | 0.02-39.56 |
| Lung disease | 0.28 | 0.196 | 0.04-1.92 |
| Liver disease | 0.19 | 0.228 | 0.01-2.85 |
| Post partum haemorrhage | 4.28 | 0.203 | 0.45-40.22 |
| Sepsis | 1.21 | 0.842 | 0.18-8.18 |
| Surgery | 8.52 | 0.139 | 0.49-145.79 |
| Vaginal delivery* | 0.1 | 0.022 | 0.01-0.73 |
| Hysterotomy | 0.17 | 0.21 | 0.01-2.68 |
| Caesarian section | 1.5 | 0.651 | 0.25-8.7 |
| Caesarian hysterectomy | 1.09 | 0.961 | 0.03-30.95 |
| Examination under anaesthesia and proceed | 4.05 | 0.488 | 0.07-211.99 |
| Exploratory laparotomy | 0.97 | 0.981 | 0.06-14.98 |
| Laparotomy for ectopic pregnancy* | 50.2 | 0.031 | 1.43-1766.87 |
| Invasive mechanical ventilation* | 35.5 | 0.003 | 3.14-401.75 |
| Supplemental oxygen support | 0.27 | 0.076 | 0.06-1.15 |
| Inotropic support* | 12.06 | 0.007 | 1.96-74.19 |
| Blood transfusion | 2.07 | 0.375 | 0.41-10.37 |
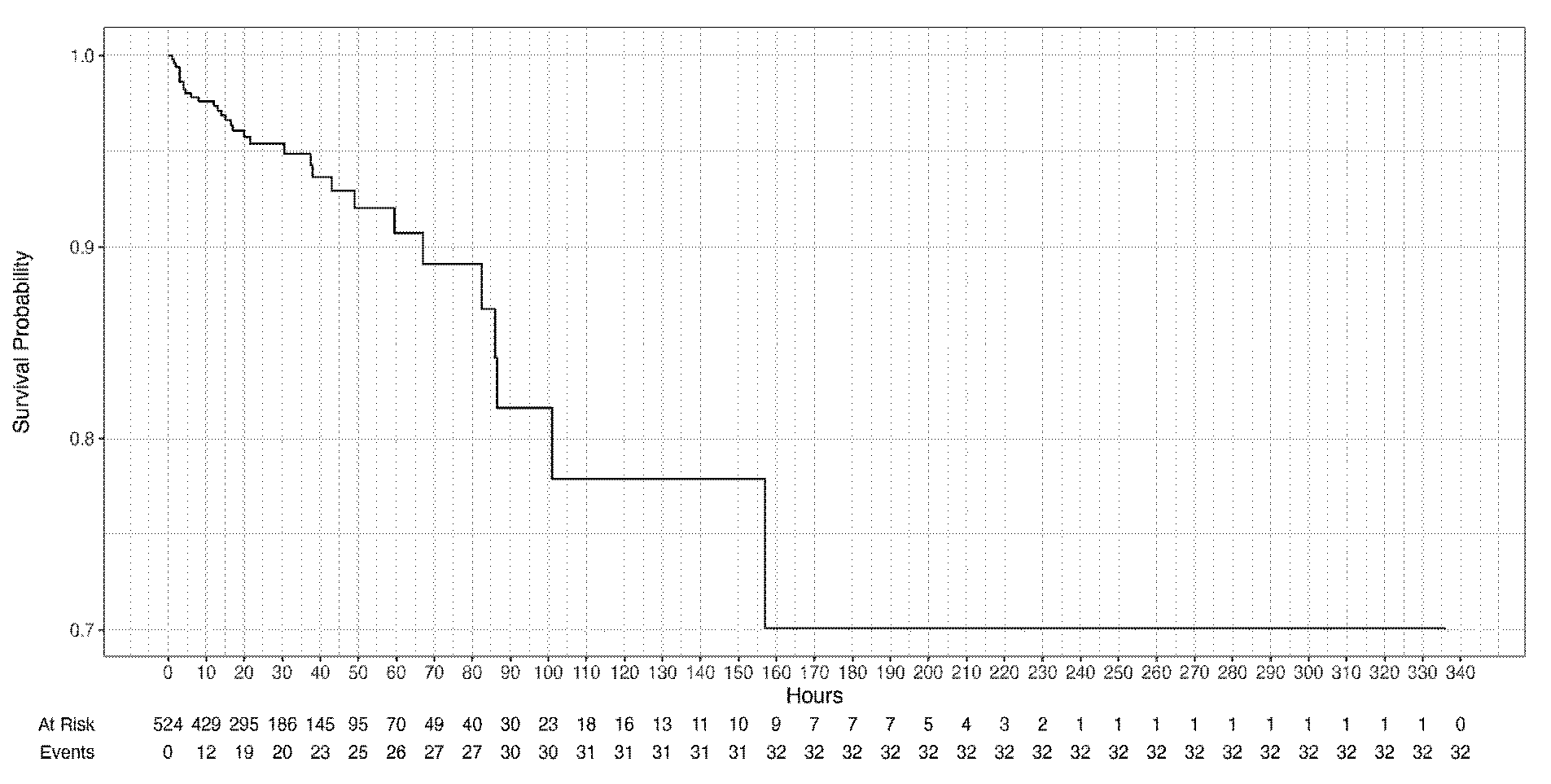
- Time survival plot of obstetric patients admitted to intensive care unit (N = 525).
Discussion
Ideally, obstetric patients should be managed in a multi-specialty centre with obstetric, neonatal and other non-obstetric facilities26,27. However, this may not always be possible, even in developed world21-24,26,27. OBG departments may work as stand-alone units or maternity hospitals like our centre. However, the lack of non-obstetric specialities at these centres may make patient care challenging21-24,26,27.
Most of the studies conducted on obstetric patients admitted to ICU are single-centre8-20 retrospective studies8-14,20. Only a few are prospective15-19, multi-center20, population based21-23 or with a case-control design13,14. Increased severity of illness on admission to ICU, as well as mortality, has been seen in un-booked obstetric patients as well as patients who did not receive antenatal care10,17. Patients with HDP (including pre-eclampsia, pregnancy-associated hypertension, and eclampsia) and its complications, along with other causes of OH, formed the bulk of our patients. These causes are similar in all regions of the world and have remained largely unchanged over time8-23. Multiple pregnancies (7% of our cohort) have also been seen to be associated with a higher risk for ICU admission12.
Like previous studies in developing countries, hypertension (including both essential hypertension and HDP), anaemia, and diabetes were the most common co-morbidities in our patients8-23,28,29. Anaemia is the most common nutritional disorder in pregnant females globally and is associated with poor maternal and foetal outcomes, including a higher risk of ICU admissions29. Management of patients with a high prevalence of anaemia and haemorrhage consequently requires a robust blood transfusion facility; more than half of our ICU patients required such services.
VD has been seen to have a lower risk of general anaesthesia, wound infection, maternal near miss, and placenta praevia and placenta accreta in subsequent pregnancies30-32. In our study, VD decreased mortality in patients admitted to ICU.
Although emergency CS has been shown to increase the risk for ICU admissions13,16,30, this demarcation between emergency and elective surgeries may not always be clear in obstetric care. The occurrence of hysterectomy at the time of CS (11% in our cohort) has been reported to increase the risk of ICU admissions16.
Unlike the developed world, where ruptured EP is an important cause of maternal mortality, EP does not form a major proportion of maternal mortality in India due to a higher number of other preventable causes like HDP, PPH, anaemia, and sepsis33-35. The incidence of EP is expected to increase globally due to an increase in CS deliveries and assisted reproductive technologies33. Patients with EP needing surgery after rupture and haemo-peritoneum have higher mortality35. Our study showed an increased risk of ICU mortality in these patients. This finding, though unique to our study, is not surprising given the delayed diagnosis, late presentations, and referrals of such patients at our centre. Since EP is a great mimicker, a high degree of suspicion and early intervention may save lives as well as future fertility in such patients33-35.
IUFD is associated with acute maternal complications, like clinical chorioamnionitis, PPH, and retained placenta36-38 as well as an increased risk of diabetes mellitus, renal disease, cardiovascular, and cerebrovascular diseases in the long term36. Although India contributes the highest number of stillbirths in the world, the data on these patients are inadequate37. Patients admitted after IUFD to the ICU had a statistically significant risk of death in our ICU.
The proportion of non-obstetric medical causes of maternal mortality and maternal near-miss, like heart diseases, has increased in recent times, especially in developed countries8-23,39,40. In our study, patients with heart diseases had a statistically significant increased risk of death when admitted to ICU.
The requirement of IMV and IS was seen in patients with high severity scores and haemodynamic instability. This is reflected in the higher mortality risk of these patients in previous studies14 as well as ours. The bulk of maternal mortality in our cohort occurred in the initial 72 h of the ICU admission. Therefore, timely transfers, prompt referrals, and early guided clinical decisions are essential in these patients. Our study also favours the technical feasibility of managing critically ill obstetric patients in stand-alone maternity centres like ours given very low transfer rates of our patients.
Our study had several strengths. First, our centre with high patient turnover manages booked as well as un-booked patients. This reflects in the large number of patients enrolled in the study in only one year period. Second, very low transfer-out rate at our centre leaves less scope for follow up losses. The patients admitted to our ICU in this study are, therefore, more representative of our centre as well as the general population of the area.
Our study also had some limitations. First, it was a single-centre study. Second, we analysed data from only one year. The protocols for admission to ICU may vary from centre to centre as well as from time to time, even in the same centre. Third, our centre caters to a very heterogeneous area with both urban as well as far-off rural areas. A significant variation in the clinical profile of these patients is therefore expected. We did not do this segregation in our ultimate analysis. Finally, ours is a dedicated centre for patients of OBG. This may lead to a referral bias to our centre with an under-representation of non-OBG medical or surgical causes of ICU admission in our cohort.
Overall, the data on the demography, clinical characteristics, and mortality in obstetric patients admitted to ICU is scarce and heterogeneous. However, the causes of ICU admission in these patients are uniform across the globe and have not changed over time. HDP and OH continue to be the most important causes of ICU admission in these patients. Mortality in obstetric ICU patients remains low. However, those admitted with heart diseases and who require IMV or IS are at increased risk of death in ICU. Similarly, those admitted after IUFD or after laparotomy for EP, are also at increased risk of mortality. On the other hand, patients admitted after VD, have a statistically significant reduced risk of mortality in ICU. ICUs at maternity hospitals can be run with satisfactory outcomes by in-house obstetricians, intensivists, anaesthetists, and neonatologists with the support of other specialties whenever needed.
Financial support & sponsorship
None.
Conflicts of Interest
None.
Use of Artificial Intelligence (AI)-Assisted Technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing of the manuscript and no images were manipulated using AI.
References
- Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27:89-94.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Pregnancy complications and later life women’s health. Acta Obstet Gynecol Scand. 2023;102:523-31.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Global causes of maternal death: A WHO systematic analysis. Lancet Glob Health. 2014;2:e323-3.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal near miss – towards a standard tool for monitoring quality of maternal health care. Best Pract Res Clin Obstet Gynaecol. 2009;23:287-96.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of maternal chronic diseases during pregnancy - a nationwide population based study from 1989 to 2013. Acta Obstet Gynecol Scand. 2016;95:1295-304.
- [CrossRef] [PubMed] [Google Scholar]
- Associations between comorbidities and severe maternal morbidity. Obstet Gynecol. 2020;136:892-901.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Transforming our world: the 2030 agenda for sustainable development. Available from: https://sdgs.un.org/2030agenda, accessed on July 6, 2024.
- Analysis of clinical characteristics, rationale, and management of critically ill obstetric patients transferred to ICU. J Pak Med Assoc. 2015;65:959-62.
- [PubMed] [Google Scholar]
- Study of obstetric admissions to the intensive care unit of a tertiary care hospital. J Obstet Gynaecol India. 2016;66:12-7.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Pattern and outcome of obstetric admissions into the intensive care unit of a southeast Nigerian hospital. Indian J Crit Care Med. 2018;22:16-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Pregnancy related and postpartum admissions to intensive care unit in the obstetric tertiary care center - an 8-year retrospective study. Ginekol Pol. 2021;92:575-8.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal critical care in obstetrics. J Obstet Gynaecol Can. 2009;31:218-21.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors for obstetric admissions to the intensive care unit in a tertiary hospital: A case-control study. Arch Gynecol Obstet. 2005;272:207-10.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of maternal mortality among critically ill obstetric patients. Malawi Med J. 2015;27:16-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Epidemiologic profile, survival, and maternal prognosis factors among women at an obstetric intensive care unit. Int J Gynaecol Obstet. 2014;124:63-6.
- [CrossRef] [PubMed] [Google Scholar]
- Severe maternal morbidity in a general intensive care unit in Nigeria: Clinical profiles and outcomes. Int J Obstet Anesth. 2016;28:39-44.
- [CrossRef] [PubMed] [Google Scholar]
- Critically ill obstetric admissions to an intensive care unit: A prospective analysis from a tertiary care university hospital in south India. Indian J Crit Care Med. 2019;23:78-82.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Determinants of maternal mortality in a critical care unit: A prospective analysis. Lung India. 2022;39:44-50.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Predictors and outcome of obstetric admissions to intensive care unit: A comparative study. Indian J Public Health. 2016;60:159-63.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors of obstetric admissions to the intensive care unit: An 8-year retrospective study. Medicine (Baltimore). 2019;98:e14835.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Obstetric admissions to intensive care units in Australia and New Zealand: A registry‐based cohort study. BJOG. 2020;127:1558-67.
- [CrossRef] [PubMed] [Google Scholar]
- Variability in intensive care unit admission among pregnant and postpartum women in Canada: a nationwide population-based observational study. Crit Care. 2019;23:381.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Obstetric admission to intensive care units in Japan: A cohort study using the Japanese intensive care patient database. J Anesth. 2023;37:539-45.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- What is an intensive care unit? A report of the task force of the world federation of societies of intensive and critical care medicine. J Crit Care. 2017;37:270-6.
- [CrossRef] [PubMed] [Google Scholar]
- RStudio: Integrated Development for R, 2024. Available from: http://www.rstudio.com/, accessed July 20, 2024.
- Multidisciplinary obstetric critical care delivery: The concept of the “virtual” intensive care unit. Semin Perinatol. 2018;42:3-8.
- [CrossRef] [PubMed] [Google Scholar]
- Current perspectives on maternity critical care. Anaesthesia. 2023;78:758-69.
- [CrossRef] [PubMed] [Google Scholar]
- Hypertension in women and pregnancy. Crit Care Nurs Q. 2023;46:377-90.
- [CrossRef] [PubMed] [Google Scholar]
- Severity of anemia during pregnancy and adverse maternal and fetal outcomes. JAMA Netw Open. 2022;5:e2147046.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Planned cesarean delivery vs planned vaginal delivery: A systematic review and meta-analysis of randomized controlled trials. Am J Obstet Gynecol MFM. 2023;5:101186.
- [CrossRef] [PubMed] [Google Scholar]
- Mode of delivery and pregnancy outcomes in preterm birth: a secondary analysis of the WHO global and multi-country surveys. Sci Rep. 2019;9:15556.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Long-term risks and benefits associated with cesarean delivery for mother, baby, and subsequent pregnancies: Systematic review and meta-analysis. PLoS Med. 2018;15:e1002494.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Overview of ectopic pregnancy diagnosis, management, and innovation. Womens Health (Lond). 2023;19:17455057231160349.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Pregnancy-related deaths due to hemorrhage: Pregnancy mortality surveillance system, 2012-2019. Obstet Gynecol. 2024;144:252-5.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Clinical profile, risk factors and outcomes of ectopic pregnancy in a tertiary care hospital: A prospective Indian study. Cureus. 2023;15:e49483.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Maternal complications associated with stillbirth delivery: A cross-sectional analysis. J Obstet Gynaecol. 2016;36:208-12.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Stillbirths in India: Current status, challenges, and the way forward. Indian J Pediatr. 2023;90:63-70.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Fetal loss and long-term maternal morbidity and mortality: A systematic review and meta-analysis. PLoS Med. 2024;21:e1004342.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- The impact of cardiovascular diseases on maternal deaths in the nordic countries. Acta Obstet Gynecol Scand. 2021;100:1273-9.
- [CrossRef] [PubMed] [Google Scholar]
- Heart disease complicating pregnancy as a leading cause of maternal deaths in LMIC settings: The Sri Lankan experience. Lancet Reg Health Southeast Asia. 2023;15:100223.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




