Translate this page into:
Lymph nodes cytology in HIV seropositive cases with haematological alterations
Reprint requests: Dr T. Neelima, C/O Ch. Venkata Rao, Door no: 5-54-80, 6/18 Brodipet, Guntar 522 002, Andhra Pradesh, India e-mail: nilu_medico@yahoo.co.in
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Lymphadenopathy and haematological alterations are the earliest manifestations with other associated opportunistic infections and malignancies. Hence, there is a need for simple investigations like fine needle aspiration cytology (FNAC) for evaluation of HIV lymphadenopathy and a haemogram to interpret the haematological alterations. This study was undertaken to analyze the cytological patterns of lymph node lesions in HIV/AIDS patients, to compare with available clinico-pathological and haematological parameters to segregate lymphadenopathy cases for further evaluation.
Methods:
In the present study, 129 HIV seropositive patients were included. Lymph node aspirates were stained routinely with hematoxylin and eosin and Ziehl-Neelsen (Z-N) stains. Special stains and cultures were done in selected patients. Peripheral smears were taken from all the patients and CD4 counts were recorded. Tuberculous lymphadenitis was further categorized. Acid fast bacilli (AFB) grading was done on Z-N positive smears. Each lesion was compared with CD4 counts, WHO clinical staging and haematological picture.
Results:
Cytological diagnosis in 129 patients included tuberculous (n=54, 41.9%), reactive lymphadenopathy (n=46, 35.6%), suppurative (n=16, 12.4%) lymphadenitis, non-Hodgkin's lymphoma (n=4, 3.1%), and Hodgkin's lymphoma, secondary deposits, other granulomatous lesions, and cryptoccocal lymphadenitis in one patient each. The predominant cytomorphological pattern in tuberculous lymphadenitis was caseous necrosis + epithelioid granuloma formation (51.85%). Grade 2+ Z-N grading was noted in 62.96 per cent of AFB positive smears. CD4 counts showed a descending pattern with progression of WHO clinical staging. Cytopenia was more common in WHO clinical stage IV disease.
Interpretation & conclusions:
Lymph node cytology was found to be a useful tool for segregating lymphadenopathy cases for further evaluation and for identification of opportunistic infections, neoplastic and non-neoplastic lesions. Comparison of lymph node lesions with CD4 counts, WHO clinical staging, haematological alterations and AFB grading reflects immunity, stage of disease and disease activity aiding better treatment.
Keywords
AFB
CD4 count
FNAC
HIV
lymphadenopathy
lymph node aspirates

According to UNAIDS report on the global AIDS epidemic (2012) 34 million people are living with HIV1. There are 2.39 million people living with HIV/AIDS in India2. Coverage of anti retroviral therapy (ART) at the end of 2009 in India was 21-40 per cent3. ART is used to reduce the replication and plasma viral load of HIV virus to undetectable levels.
Lymphadenopathy is a common manifestation of many diseases which are categories as “MIAMI” representing malignancies, infections, autoimmune disorders, miscellaneous and iatrogenic causes. Among various serious illnesses that can present with lymphadenopathy as an early presentation, one of the most concerning causes is HIV infection and its associated lesions456.
In developing countries like India, with a huge population and socio-economic constraints, there is a need for a simple investigative technique like fine needle aspiration cytology (FNAC) to investigate lymphadenopathy7. The aspirated material can be used for further ancillary studies8.
This study was undertaken to observe the cytomorphology of lymph node aspirates of HIV seropositive patients along, with various clinical and haematological parameters to improve the diagnostic efficacy.
Material & Methods
The study was conducted in the Department of Pathology, NRI Medical College and General Hospital, Chinakakani, Andhra Pradesh, India, from May 2009 to April 2011. One hundred and twenty nine HIV seropositive patients with lymphadenopathy were included. Fourteen patients with lymphadenopathy of <0.5 cm in diameter and known haematological disorders were excluded from the study.
One hundred and fifty three lymph node aspirates from 129 cases (34 cases had lymph nodes at multiple sites) using 23G needle and 5 ml disposable syringe were obtained. Smears were alcohol-fixed. Hematoxylin & eosin (H&E) and Ziehl-Neelsen (Z-N) staining were done in all cases. Acid fast bacilli (AFB) grading was done on Z-N stain positive smears.
Grading of AFB was done as proposed by Kumar et al9. Grade 1+ = AFB was found after a careful search; Grade 2+ = AFB were singly scattered; Grade 3+ = AFB were found in large numbers arranged in faggots and singly. Bacilli could be detected even under 10X magnification.
Other special stains like Gram's stain, perioidic acid schiff stain (PAS), Grocott methanamine silver stain (GMS) and mucicarmine were used to rule out any other offending pathogen. Culture and sensitivity were performed from the lymph node aspirates whenever necessary. Histological study was done only in one case. Laboratory details (including complete haemogram, CD4 count) were compared with lymph node cytomorphology and revised WHO clinical staging system for adults and adolescents10.
The study protocol was approved by the institutional ethics committee.
Results
The age group of patients ranged from 13-65 yr with a mean age of 32.4 ± 10.9 SD yr. The male: female ratio was 1.3:1; 98 (76%) patients were between 21-40 yr.
The most common symptom was fever in 109 patients (84.49%). Pallor was the most common sign in 79 patients (61.24%). The increased occurrence of signs (pallor, oral thrush) and symptoms (fever, fatigue, weight loss) possibly was due to severity of the illness as majority of the patients (60) were in WHO clinical stage IV.
The most common site of lymphadenopathy was cervical (left posterior cervical group) in 124 patients (81.04%), followed by axillary lymphadenopathy in 19 (12.4%). The size of the lymph nodes ranged between 0.5 to 6 cm. Majority (80.62%) were of <2 cm size. Of the lymph nodes of size <2 cm, 41.34 per cent were diagnosed as reactive lymphadenitis. Lymph nodes with larger sizes (>2-6 cm) included five cases of lymphomas with a mean size of 4.5 cm, one case of metastatic deposits of 5 cm size and the remaining were cases of suppurative lymphadenitis and cold abscesses with a mean size of 3.2 and 3.6 cm, respectively, indicating that increased lymph nodel size was associated with clinically significant and malignant lesions.
The distribution of cytological diagnosis of various HIV lymphadenopathies included tuberculous lymphadenitis in 54 cases (41.8%), which was the most common cytological diagnosis. The three cytological patterns of tuberculous lymphadenitis diagnosed were caseous necrosis- epithelioid cell granulomas (CN-ECG) in 28 (51.85%) of patients, caseous necrosis (CN) in 20 (37.04%) patients and epithelioid cell granulomas (ECG) in 6 (11.11%) patients (Fig. 1).

- Various cytological patterns of tuberculous lymphadenitis on FNAC. 1a. Caseous necrosis (CN) (H&E 40X). 1b. Epithelioid cell granuloma (ECG) (H&E 400X). 1c. Epithelioid cell granuloma in a caseous necrotic background (CN-ECG) (H&E 100X). 1d. Langhans type of giant cell in tuberculous lymphadenitis (H&E 1000X).
Cytological features were associated with AFB grading on Z-N stain positive smears. Acid fast bacilli (AFB) were abundant in smears with caseous necrosis and decreased in cases with granulomas. This difference in staining pattern was assumed to be due to compromised immunity in HIV infected individuals. The present study showed grade 2+ as the predominant pattern (62.96%). Z-N grade 1+ was seen in 6 (11.11%) and grade 3+ in 14 (25.92%) patients. CD4 counts in tuberculous lymphadenitis patients were found to be decreased with increased bacillary load. Mean CD4 counts in patients with CN were 99.6-103.7, 105.2 in CN-ECG and 139.5 cells/μl in ECG (Fig. 2).
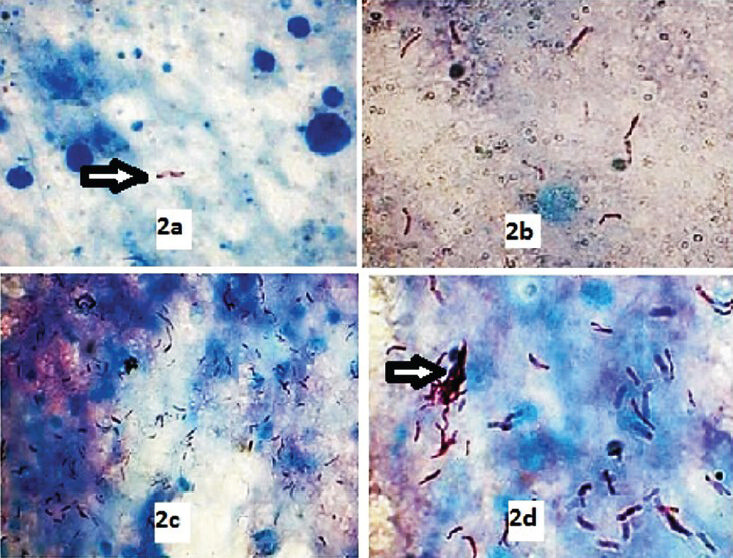
- AFB grading on Z-N stained smears. 2a. Grade 1 + (ZN stain 1000X). 2b. Grade 2+ (ZN stain 1000X). 2c. Grade 3+ (ZN stain 400X). 2d. Grade 3+ (ZN stain 1000X).
Reactive lymphadenitis was seen in 46 patients (35.6%). This was the second common cytological diagnosis with a mean CD4 count of 283.3 cells/μl. Non-specific chronic granulomatous lymphadenitis was seen in only one patient. The routine culture of this lymph node aspirate was sterile and no fungus was demonstrated on special stains.
Sixteen cases (12.4%) of suppurative lymphadenitis were diagnosed. Gram's stain, PAS and GMS staining was done on these smears. Smears were negative for PAS and GMS stains but nine patients showed either Gram negative/positive bacilli in the lymph node aspirates indicating secondary bacterial infections. Mean CD4 count in this group of patients was 181.65 cells/μl.
One patient was diagnosed with cryptococcal lymphadenitis. Cryptococcus was confirmed by PAS, GMS and mucicarmine stains. When compared to other lesions, CD4 counts in cryptococcal lymphadenitis showed lowest value of 48 cells/μl and the patient was in WHO clinical stage IV (Fig. 3). Of the five cases of lymphomas, four were reported as non-Hodgkin's lymphoma (NHL) and one was a Hodgkin's lymphoma. One case of papillary adenocarcinomatous deposits from lung was observed. All these malignant lesions had a CD4 count <100 cells/μl (Fig. 4).
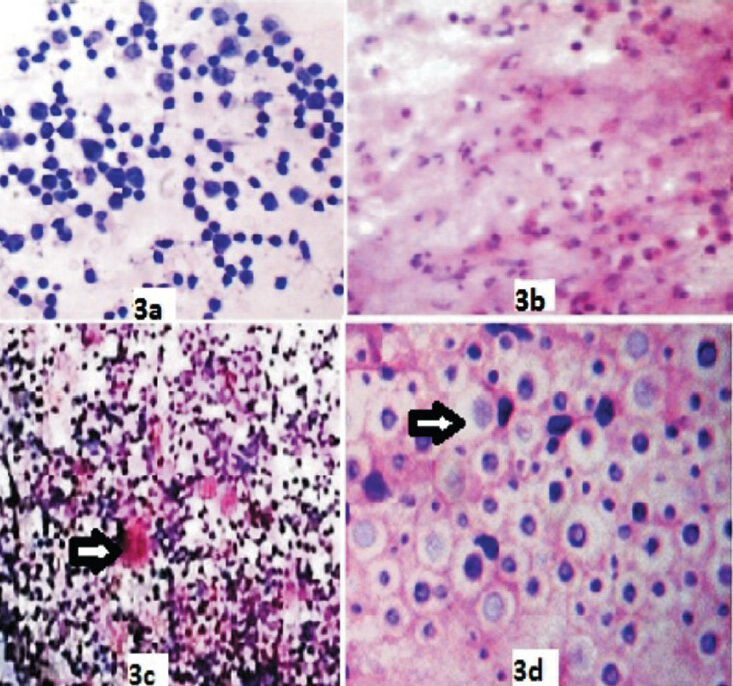
- Various non neoplastic cytological patterns of HIV lymphadenopathy on FNAC. 3a. Reactive lymphadenitis showing polymorphous lymphoid population (H&E 400X). 3b. Suppurative lymphadenitis with degenerating neutrophils (H&E 400X). 3c. Non specific granulomatous lesion (H&E 100X) 3d. Cryptococci showing capsule (H&E 1000X).
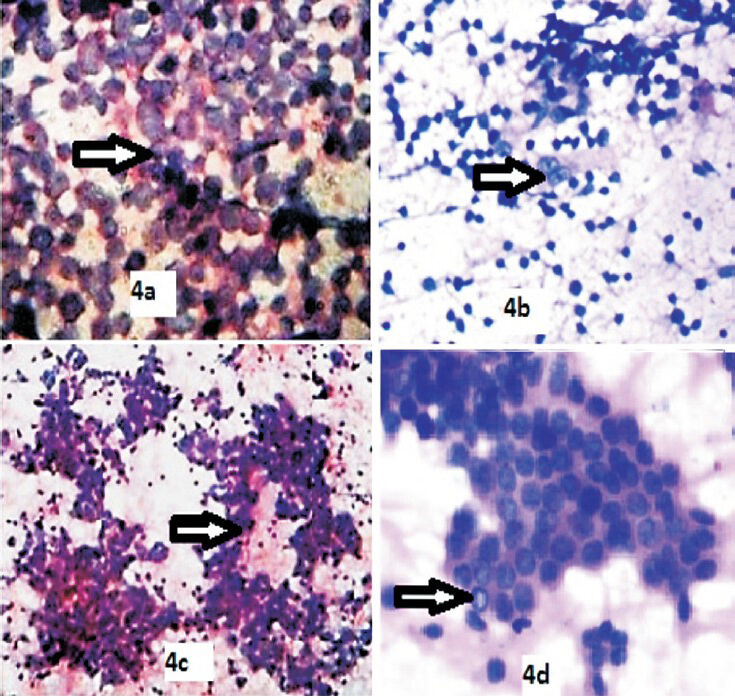
- Various neoplastic cytological patterns of HIV lymphadenopathy on FNAC. 4a. Non Hodgkin's lymphoma showing monotonous population of lymphoid cells (H&E 400X). 4b. Hodgkin's lymphoma showing Reed Sternberg cell (H&E 100X). 4c. Papillary adenocarcinomatous deposits showing papillae with fibrovascular cores (H&E 100X). 4d. Papillary adenocarcinomatous deposits showing papillae with intranuclear inclusions (H&E 400X).
Of the 129 patients, lymph node aspirates from five (3.9%) patients were inadequate to report. Repeated aspirations in these cases yielded only blood and blood cellular elements.
Among the haematological alterations, anaemia was the most common presentation in 79 patients (61.24%). Most common type among females was microcytic hypochromic anaemia (n=28, 58.22%) with WHO clinical stage IV disease and a cytological diagnosis of cold abscess. Normocytic normochromic anaemia was reported in 45patients (34.9%). Most of them had a cytological diagnosis of reactive lymphadenopathy due to a better immune status, anti retroviral therapy and high CD4 counts. Macrocytic anaemia was seen in a case of NHL with increased cell turn over utilizing B12 and folic acid stores. Biochemical analysis in this patient showed decreased B12 and folic acid levels. Of the 79 patients presenting with anaemia, 66 patients (83.54%) with Hb% <11 g% had CD4 count <200cells/μl and the remaining 13 patients (16.46%) had CD4 counts >200 cells/μl reflecting variable immune status and varied clinical staging.
The total leukocyte counts ranged from 1900 to16300 cells/μl. Relative neutrophilia was noted in 32 (24.8%) patients, neutrophilic leucocytosis in 28 (21.7%) with toxic granulations in 19 patients (14.7%). Neutrophilic alterations were seen in reactive and suppurative lymphadenitis. Lymphocytic preponderance was seen mostly in tuberculous lymphadenitis constituting 23 patients (17.82%), lymphocytosis in four (3.10%) and five patients (3.87%) showed reactive lymphocytes. Peripheral eosinophilia was seen in three cases with skin and oral infections but no fungal elements were isolated from the lymph node aspirate (Fig. 5).
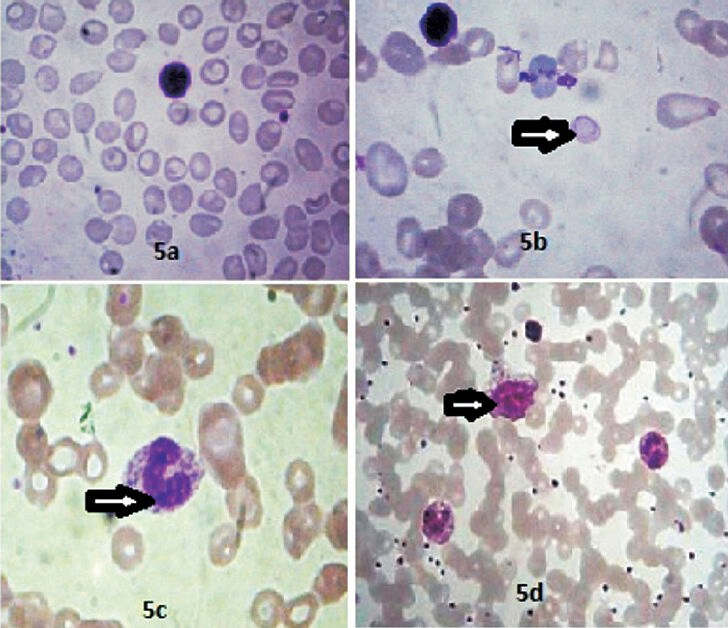
- Haematological alterations in HIV seropositive patients?. 5a. Microcytic hypochromic anaemia (Leishman stain 400X). 5b. Macrocytic anaemia showing cabot ring (Leishman stain, 1000X). 5c. Neutrophil with toxic granules (Leishman stain, 1000X). 5d. Showing a reactive lymphocyte (Leishman stain, 400X).
Leucopenia (in 4.65% patients) and thrombocytopenia (in 3.10% patients) were seen in cases with NHL undergoing chemotherapy and in a case with secondary deposits. Reactive thrombocytosis was seen in 3(2.4%) patients and 9 (7%) patients had a normal blood picture.
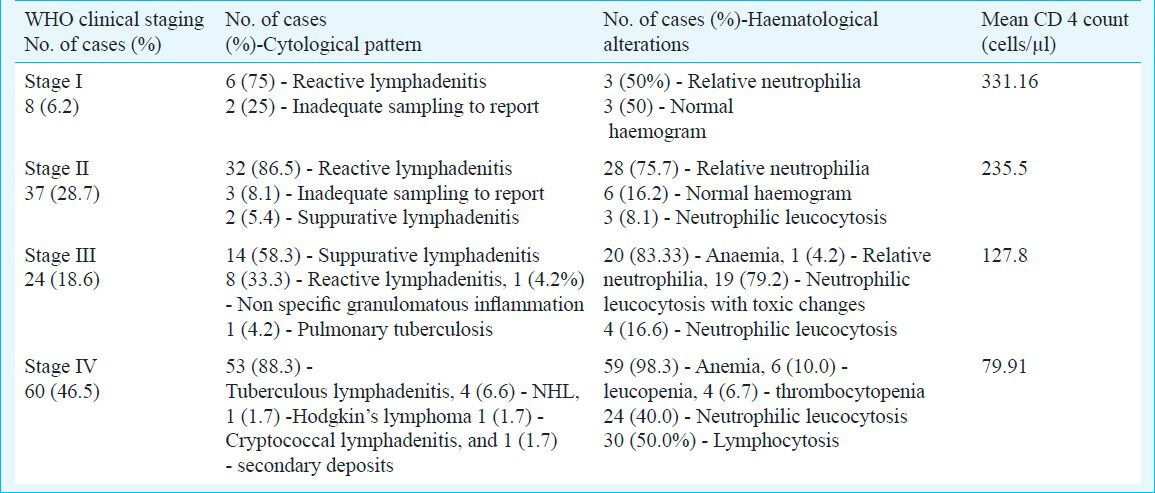
The WHO clinical staging was done in all cases. It included eight (6.2%) patients in WHO clinical stage I, 37 (28.68%) in stage II, 24 (18.6%) in stage III and 60 (46.51%) in stage IV disease. The WHO clinical staging of HIV seropositive patients was associated with cytological diagnosis and haematological alterations. CD4 counts showed a descending pattern with progression of WHO clinical staging (Table).
Discussion
Lymphoid tissues are one of the prime targets in HIV/AIDS11. Regardless of the portal of entry of HIV, these are the major anatomic sites for establishment and propagation of HIV infection12. The commonest opportunistic infection among HIV seropositive cases is tuberculosis13. Extrapulmonary involvement occurs frequently and earlier than the other opportunistic infections, especially in individuals dually infected with HIV and tuberculous bacilli14. Occurrence of extrapulmonary tuberculosis has increased by 20 per cent as compared to 3 per cent increase in cases of pulmonary tuberculosis and is believed to be due to more severe immunodeficiency in the HIV-infected patient15.
In the present study, maximum number of cases i.e. 98 patients (76%) were seen in the age group of 21-40 yr. Similar findings have been reported earlier161718.
In the present study, males (57.3%) were affected more commonly then females (42.6%) with a male: female ratio of 1.34:1. Similar findings were reported by Deshmukh et al19 (1.7:1) and Guru et al20 (2.3:1). In contrast, female predominance was noted by Narang et al21 (4:5). The incidence of lymphadenopathy decreased with advancing age after 50 years as in a study by Agravat et al17.
The most common site of lymphadenopathy was cervical in 124 patients (81.04%). Similar findings were recorded by others171920.
The most common cytological diagnosis was tuberculous lymphadenitis(41.8%); similar to observations made in studies by others1117181922. The diagnosis of tuberculous lymphadenitis was rendered only when smears were positive for AFB. A similar criterion is considered by others1923.
CN was the predominant cytological pattern in the present study among tuberculous lymphadenitis. Gupta et al7 had made similar observations. Other groups have recorded CN -ECG as predominant pattern of tuberculous lymphadenitis1124.
Association of grading of AFB staining pattern with cytomorphological features of tuberculous lymphadenitis demonstrated the presence of AFB in greater number in smears showing CN pattern and their number decreased with appearance of granulomas. Similar observations have been made by others72024. Mean CD4 T lymphocyte count decreased progressively with increase in AFB load and appearance of necrosis. Three cases were found to be multi drug resistant tuberculosis by culture and sensitivity.
In the present study, highest CD4 counts were observed in patients with reactive lymphadenitis. Similar observations have been reported by others1720.
Diagnosis of non-specific chronic granulomatous lymphadenitis was considered when granulomas were observed in the absence of AFB in the smears studied. Jayaram and Chew22 and Kumar Guru et al20 considered a similar criterion. This lesion needs further evaluation such as biopsy and serological investigations to establish the aetiological agent.
In the present study, cryptococci were seen in sheets in the lymph node aspirate of a seriously immuno compromised HIV seropositive patient. Saikia et al23 observed two cases and Jayaram and Chew22 observed one case of cryptococcal lymphadenitis in their studies. One patient with metastatic disease was also observed viz. papillary lung carcinoma metastatic to a lymph node. Squamous cell carcinoma deposits and poorly differentiated carcinoma deposits have been seen and reported in earlier studies1123.
Haematological complications are a common cause of mortality in HIV infected patients. Cytopenias are most frequent during the advanced stages of the disease. Of all the cytopenias, anaemia was most common in the present study as reported earlier also25. HIV infected individuals with anaemia are at increased risk for progression to AIDS and its associated high mortality. The multifactorial origin of anaemia in HIV disease complicates its differential diagnosis and treatment. In the present study, increased prevalence of microcytic hypochromic anaemia in females was due to periodic blood loss during regular menstrual cycles, parity, along with irregular iron metabolism and reutilization due to chronic HIV infection26.
The present study demonstrated the utility of lymph node cytology in the diagnosis and segregation of HIV lymphadenopathies with various haematological alterations, CD4 counts and WHO clinical staging. FNAC of HIV lymphadenopathy is a valuable tool for identification of opportunistic infections, neoplastic and non-neoplastic lesions and also for segregating cases that need further evaluation. Non specific chronic granulomatous lymphadenitis needs biopsy for aetiological work up. Neoplastic lesions like NHLs need biopsy and immunohistochemistry for further typing. Correlation of cytological lesions with CD4 counts, haematological parameters and WHO clinical staging provides information about immune status and stage of the disease.
References
- Global AIDS Response Progress Reporting 2012: guidelines - construction of core indicators for monitoring the 2011 political declaration on HIV/AIDS. Geneva: UNAIDS; 2012.
- [Google Scholar]
- HIV Sentinel Surveillance 2010-11: A Technical Brief. New Delhi: National AIDS Control Organization (Department of AIDS Control); 2012.
- [Google Scholar]
- Estimating the impact of antiretroviral therapy: regional and global estimates of life-years gained among adults. Sex Transm Infect. 2010;86(Suppl 2):ii67-ii71.
- [Google Scholar]
- Lymph node biopsies in HIV-infected and non- infected children with persistent lung disease. Int J Tuberc Lung Dis. 2000;4:139-46.
- [Google Scholar]
- Clinico-immunopathological alterations of lymphnodes from human immunodeficiency virus infected patients in northern Thailand. Asian Pac Allergy Immunol. 1999;17:85-92.
- [Google Scholar]
- Fever of undetermined origin in patients with the acquired immunodeficiency syndrome in Brazil: report on 55 cases. Reg Insti Medi Trop Sao Paulo. 1999;41:27-32.
- [Google Scholar]
- Reliability and limitations of fine needle aspiration cytology of lymphadenopathies: an analysis of 1,261 cases. Acta Cytol. 1991;35:777-83.
- [Google Scholar]
- Role of fine needle aspiration cytology in the diagnosis of lymphadenopathy. Indian J Chest Dis Allied Sci. 1993;35:27-9.
- [Google Scholar]
- Acid-fast staining patterns and their correlation with HIV positivity (lett) Acta Cytol. 2005;49:111-2.
- [Google Scholar]
- The Union WHO clinical staging of HIV infection and disease, tuberculosis and eligibility for antiretroviral treatment:relationship to CD4 lymphocyte counts. Int J Tuberc Lung Dis. 2005;9:258-62.
- [Google Scholar]
- Fine needle aspiration diagnosis in HIV-related lymphadenopathy in Mangalore, India. Acta Cytol. 2002;46:35-9.
- [Google Scholar]
- Human immunodeficiency virus disease: AIDS and related disorders. In: Kasper DC, Fauci AS, Longo DL, Braunwald E, Hauser SL, Jameson IT, eds. Harrison's principles of internal medicine (16th ed). New York: McGraw-Hill Companies; 2005. p. :1076-39.
- [Google Scholar]
- Diagnostic utility of fine needle aspiration (FNA) cytology in HIV-infected patients with lymphadenopathy. Cytopathology. 1998;9:230-9.
- [Google Scholar]
- The global tuberculosis situation and the new control strategy of the World Health Organization. Tubercle. 1991;72:1-6.
- [Google Scholar]
- Tuberculosis and acquired immunodeficiency syndrome: A historical perspective on recent developments. Am J Med. 1994;96:439-50.
- [Google Scholar]
- Dignostic utility of FNAC in HIV positive lymphadenopathy. J Clin Res Lett. 2012;3:37-40.
- [Google Scholar]
- Fine needle aspiration cytology study of lymphnode in HIV patients and CD4 count. Int J Res Med. 2013;2:16-9.
- [Google Scholar]
- Fine-needle aspiration cytology findings in human immunodeficiency virus lymphadenopathy. Indian J Pathol Microbiol. 2008;51:481-4.
- [Google Scholar]
- Cytological evaluation of lymphadenopathy in HIV patients. Int J Recent Trends Sci Technol. 2013;6:125-9.
- [Google Scholar]
- Fine needle aspiration cytology of lymph nodes in HIV- infected individuals. Acta Cytol. 2000;44:960-6.
- [Google Scholar]
- Fine needle aspiration cytology in lymphadenopathy of HIV positive cases. Acta Cytol. 2001;45:589-92.
- [Google Scholar]
- Tuberculous lymphadenitis: Correlation of cellular components and necrosis in lymph node aspirate with AFB positivity and bacillary count. Indian J Pathol Microbiol. 1990;33:1-10.
- [Google Scholar]
- Profile of hematological abnormalities of Indian HIV infected individuals. BMC Blood Disorders. 2009;9:1-6.
- [Google Scholar]
- Pathogenesis of anemia during human immunodeficiency virus infection. J Investig Med. 2001;49:225-39.
- [Google Scholar]




