Translate this page into:
Low vaccine efficacy of mumps component among MMR vaccine recipients in Chennai, India
Reprint requests: Dr. Thangam Menon, Director Professor & Head, Department of Microbiology, Dr. ALM Post Graduate Institute of Basic Medical Sciences, University of Madras, Taramani Campus, Chennai 600 113, India. e-mail: thangam56@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction of MMR vaccine was believed to have resulted in a decline in the incidence of measles, mumps and rubella infections. However, recent reports suggest the re-emergence of mumps infection worldwide in the vaccinated populations. It was proposed that the reason for this re-emergence was poor efficacy of MMR vaccine. The present study was aimed to investigate mumps infection in MMR vaccinated and non-vaccinated populations in Chennai, India. Blood samples were collected from acute mumps cases (n=74, 42<12 yr age, 54% males) and investigated for IgM antibody against mumps, IgG antibody against measles, mumps and rubella viruses by ELISA. Sixty seven (91%) patients had received MMR vaccine. All the 67 vaccinated cases were positive for parotitis, and mumps IgM. However, only 10 (15%) were positive for IgG. All samples (100%) were positive for rubella and measles IgG. These findings showed the occurrence of mumps infection among MMR vaccinated individuals in Chennai, India. The MMR vaccine failed to generate anti-mumps IgG. The reason may be low vaccine efficacy of the mumps component of the MMR vaccine used.
Keywords
ELISA
IgM and IgG antibody
mumps virus
MMR vaccine

Mumps is an acute, systemic, communicable viral infection characterized by swelling of one or both parotid glands, often accompanied by more serious complications, such as meningitis, pancreatitis, or orchitis1. After the implementation of the mumps vaccine in 1967 in the United States, by 2001, the disease was nearly eliminated, with less than 0.1 case per 100,0002. Similar success in the control of mumps has been achieved in other countries; however, over the past few years, mumps has made a global resurgence. Though mumps is considered as a childhood disease, the present outbreaks predominantly involve vaccinated young adults2. In addition to waning immunity, it has also been postulated that antigenic differences between the vaccine and strains causing outbreaks may result in a deficient immune response conferred by the vaccine234. There have been no comprehensive reports on the prevalence of mumps infection in India, and a majority of cases go unnoticed. There are a few reports which describe the seroprevalence of mumps in India567. The World Health Organization, the Advisory Committee on Immunization Practices as well as the Indian Academy of Pediatrics, have recommended the use of two doses of the MMR (measles, mumps, rubella) vaccine for immunization6. However, the protection it offers in developing countries including India, where mumps is still a major health problem is not known689. The epidemiology and magnitude of mumps in India is still not fully understood, and it is suggested that outbreaks occur at the intervals of 5 to 10 years7 and incidence of mumps infection occurs during January to March each year5. Previous studies have indicated that children are commonly affected with preponderance in males in addition to reports of meningoencephalitis and orchitis in vaccinated patients56710. An important fact that needs mention is that currently the MMR vaccine is not routinely administered to children in government healthcare centres5611. This study was planned to determine the occurrence of mumps infection in MMR vaccinated and unvaccinated populations attending the healthcare facilities in Chennai, Tamil Nadu, India.
For the selection of mumps cases, the WHO guidelines were adopted which include an acute onset of unilateral or bilateral tender, self-limited swelling of the parotid or other salivary glands, lasting two or more days and without other apparent cause12. An informed written consent was obtained prior to inclusion and the study was approved by the Ethics committee of Sri Ramachandra University, Chennai, India.
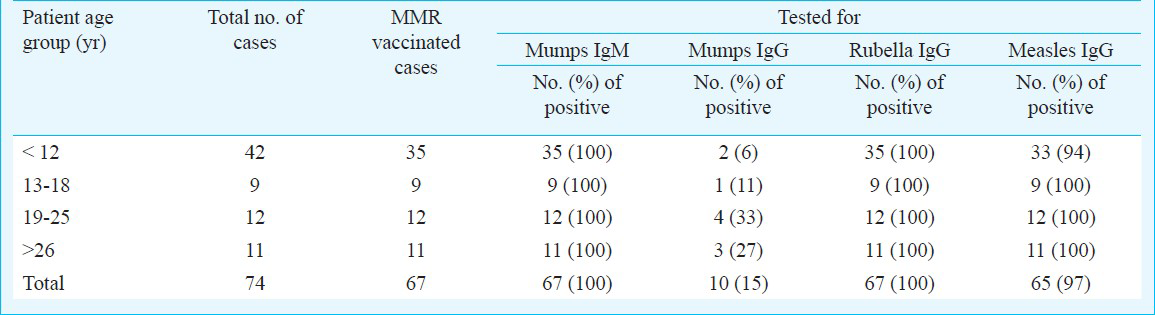
A total of 74 serum samples from suspected mumps cases were collected over a period of 16 months (July 2011 to November 2012) from Sri Ramachandra Medical College & Research Institute and V. K. Nursing Home, Chennai, India. Patients exhibited clinical manifestations which included parotitis (swelling in left cheek 15 (20%), swelling in right cheek 16 (22%) and bilateral swelling 43 (58%). Other complaints were high fever 74 (100%), vomiting 16 (22%), headache 17 (23%), orchitis 3 (4%), ear pain 5 (7%), difficulty in swallowing 9 (12%), rash 6 (22%), loss of appetite 5 (7%), conjunctivitis 4 (5%), lymph node enlargement 8 (11%) and abdominal pain 2 (3%). The occurrence of mumps infection was highest in school children 53 (72%), followed by a very low percentage in teachers, college students, housewives, cooks, clerks and housemaids. Of the 74 samples collected from various age groups, 42 were from paediatric patients (Table). Of these, 54 per cent were males. Sixty seven (91%) patients had received MMR vaccine while the others were not vaccinated. Systematic laboratory tests which included quantitative IgM and IgG antibody assays (Techno Genetics, Italy) were done for all the samples. Results for mumps IgM in vaccinated cases indicated that all samples (100%) tested were positive, whereas 57 of 67 (85%) samples were negative for mumps IgG. These facts inevitably state that MMR vaccine failed to offer protection in vaccinated individuals against mumps infection. All 67 (100%) samples tested positive for rubella specific IgG and 65 (97%) samples tested positive for measles specific IgG, suggesting that the mumps component in the MMR vaccine had low seropositivity (Table). Of the 74 acute mumps cases, seven were not vaccinated. Mumps IgM was positive for these samples; however, they were negative for both mumps and rubella IgG. These samples were positive for measles IgG, because a separate measles vaccine is given at 9 months of age, prior to the MMR vaccine. The proposed mechanisms for mumps vaccine failure include the following: high viral burden in close settings like school and college campus that overcomes herd immunity; suboptimal vaccination in high-risk populations; poor storage and handling practices that lead to virus inactivation and possible waning immunity in previously vaccinated individuals13.
This study showed that mumps infection occurred in MMR vaccinated individuals in Chennai. MMR failed to generate anti-mumps IgG and thus showed low efficacy of vaccine in providing protection against mumps as compared to measles and rubella.
Acknowledgment
Authors thank Drs Srinivasan V, Chitra S, from V.K. Nursing Home, Valasaravakkam, Chennai, and Dr Padmasani Venkat Ramanan, Department of Pediatrics, Sri Ramachandra Medical College & Research Institute, Porur, Chennai, India, for their help in obtaining serum samples.
References
- Recent mumps outbreaks in vaccinated populations: no evidence of immune escape. J Virol. 2012;86:615-20.
- [Google Scholar]
- Assessment of mumps virus-specific antibodies by different serological assays: which test correlates best with mumps immunity? Eur J Clin Microbiol Infect Dis. 2011;30:1223-8.
- [Google Scholar]
- An outbreak of mumps meningoencephalitis in Sangli district. Indian Pediatr. 2007;44:235.
- [Google Scholar]
- An outbreak of mumps in Thiruvananthapuram district. Indian Pediatr. 2004;41:298-300.
- [Google Scholar]
- Centres for Disease Control (CDC). Update: International Task Force for Disease Eradication, 1990 and 1991. MMWR Morb Mortal Wkly Rep. 1992;41:40-2.
- [Google Scholar]
- Does primary immunisation status predict MMR uptake? Arch Dis Child. 2009;94:49-51.
- [Google Scholar]
- Role of laboratory in rapid diagnosis of atypical mumps. Braz J Infect Dis. 2010;14:201-2.
- [Google Scholar]
- Sharp rise in mumps cases in district. Available from: http://ibnlive.in.com/news/sharp-rise-in-mumps-casesin-district/226432-60-122.html
- [Google Scholar]
- Characterisation of mumps virus genotype C among patients with mumps in India. Indian J Med Microbiol. 2013;31:290-2.
- [Google Scholar]




