
Translate this page into:
Look says it all - Clinically recognizable electrical storm
*For correspondence: r_narang@yahoo.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 59 yr old female† presented to the Cardiology department, All India Institute of Medical Sciences, New Delhi, India, in June 2019, with four syncopal episodes and palpitations. Examination showed hypothermia, bradycardia, carotenaemia (Fig. 1) and drowsiness. Electrocardiography showed sinus bradycardia, long QT (580 msec) (Fig. 2) malignant ventricular premature contractions (Fig. 3), leading to runs of ventricular flutter (electrical storm) (Fig. 4). Laboratories showed undetectable thyroid-stimulating hormone (0.001 mU/L), low T3, T4 and all other anterior pituitary hormones were low. Her history revealed lactation failure 30 years back. The diagnosis of Sheehan's syndrome presenting with myxoedema coma and ventricular flutter secondary to acquired long QTc due to hypothyroidism was made and treated with high-dose levothyroxine and corticosteroids. The patient showed dramatic clinical improvement with normalization of QTc interval on five months of follow up. Uniqueness of the case is to highlight that not all ventricular arrhythmias need anti-arrhythmics, and clinical examination is of utmost importance even in the era of artificial intelligence. Sheehan's syndrome is an important reversible cause of electrical storm.

- Characteristic carotenaemia, myxoedemic facies before treatment, with remarkable disappearance following treatment on five-month follow up.
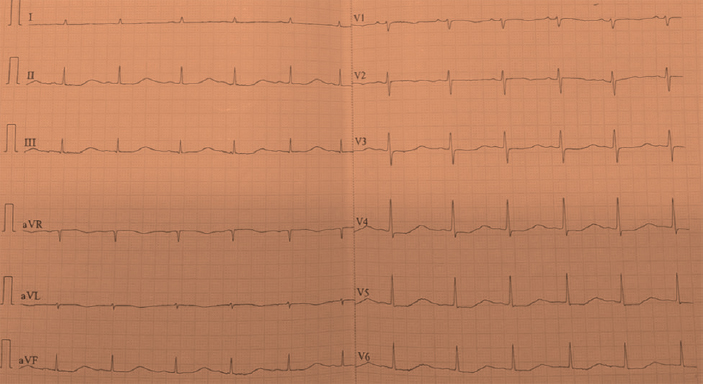
- Baseline electrocardiography – Sinus bradycardia with prolonged QTc of 580 msec.
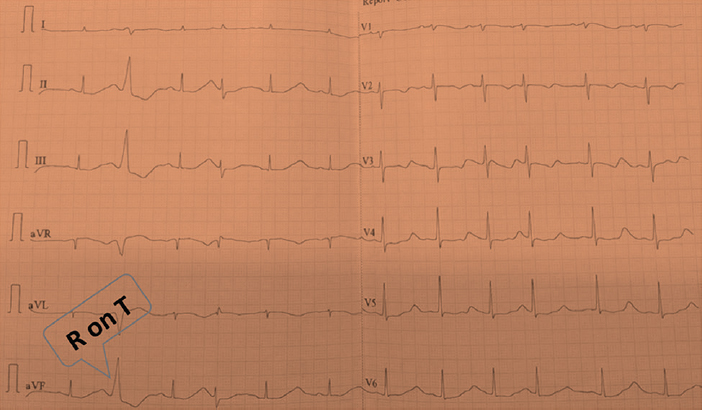
- Electrocardiography showing short-coupled ventricular premature contraction with R on T phenomenon.
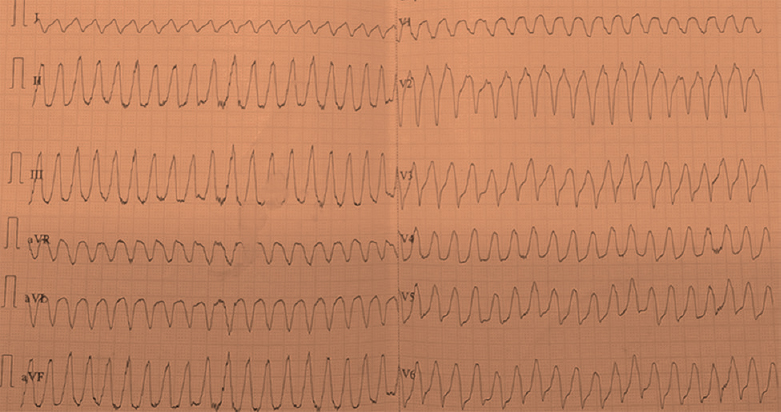
- Ventricular flutter evident on lead I.
Conflicts of Interest: None.




