
Translate this page into:
Long-term outbreak of Klebsiella pneumoniae & third generation cephalosporin use in a neonatal intensive care unit in north India
Reprint requests: Dr Shampa Anupurba, Department of Microbiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi 221 005, Uttar Pradesh, India e-mail: shampa_anupurba@yahoo.co.in
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The indiscriminate use of third generation cephalosporin has contributed to the emergence and widespread dissemination of extended spectrum β lactamases (ESBL) genes in Klebsiella pneumoniae. This study was undertaken to elaborate the genetic behaviour of ESBL - producing K. pneumoniae isolates in the neonatal intensive care unit (NICU) of a tertiary care hospital in north India causing successive outbreaks in context with empirical third generation cephalosporin use.
Methods:
Isolates of K. pneumoniae (43 from blood, 3 from pus and endotracheal tube, 4 from environment) causing successive outbreaks in the NICU of a tertiary care university hospital were studied for two years. Antimicrobial susceptibility testing was done by disc diffusion and minimum inhibitory concentration (MIC) determination by agar dilution methods. ESBL production was determined by phenotypic and genotypic methods. Clonal relatedness among the isolates was studied by enterobacterial repetitive intergenic consensus polymerase chain reaction (ERIC-PCR). Genetic environment of these isolates was assessed by the presence of integrons and gene cassettes. Transformation experiments were done, and plasmids of these isolates were characterized by stability testing and incompatibility testing. Subsequently, a change in the ongoing antibiotic policy was adopted, and corresponding changes in the behaviour of these isolates studied.
Results:
During the period from August 2011 to January 2013, 46 isolates of monoclonal ESBL K. pneumoniae were obtained from different neonates and four similar environmental isolates were studied. Multidrug-resistant ESBL isolates harboured both blaCTXM-15 and blaSHV-5. The dfr and aac-6’ resistant genes were found in gene cassettes. A 50 kb plasmid belonging to IncFIIA group was detected in all the isolates which was transferable and stable. The emergence and regression of the outbreaks coincided with antibiotic usage in the NICU, with widespread empirical use of cefotaxime being responsible for their persistence in the environment.
Interpretation & conclusions:
The study indicates that empirical use of third generation cephalosporins may promote the emergence, persistence, and dissemination of resistant isolates in the hospital environment. Periodic review of antibiotic policy is necessary for rationalized use of antibiotics.
Keywords
Cefotaxime
clonal
extended spectrum β lactamases
Klebsiella pneumoniae
neonatal
outbreak
withdrawal

The association of Klebsiella pneumoniae with several outbreaks, especially in the neonatal intensive care unit (NICU), is an example of the importance of selective antibiotic pressure in relation to infection control measures. With the advent of extended spectrum β lactamases (ESBL), metallo β lactamases (MBL) and subsequently K. pneumoniae carbapenemases, the pathogen has evolved itself to survive. ESBLs have existed in the environment on large multidrug resistance plasmids even before their recognition as a worldwide problem1. Often these present with complex molecular epidemiology with the varied manifestation of their genetic makeup like the presence of different ESBL genes in clonally related strains, plasmid transfer among genotypically unrelated strain or same ESBL gene being mediated by different plasmids in the hospital environment2. All these suggest that both selective antibiotic pressure and plasmid sharing have been responsible for independent evolution and widespread dissemination of ESBLs.
The rise in the emergence and widespread dissemination of the ESBL genes in K. pneumoniae have often been attributed to the increasing use of broad-spectrum antibiotics, the third generation cephalosporins in particular3. In this respect, developing countries have been liberal enough to prescribe this class of antibiotic indiscriminately in clinical practice, though sufficient data in this context do not exist4. In India alone, the sale of cephalosporin has increased tremendously in a period of five years5. Several outbreaks of neonatal sepsis by K. pneumoniae have been reported from India, especially caused by diverse clones of the organism6789. In all these studies the isolates have been characterized along with their sources and all these studies concluded with a need for better antibiotic prescribing practices. However, in depth study of the complex genetic behaviour and adaptability of these isolates has not been done in the hospital against antibiotic use.
Because indiscriminate use of antibiotics modulates the entire environment, especially within hospitals, this study was undertaken to investigate successive outbreaks in the NICU of a tertiary care hospital in north India, due to ESBL producing K. pneumoniae over an extended period and how these complex antibiotic resistance determinants emerged and persisted in the hospital settings against a background of heavy third generation cephalosporin use.
Material & Methods
The study was performed in the department of Microbiology, Sir Sunderlal Hospital, Institute of Medical Sciences, Varanasi, India. The study was approved by the Institute Ethical Committee, and informed written consent was taken from parents/guardians of all the neonates included in the study.
During July 2011, within a period of one week, 12 isolates of phenotypically similar K. pneumoniae were obtained from the blood of neonates admitted in the NICU. The increased frequency of isolation of K. pneumoniae hinted towards the emergence of an outbreak. A microbiological survey of NICU and labour room (LR) environment was immediately done to trace the source of the outbreak because most of the affected newborns were transferred to the NICU directly from the LR. A total of 14 samples were collected from NICU linen, humidifiers, incubator, cradle, water tap, suction fluid and hands of healthcare workers. Ten samples were collected from LR including linen, antiseptic solution in which scissors were kept, water tap, suction tube, humidifier, bed rails and surfaces and hands of healthcare workers.
During a period of three weeks, 20 positive blood cultures from an equal number of newborns were collected. In addition, two K. pneumoniae isolates from the endotracheal tube (ETT) and the third one from a pus sample in the same neonatal unit were also isolated. During the outbreak free period, routine monthly surveillance cultures in the NICU and LR revealed the presence of four K. pneumoniae isolates in the bed rails and floor of the LR.
After a gap of almost eight months, a similar isolate was obtained from the blood culture of a neonate in the same NICU on May 2, 2012 followed by isolation of another 16 such isolates from the blood of septicaemic neonates in a period of four weeks. Following this, there was again increased isolation of K. pneumoniae from blood samples from August 30 to September 15, 2012 (total five isolates). A single similar isolate was reported on January 4, 2013. The NICU was on constant monitoring and in 2013 further no such isolate was detected (Fig. 1).
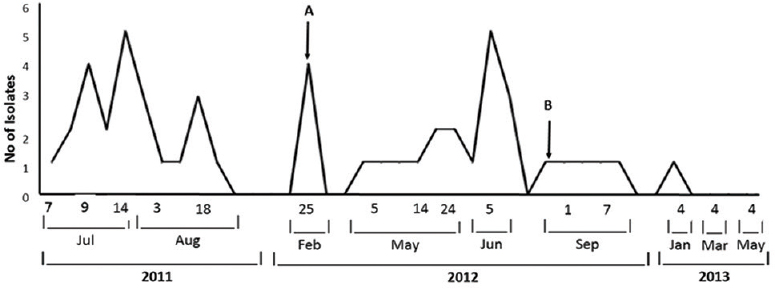
- Distribution of the isolates during the study period. A: Isolation of environmental isolates of K. pneumoniae. B: Initiation of change in antibiotic policy.
Isolation and identification of isolates from blood culture and other samples were done as per standard protocol10. All the samples from the environment were collected in nutrient broth and subcultured on blood agar (HiMedia, Mumbai) and MacConkey agar (HiMedia). The identification of K. pneumoniae isolates was based on extensive biochemical tests11.
Antimicrobial susceptibility testing: The isolates were subjected to antimicrobial susceptibility testing by Kirby-Bauer disc diffusion method12 following the zone size criteria recommended by the Clinical Laboratory Standards Institute13. The antibiotics used were ampicillin (AM, 10 μg), amikacin (AK, 30 μg), gentamicin (GEN, 30 μg), ciprofloxacin (CIP, 5 μg), levofloxacin (LVX, 5 μg), trimethoprim-sulphamethoxazole (SXT, 7.5/2.5 μg), piperacillin/tazobactam (PTZ, 100/10 μg), ceftazidime (CAZ, 30 μg), ceftriaxone (CRO, 30 μg), cefepime (CPM, 30 μg), imipenem (IPM, 10 μg), and meropenem (MEM, 10 μg) (HiMedia). Determination of minimum inhibitory concentration (MIC) values for ampicillin, ceftazidime, cefepime and imipenem was done by agar dilution method12. All these isolates were tested for ESBL production by the combination disc method using ceftazidime (30 μg) and ceftazidime/clavulanic acid (30/10 μg) and cefotaxime (30 μg) and cefotaxime/clavulanic acid (30/10 μg)13. K. pneumoniae ATCC 700603 was used as positive control and Escherichia coli ATCC 25922 was used as negative control.
Study of clonal relationship: To study the clonal relatedness, all K. pneumoniae isolates collected during the study from varied sources were typed both by arbitrarily primed polymerase chain reaction (PCR) technique using ‘primer 7’ (5’GTGGATGCGA3’)14 and enterobacterial repetitive intergenic consensus (ERIC) PCR using primers ERIC1R (5’ATGTAAGCTCCTGGGGATTCAC3’) and ERIC2 (5’AAGTAAGTGACTGGGGTGAGCG3’) primers15. DNA patterns were compared visually.
Characterization of ESBL genes and their genetic environment: Multiplex PCR for detection and characterization of ESBL genes was done using primers for blaTEM, blaSHV, blaCTXM1,2,9 and blaOXA2,10 as described elsewhere16. The PCR products were purified and sequenced (Genei, Bengaluru) to detect the type of ESBL genes. Class 1 and Class 2 integrons were detected by integrase gene PCR17.
Analysis of the genetic environment of the ESBL genes was done by 59-base element PCR18. PCR products were extracted and purified (extraction kit, Qiagen Inc., CA) and subjected to DNA sequencing (Genei) followed by sequence analysis using BLAST suite programs (www.ncbi.nlm.nih.gov/Blast.cgi).
Study of transfer of resistance: Study of transfer of resistance was performed as described elsewhere19. Briefly, conjugation experiments were carried out between clinical isolates as donors and streptomycin resistant E. coli recipient strain B (Genei, Bengaluru). Overnight culture of the bacteria were diluted in Luria Bertani (LB) broth (HiMedia, Mumbai) and was grown at 37°C till the optical density of the recipient and donor culture reached 0.8-0.9 at A600. Donor and recipient cells were mixed at 1:5 donor-to-recipient ratios and transconjugants were selected on cefotaxime (0.5 mg/l) and streptomycin (1000 mg/l) agar plates. The transformation was also carried out using E. coli JM107 (Fermentas, USA) as recipient. Transformants were selected on cefotaxime (0.5 mg/l) containing LB agar plates.
Characterization of plasmids: Plasmid stability and fitness were assessed by serial passage of blaCTX-M, SHV positive isolates on LB broth without any antibiotic pressure. After each passage, the isolates were tested for the presence of blaCTXM, SHV by PCR assay17. Isolation of plasmids was done by isopropanol precipitation method, and plasmid size was estimated on 0.8 per cent agarose20. For the detection of incompatibility group of plasmid in transconjugant with blaCTXM, SHV as well as in the donor strains, PCR-based replicon typing was carried out targeting 18 different replicon types21.
Antibiotic usage in the NICU: Initially, the NICU in our hospital followed an antibiotic policy based on empirical treatment with ampicillin and cefotaxime to neonates suspected with septicaemia. After the first outbreak, following the detection of ESBL producing K. pneumoniae isolates and their susceptibility reports, neonates were treated with ofloxacin and amikacin. Cefotaxime was withdrawn for a short period (from July 14 to September 22, 2011), only to be reintroduced as before following the initial antibiotic policy. The same strategy was followed with the subsequent successive outbreaks, where cefotaxime was withdrawn from May 30 to June 19, 2012. However, after the regression of the second outbreak, on August 24, 2012 a change in antibiotic policy of the NICU was initiated and continued. Use of third generation cephalosporin was withdrawn and piperacillin-tazobactam along with amikacin was administered empirically. The occurrence of the cases in relation to empirical third generation cephalosporin is shown in Fig. 2.
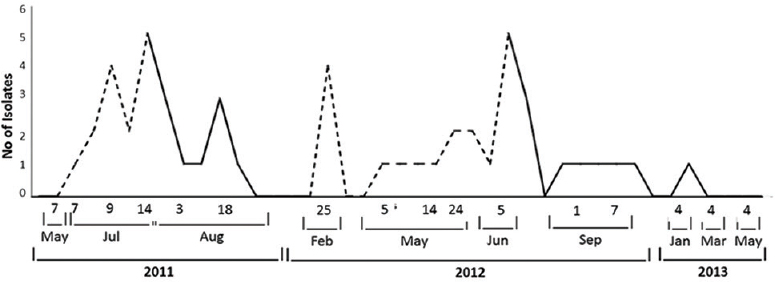
- Occurrence of cases in relation to third-generation cephalosporin use. Dotted and solid lines show the occurrence of cases with and without third generation cephalosporin use, respectively.
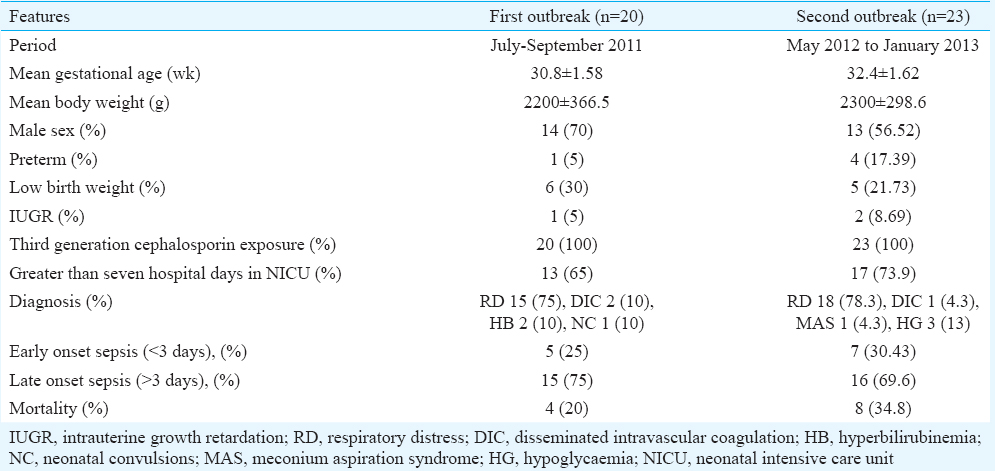
Results
The study included a total of 23 isolates of K. pneumoniae from the first outbreak, 23 isolates from the following successive outbreaks and four environmental isolates. The environmental isolates were collected from the LR in the outbreak free period. No isolate was recovered from the NICU environment. The clinical characteristics of the affected neonates in the two outbreaks are shown in Table I. The overall mortality from the first outbreak was 20 per cent, followed by 34.8 per cent in the successive ones. Detailed history revealed all the neonates were empirically treated with cefotaxime and amikacin as per the antibiotic policy. Table II shows the characteristics of K. pneumoniae isolates obtained during the two outbreaks. All 23 isolates obtained from the first and the second outbreaks each contained class 1 integron.
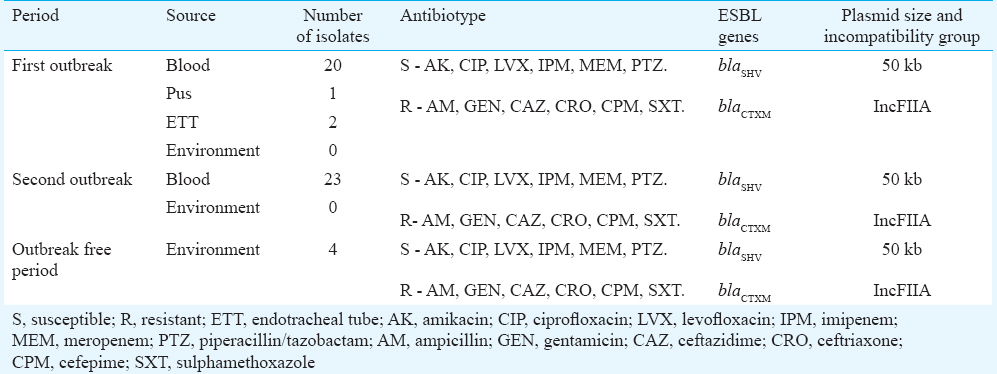
Antimicrobial susceptibility testing: It was found that all the isolates recovered from the clinical and environmental samples showed uniform antibiotic susceptibility pattern showing resistance to ampicillin (MIC >256 µg/ml), gentamicin, trimethoprim/sulphamethoxazole, extended spectrum cephalosporins (ceftazidime MIC >512 µg/ml, cefepime MIC >256 µg/ml) and susceptibility to amikacin, fluoroquinolones (both ciprofloxacin and levofloxacin), imipenem (MIC <0.5 µg/ml), meropenem and piperacillin-tazobactam (Table II). ESBL screening test yielded positive results for all the isolates (100%) along with phenotypic confirmation with combination disc test.
Study of clonal relation: All the K. pneumoniae isolates collected from different neonates and environment showed identical clonal relation thus belonging to a single cluster (cluster A) by both the typing methods used (Fig. 3).
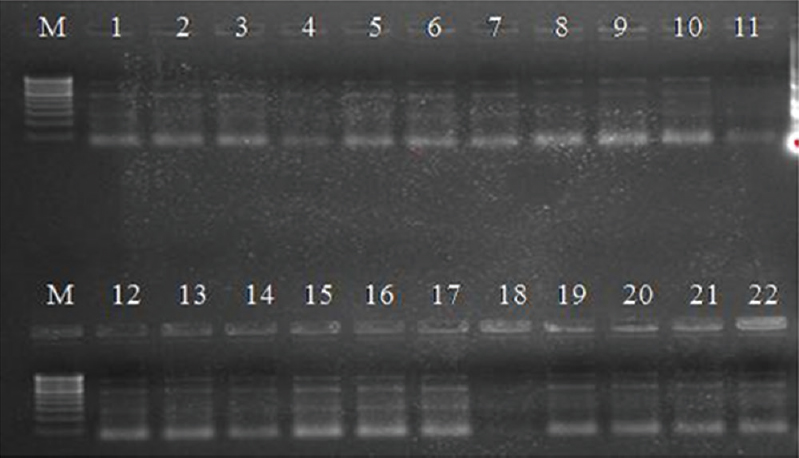
- Molecular typing of K. pneumoniae isolates by ERIC PCR. Lane M: 100 bp ladder, lanes 1-18: Clinical isolates, lanes 19-22: Environmental isolates.
Characterization of ESBL genes and their genetic environment: Molecular characterization of the ESBL genes showed the presence of both blaCTXM and blaSHV genes in 47 (94%) of the isolates and only blaCTXM in three isolates. DNA sequencing of PCR products revealed the presence of blaCTXM-15 and blaSHV-5 genes. All the isolates (100%) were positive for class 1 integrons (160 bp). The genetic environment of these ESBL positive isolates showed the presence of gene cassettes of 400 and 600 bp sizes containing the dihydrofolate reductase gene (dfr) and 6’ N-acetyltransferase (aac-6’) gene, contained in class 1 integron. However, the ESBL genes were not seen to be a member of these cassettes.
Transfer of resistance genes and plasmid analysis: Resistance to ESBL was transferable both by conjugation and transformation from all the ESBL positive K. pneumoniae isolates. A plasmid of approximately 50 kb was detected in all the transformants and transconjugants (Fig. 4). The serial subculture of the transformants, transconjugants and the clinical isolates of K. pneumoniae on antibiotic-free medium revealed that the plasmids were considerably stable. While the transformants and the transconjugants lost their plasmid after the thirteenth subculture, the clinical isolates required an average of 43 subcultures to lose the plasmid harbouring the ESBL genes. PCR-based replicon typing showed that the transferable 50 kb plasmid belonged to the incompatibility group IncFIIA in all the transconjugants and transformants.
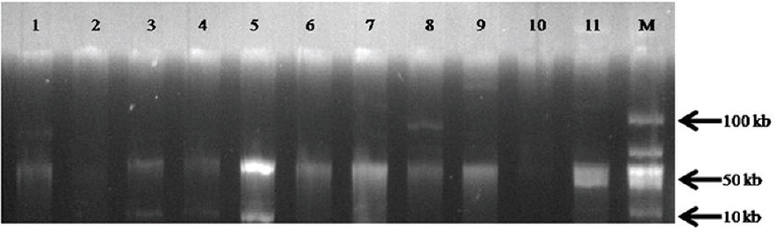
- Profile of plasmids among the transconjugants and transformants. Lanes 1-11: Plasmid (50 kb) in transconjugants and transformants, M: Hyperladder (Bioline, UK).
Discussion
Many outbreaks have been reported globally, affirming the well-noted adaptation of this organism to the nosocomial environment222324. In addition, a few of the studies have also provided some insight into the genetic characteristics of such outbreak strains19252627. However, most of these studies have not focused on the emergence of these isolates in the hospital environment with antibiotic usage. The present study added another aspect to the survival of the ESBL positive K. pneumoniae in the hospital environment and their genetic behaviour amidst antibiotic pressure. This study showed both widespread dissemination and persistence of clonally related isolates of K. pneumoniae in the NICU showing an endemic tendency.
An earlier study has suggested that similar type of successive outbreaks result from the changing multiplication rates of these strains28. Due to some reasons, their number increase causing an outbreak, followed by regression. This phenomenon was depicted in our study also. Additionally, antibiotic selective pressure due to empirical use of third generation cephalosporin was identified as the reason behind the persistence of these isolates. While the selective pressure of third generation cephalosporins resulted in the rapid dissemination of the isolates thus causing the first outbreak, withdrawal of third generation cephalosporin from the NICU environment led to a gradual regression of the K. pneumoniae only to persist in that setup. Later introduction of the same class of antibiotic resulted again in the dissemination of the same clone. Surprisingly, during the outbreak period, no environmental reservoir could be detected. On the other hand, in the outbreak free period similar isolates were found to persist, thus serving as a pool of resistance genes. It could be hypothesized that isolates of K. pneumoniae survived in the hospital environment of the LR in the outbreak free period only to gradually increase in number under the selective pressure of cefotaxime and caused repeated outbreaks. The prompt infection control measures adapted with the onset of the outbreaks might have decreased the number of isolates to undetectable levels.
Spread of blaCTXM-15, SHV-5 genes was associated with plasmids of a single incompatibility group (IncFIIA) carrying class I integrons. The 50 kb plasmid showed considerable stability even without antibiotic pressure. Therefore, once acquired, these resistant determinants remain a threat for long even if use of the antibiotic responsible for their selection is reduced. Coexistence of plasmids carrying ESBL genes along with gene cassettes with other resistant determinants might have increased the chances of survival of these isolates in the hospital environment. The ease of transfer of drug resistance in these isolates is also a cause of concern. In due course of time, these isolates may serve as efficient genetic vehicles for transfer of these resistant determinants.
Both carbapenem and beta lactam-beta lactamase inhibitor combinations have been successfully used as replacements for the cephalosporin29. Therefore, the ongoing policy in our NICU was revised with the use of piperacillin-tazobactam instead of cefotaxime. Piperacillin-tazobactam was considered due to its established significant protective effect in reducing ESBL producing K. pneumoniae infections3. Carbapenems were preserved as the last resort drugs in case of serious illnesses. In addition, infection control practices were reinforced as a preventive measure despite the lack of evidence of the outbreak strains in its direct environment. The last isolate was reported after a sufficient period (four months) since the change in empirical treatment policy. This implied that reducing selective pressure alone was not enough to eradicate these isolates. Due to unpredictable nature of these isolates, a thorough environmental surveillance at regular intervals should be done.
As suggested earlier1927, ESBL strains usually harbour multiple resistant genes conferring resistance to several classes of antibiotics namely aminoglycosides and fluoroquinolones. Consequently, it is easy for these strains to persist in the nosocomial environment. In addition, outbreaks of ESBL K. pneumoniae with transferable plasmids are typically polyclonal29. Contrary to this, despite fluoroquinolone susceptibility and lack of multidrug resistance, a prompt change in antibiotic therapy could not produce sustained effects to completely eradicate these monoclonal isolates. The concern is that if these isolates with complex genetic structures, harbouring drug resistance genes, gene cassettes and mobile plasmids survive in the hospital environment, with the passage of time, these may evolve to become reservoirs of mobile elements. As behaviour of these organisms is complex, it can only be speculated that withdrawal of a particular antibiotic for a defined period can be adopted as a temporary measure to control. For their complete eradication, an integrated approach considering strict vigilance on infection control measures, frequent reviewing of antibiotic policies and prudent use of antibiotics may be required.
In conclusion, this study emphasizes the importance of controlled empirical use of antibiotics which could contribute immensely to the genetic behaviour of pathogens within the hospital environment, along with the need for stringent infection control practices in the NICU. It is also important to review the existing policies and guidelines for rationalized use of antibiotics.
Acknowledgment
The authors thank Banaras Hindu University, Varanasi for providing financial assistance to conduct the study.
Conflicts of Interest: None.
References
- Beta-lactamases in laboratory and clinical resistance. Clin Microbiol Rev. 1995;8:557-84.
- [Google Scholar]
- Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005;18:657-86.
- [Google Scholar]
- Extended spectrum beta lactamase-producing Klebsiella pneumoniae infections: a review of the literature. J Perinatol. 2003;23:439-43.
- [Google Scholar]
- Third generation cephalosporin use in a tertiary hospital in Port of Spain, Trinidad: need for an antibiotic policy. BMC Infect Dis. 2004;4:59-66.
- [Google Scholar]
- Global Antibiotic Resistance Partnership (GARP) – India Working Group. Rationalizing antibiotic use to limit antibiotic resistance in India. Indian J Med Res. 2011;134:281-94.
- [Google Scholar]
- Nosocomial outbreak of septicaemia in Neonatal Intensive Care Unit due to extended spectrum ß-lactamase producing Klebsiella pneumoniae showing multiple mechanisms of drug resistance. Indian J Med Microbiol. 2010;28:380-4.
- [Google Scholar]
- Neonatal septicaemia caused by diverse clones of Klebsiella pneumoniae & Escherichia coli harbouring blaCTX-M-15. Indian J Med Res. 2013;137:791-9.
- [Google Scholar]
- An outbreak of extended spectrum beta-lactamase producing Klebsiella pneumoniae in a Neonatal Intensive Care Unit. Indian J Pathol Microbiol. 2007;50:669-70.
- [Google Scholar]
- Sepsis in neonates due to imipenem-resistant Klebsiella pneumoniae producing NDM-1 in India. J Antimicrob Chemother. 2011;66:1411-3.
- [Google Scholar]
- Culture of bacteria. In: Collee JG, Fraser AG, Marmion BP, Simmons A, eds. Mackie and McCartney practical medical microbiology (14th ed). London: Churchill Livingstone; 1996. p. :113-30.
- [Google Scholar]
- Enterobacteriaceae: Escherichia, Klebsiella, proteus and other genera. In: Collee JG, Fraser AG, Marmion BP, Simmons A, eds. Mackie and McCartney practical medical microbiology (14th ed). London: Churchill Livingstone; 1996. p. :361-84.
- [Google Scholar]
- Antimicrobial susceptibility testing by the Kirby-Bauer disc diffusion method. Ann Clin Lab Sci. 1973;3:135-40.
- [Google Scholar]
- Clinical Laboratory and Standards Institute. In: Performance standard for antimicrobial susceptibility testing: twenty first informational supplement M100. Wayne, PA: CLSI; 2011. p. :31.
- [Google Scholar]
- Multicenter evaluation of arbitrarily primed PCR for typing of Staphylococcus aureus strains. J Clin Microbiol. 1995;33:1537-47.
- [Google Scholar]
- Presence of qnr gene in Escherichia coli and Klebsiella pneumoniae resistant to ciprofloxacin isolated from pediatric patients in China. BMC Infect Dis. 2008;8:68-74.
- [Google Scholar]
- Detection of OXA-2 group extended-spectrum-beta-lactamase-producing clinical isolates of Escherichia coli from India. J Antimicrob Chemother. 2007;60:703-4.
- [Google Scholar]
- Observation on integron carriage among clinical isolates of Klebsiella pneumoniae producing extended-spectrum beta-lactamases. Indian J Med Microbiol. 2010;28:207-10.
- [Google Scholar]
- Site-specific insertion of genes into integrons: role of the 59-base element and determination of the recombination cross-over point. Mol Microbiol. 1991;5:1941-59.
- [Google Scholar]
- Outbreak caused by a multi-resistant Klebsiella pneumoniae strain of new sequence type ST341 carrying new genetic environments of aac(6’)-Ib-cr and qnrS1 genes in a Neonatal Intensive Care Unit in Spain. Int J Med Microbiol. 2010;300:464-9.
- [Google Scholar]
- A procedure for large-scale plasmid isolation without using ultracentrifugation. Biotechnol Appl Biochem. 1992;16:211-5.
- [Google Scholar]
- Identification of plasmids by PCR-based replicon typing. J Microbiol Methods. 2005;63:219-28.
- [Google Scholar]
- Risk factors for colonization and infection in a hospital outbreak caused by a strain of Klebsiella pneumoniae with reduced susceptibility to expanded-spectrum cephalosporins. J Clin Microbiol. 2004;42:4242-9.
- [Google Scholar]
- Analysis of three outbreaks due to Klebsiella species in a Neonatal Intensive Care Unit. Infect Control Hosp Epidemiol. 2003;24:495-500.
- [Google Scholar]
- Multiclonal outbreak of Klebsiella pneumoniae producing extended-spectrum beta-lactamase CTX-M-2 and novel variant CTX-M-59 in a Neonatal Intensive Care Unit in Brazil. Antimicrob Agents Chemother. 2008;52:1790-3.
- [Google Scholar]
- A long-term low-frequency hospital outbreak of KPC-producing Klebsiella pneumoniae involving intergenus plasmid diffusion and a persisting environmental reservoir. PLoS One. 2013;8:e59015.
- [Google Scholar]
- Complex clonal and plasmid epidemiology in the first outbreak of Enterobacteriaceae infection involving VIM-1 metallo-beta-lactamase in Spain: toward endemicity? In: Clin Infect Dis. Vol 45. 2007. p. :1171-8.
- [Google Scholar]
- Containment of an outbreak of KPC-3-producing Klebsiella pneumoniae in Italy. J Clin Microbiol. 2011;49:3986-9.
- [Google Scholar]
- Molecular epidemiology of multidrug resistant extended-spectrum β-lactamase producing Klebsiella pneumoniae outbreak in a Neonatal Intensive Care Unit. Int J Collab Res Internal Med Public Health. 2010;2:226-37.
- [Google Scholar]
- Controlling antibiotic resistance in the ICU: different bacteria, different strategies. Cleve Clin J Med. 2003;70:793-800.
- [Google Scholar]




