
Translate this page into:
Lessons learnt during the first 100 days of COVID-19 pandemic in India
*For correspondence: drrajesh.bhatia1953@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
The COVID-19 pandemic due to SARS-CoV-2 commenced in China in December 2019, was declared as a public health emergency of international concern by the World Health Organization (WHO) on January 30, 20201 and a pandemic on March 11, 20202. As of May 10, 3,925,815 cases of COVID-19 and 274,488 deaths from 215 countries3 have been reported to the WHO. The first case of COVID-19 in India was reported on January 30, 202045. Till May 10, 67,152 cases with 2,206 deaths had taken place in India6.
India's efforts have been directed to contain the spread of COVID-19, halt its local transmission and mitigate the impact of the outbreak. In the process several lessons have been learnt, some of which are briefly described hereunder.
Early response, effective command, whole-of-government approach and strong political leadership ensure focused and coordinated actions
Preparations for responding to potential pandemic in India began soon after the Wuhan event became public in January 2020. Initial COVID-19 cases in India comprised students coming back from China and Italian tourists. Thermal screening of passengers arriving from China began on January 21, 2020 and was subsequently extended to all countries. All visas, except diplomatic and official visas, were suspended. Indians returning from COVID-19-affected countries were asked to be quarantined for 14 days. In March 2020, all international and domestic flights, passenger trains and road transport with the exception of those carrying essential items were suspended. Disaster management response was activated under the overall supervision and guidance of the Prime Minister, of India.
Existing laws provide legal framework for control activities
The Epidemic Disease Act of India, 19877, has been on statute for more than a century. The Disaster Management Act8 was passed by the Indian Parliament in 2005. These legislative tools provide widespread legal power to civil authorities to implement pandemic control measures, thus ensuring cooperation from the public and reporting of cases by the medical professionals irrespective of their affiliation to public or private sector.
Evidence-based strategy to reduce viral transmission worked for a shorter time
A nationwide lockdown for 21 days was declared on March 24, 20209 and subsequently extended till May 310. Initially, the impact of lockdown was visible11. The doubling rate for COVID-19 in India prior to lockdown was 3.4. It improved to 7.5 by April 19, 202012 and 12.9 in the second week of May13. The lockdown provided the much-needed time to strengthen health system response and ensure public engagement.
In spite of the extensive and prolonged lockdowns, increase in the doubling time of occurrence of cases and the number of new cases continued to rise in India. The average number of cases reported to the WHO14 per day for three different time segments of lockdown is shown in the Table. The Figure shows the increasing number of daily cases during the last 10 days of this 100-day period. Multiple eruptions of cases in new locations were reported, indicating breaches in the implementation of lockdown. The COVID-19 pandemic has not been uniform in India. One of the possible solutions is to develop and implement operational plans through microplanning for local area using data generated locally.
| Period of lockdown | Average number of cases/day |
|---|---|
| March 25 - April 7 | 331 |
| April 8-30 | 1,211 |
| May 1-10 | 2,989 |
Source: Ref. 14
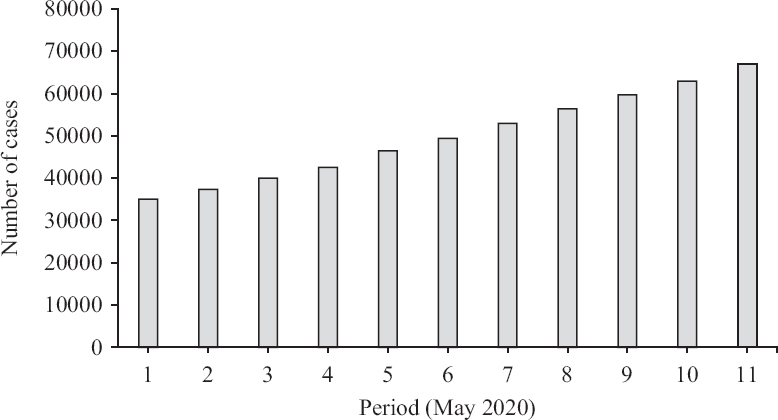
- Rising trend of cases of COVID-19 between May 1-10, 2020. Source: Ref. 14.
Understand the impact of uncontrolled movement of migrant populations
One-third of India's population comprises internal migrants. They work in unorganized sectors and most of them live below the poverty line. A large number of them have moved from far-away central and eastern parts of India to rest of India. The sudden national lockdown made them jobless, without food and apprehensive about them getting infected. Their exodus to native places was not anticipated but had to be curtailed in the context of national lockdown. Soon it became obvious that unless effective steps are taken, these migrants shall start travelling to their native places carrying the virus with them. This was a high-risk public health action with the potential to seed the outbreaks of COVID-19 in different and far-flung rural areas of India, thus requiring utmost surveillance and rapid containment actions.
Pan-India laboratory networks are essential and must be sustained
Apart from an Indian Council of Medical Research (ICMR) network of around 65 Virus Research and Diagnostic Laboratories (VRDLs), India did not have many laboratories that could provide diagnostic support at the beginning of the COVID-19 pandemic. The testing capacity of the entire network was limited to a few thousand samples. It was swiftly scaled up. Till May 10, 2020, India had tested 1,609,037 samples for SARS-CoV-2 virus, giving a rate of around 1200 tests per million people. Of these, 62,937 tested positive15. In the beginning of May 2020, the reverse transcription-polymerase chain reaction (RT-PCR) test facility became available in 360 government and 112 private facilities across the country15, with per day testing capacity of around 90,000. India needs a permanent network of at least 1000 laboratories with PCR facilities with at least one laboratory in each of its 734 districts and multiple such facilities in cities and metros.
Protection and preservation of vulnerable senior citizens should be a priority
India accorded special attention to protect its senior citizens from getting infected with SARS-CoV-2. Of its entire population, 9.3 per cent is between 60 and 79 years16. This large population is extremely vulnerable to COVID-19 and the resultant high mortality. India is also considered the capital of diabetes. Coronavirus patients with heart ailments have almost 10 per cent mortality rate and those with diabetes have mortality rate of seven per cent17. Special efforts were undertaken in India to protect and treat these elderly citizens. Looking at the age distribution of those who succumbed to COVID-19, those aged less than 45 yr made up for 14 per cent; between 45 and 60 yr age group accounted for 34.8 per cent; 51.2 per cent fell in the category of more than 60 years, whereas 42 per cent belonged to the age group of 60-75 yr, 9.2 per cent accounted for above 75 yr category and those with comorbidities formed 78 per cent18. Strong risk communication strategies and access to medical care are essential to preserve and protect this population.
Frontline workers need protection from infection and ignorant communities
The professional responsibilities of frontline workers bring them close to the known and unknown sources of exposure. Availability and the use of personal protective equipment (PPE) are mandatory for them. The Indian society showed substantial respect for these 'Corona Warriors'. However, there were a few unfortunate instances where communities, out of ignorance, protested against their living in the neighbourhood. Apart from educating these communities, the national authorities amended the Epidemic Act, 189719 and introduced harsh legal penalties to those who harassed frontline workers. Active dialogue with the communities to promote their engagement to recognize and respect these workers is the need of the hour.
Harnessing all national resources is a swift and cost-effective approach
Infrastructure and expertise available in different sectors namely research institutes or universities, other government departments and the private sector, especially the diagnostic laboratory services, have been and are being extensively used in India. The success of this endeavour augurs well for the future and needs to be employed in harnessing tremendous expertise and infrastructure available in different sectors.
Public engagement is the key to contain COVID-19 pandemic
COVID-19 pandemic is driving home the irrefutable evidence that mitigation of the pandemic warrants immediate application of evidence-based non-pharmaceutical interventions (NPIs) by an empowered and educated community. The pharmaceutical interventions (drugs and vaccines) are not likely to become accessible to developing countries during the next few months and hence NPIs mainly hand hygiene, respiratory hygiene and social distancing shall be the major elements to prevent and contain COVID-19. All these require sustained public cooperation20. A positive change in the behaviour of the communities in implementing NPIs is a prerequisite. There is a need to learn from the success obtained by TB and HIV programmes by engaging civil society.
Responsible role of mainstream and social media is crucial
The reach of mainstream media in the dissemination of appropriate and accurate information is huge. Several messages of public health importance have been generously transmitted by electronic and print media. Social media has now become an integral part of human life. WhatsApp is widely used, deeply penetrated in the country and is free. Used rationally, this can be an excellent tool for social communication and accessing reliable information21.
Encourage R&D at national level and participate in global research activities
India is considered world pharmacy because of the huge manufacturing capacity for medical devices, vaccines and medicines. Global vaccine manufacturers are also looking forward to Indian industries to collaborate to scale-up the production volumes once an approved vaccine or other pharmaceutical products become available. Indian pharmaceutical companies have also begun trials for many new vaccines and medicines22. A collaboration between academia and industry must be catalyzed. The National Regulatory Authority should, in advance, put in place mechanisms to fast-track the approval processes so that quality-assured tools to combat the pandemic become available at the earliest.
One-Health approach for early detection and control of pandemics
Millions of viruses, including coronaviruses, are circulating in wildlife and most of these have the potential to infect humans23. A need for undertaking joint surveillance by human health and animal health has also been expressed24, for early detection of zoonotic infections.
Mathematical models fail to predict the biological phenomenon of infectious diseases
Several mathematical models projected the severity of pandemic in terms of cases and deaths. At least in the context of India, none of these proved correct. Estimates that emerge from modelling studies are only as good as the validity of the epidemiological or statistical model used; and accuracy of assumptions made for modelling25. It was obvious that the models proposed during the COVID-19 pandemic carried a strong element of bias and used assumptions which proved to be far from real. The power of these models to influence policy decisions for advance planning is a huge risk. Predicting infectious diseases for a novel pathogen is an extremely perilous proposition and should be avoided.
Pandemic should not interrupt or disrupt non-COVID-19 healthcare services to people
The COVID-19 pandemic is an add-on to the existing health problems of the communities. Some of these require continuous monitoring and interventions (e.g., cancer therapy), emergencies (e.g., myocardial infarction, stroke)26, uninterrupted supply of anti-TB and antiretroviral drugs, antenatal care and regular immunization of children. Arrangements must be made to obviate their discontinuation or irregular availability. Health system must be robust enough to address these issues along with mounting of strong fight against the pandemic.
Conclusions
India's COVID-19 Containment Strategy has been aligned with WHO's Strategic Preparedness and Response Plan for COVID-1927. During the ongoing pandemic, India could successfully and rapidly scale-up several important interventions. One must never ignore the fact that SARS-CoV-2 is an unknown treacherous enemy. Despite having a rudimentary genetic structure it is proving to be more experienced and intelligent than the entire humanity. It can strike in hitherto unknown ways. It has the potential of causing greater disruption and destruction. India cannot afford any complacency. Caution should be the keyword during the days to come.
Conflicts of Interest: None.
Conflicts of Interest: None.
References
- Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). Available from: https://wwwwhoint/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov)
- WHO Director General's opening remarks at the media briefing on COVID-19 -March 11, 2020. Available from: https://wwwwhoint/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020">https://wwwwhoint/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020
- Coronavirus disease (COVID-19) pandemic. Geneva: WHO; 2020.
- Novel Coronavirus (2019-nCoV) Situation Report - 11 2020
- First confirmed case of COVID-19 infection in India: A case report. Indian J Med Res. 2020;151:490-2.
- [Google Scholar]
- COVID-19 Dashboard. Available from: https://wwwmohfwgovin/">https://wwwmohfwgovin/
- Disaster Management Act, 2005. Available from: https://wwwndmagovin/images/ndma-pdf/DM_act2005pdf">https://wwwndmagovin/images/ndma-pdf/DM_act2005pdf
- Government of India issues orders prescribing lockdown for containment of COVID-19 epidemic in the country. Available from: https://pibgovin/PressReleasePageaspxPRID=1607997">https://pibgovin/PressReleasePageaspxPRID=1607997
- Lockdown measures for containment of COVID-19 pandemic in the country to continue to remain in force up to May 3, 2020. Available from: https://pibgovin/PressReleasePageaspxPRID=1614481
- GoM reviews current status, and actions for management of COVID-19. Available from: https://pibgovin/PressReleasePageaspxPRID=1615392">https://pibgovin/PressReleasePageaspxPRID=1615392
- Updates on COVID-19; April 20, 2020. Available from: https://pibgovin/PressReleasePageaspxPRID=1616415">https://pibgovin/PressReleasePageaspxPRID=1616415
- 15th meeting of GoM on COVID-19 held; reviews current status, preparedness and actions for management of COVID-19. Available from: https://pibgovin/PressReleasePageaspxPRID=1624057">https://pibgovin/PressReleasePageaspxPRID=1624057
- Coronavirus disease (COVID-2019) situation reports. Available from: https://wwwwhoint/emergencies/diseases/novel-coronavirus-2019/situation-reports">https://wwwwhoint/emergencies/diseases/novel-coronavirus-2019/situation-reports
- Total operational (initiated independent testing) laboratories reporting to ICMR. Available from: https://wwwicmrgovin/pdf/covid/labs/COVID_Testing_Labs_09062020pdf">https://wwwicmrgovin/pdf/covid/labs/COVID_Testing_Labs_09062020pdf
- net Diabetes prevalence (% of population ages 20 to 79). Available from: https://wwwpopulationpyramidnet/hnp/diabetes-prevalence-ages-20-to-79/2015/">https://wwwpopulationpyramidnet/hnp/diabetes-prevalence-ages-20-to-79/2015/1
- Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323:1061-9.
- [Google Scholar]
- Updates on COVID-19; April 30, 2020. Available from: https://wwwpibgovin/PressReleasePageaspxPRID=1619609">https://wwwpibgovin/PressReleasePageaspxPRID=1619609
- Updates on COVID-19; April 23, 2020. Available from: https://pibgovin/PressReleasePageaspxPRID=1617510">https://pibgovin/PressReleasePageaspxPRID=1617510
- Public engagement is the key to contain COVID-19 pandemic. Indian J Med Res. 2020;151:118-20.
- [Google Scholar]
- WhatsApp and MyGov launch official coronavirus and Covid-19 alert service for India, here is how you can use it. Available from: https://wwwindiatodayin/technology/news/story/whatsapp-and-mygov-launch-official-coronavirus-and-covid-19-alert-service-for-india-here-is-how-you-can-use-it-1658295-2020-03-21">https://wwwindiatodayin/technology/news/story/whatsapp-and-mygov-launch-official-coronavirus-and-covid-19-alert-service-for-india-here-is-how-you-can-use-it-1658295-2020-03-21
- Guidance for evaluation of novel applications for COVID-19. Available from: https://wwwicmrgovin/cnaclaimshtml">https://wwwicmrgovin/cnaclaimshtml
- Need for integrated surveillance at human-animal interface for rapid detection and response to emerging corona viral infections using One Health approach. Indian J Med Res. 2020;151:132-5.
- [Google Scholar]
- Implementation framework for one health approach. Indian J Med Res. 2019;149:329-31.
- [Google Scholar]
- Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. Available from: https://wwwimperialacuk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020pdf">https://wwwimperialacuk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020pdf
- Impact of COVID-19 pandemic on health system & Sustainable Development Goal 3. Indian J Med Res. 2020;151:395-9.
- [Google Scholar]
- Strategic preparedness and response plan. Available from: https://wwwwhoint/publications-detail/strategic-preparedness-and-response-plan-for-the-new-coronavirus">https://wwwwhoint/publications-detail/strategic-preparedness-and-response-plan-for-the-new-coronavirus




