
Translate this page into:
Langerhans cell histiocytosis
*For correspondence: menonara@yahoo.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A two years old girl† was admitted to the Pediatric ward of Command Hospital, Lucknow, India, in May 2013 with polyuria and polydipsia. Her height, weight and developmental milestones were appropriate for age. Plasma glucose (random, 86 mg/dl), serum sodium [132 mEq/l (normal range 135-145)], and serum osmolality [284 mOsm/kg (285-295)], were normal. However, urine osmolality was 34 mOsm/kg (normal range 300-900). Magnetic resonance imaging (MRI) brain showed normal pituitary stalk thickness and absence of posterior pituitary bright spot (Fig. 1). Based on the symptoms, hypo-osmolar urine and findings of the MRI brain, she was diagnosed to have central diabetes insipidus (DI) and started on desmopressin nasal spray.
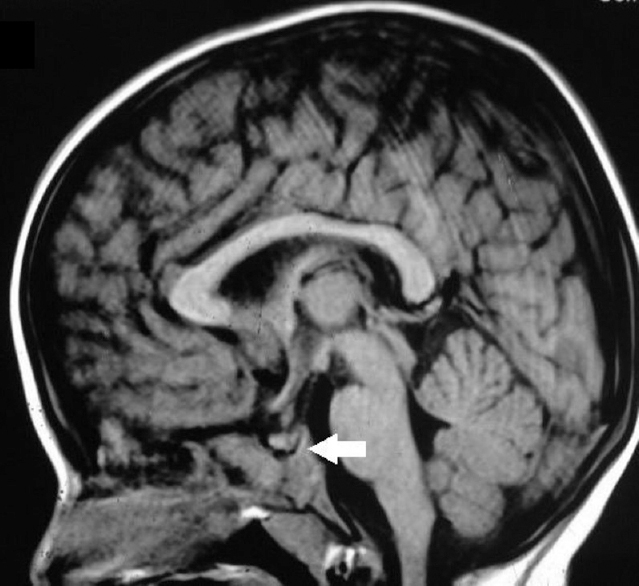
- Magnetic resonance imaging of the brain showing the absence of posterior pituitary bright spot (arrow).
One year later, she developed induration over the right gluteal region which later developed into fistula (Fig. 2). Biopsy of the wall revealed numerous Langerhans cells (reniform nucleus and abundant pink cytoplasm) with characteristic immunoreactivity for CD1a antigen (Figs. 3 and 4). Skeletal survey and positron emission tomography-computed tomography (PET-CT) did not show any other organ involvement. She was diagnosed to have multisystem Langerhans cell histiocytosis (pituitary and skin) and treated with chemotherapy (prednisolone, vinblastine and 6-mercaptopurine) which led to the healing of cutaneous lesion. The patient has been on follow up for the last three years; though in clinical remission she is continued on desmopressin spray due to the persistence of DI.

- Sinus on the right gluteal region.
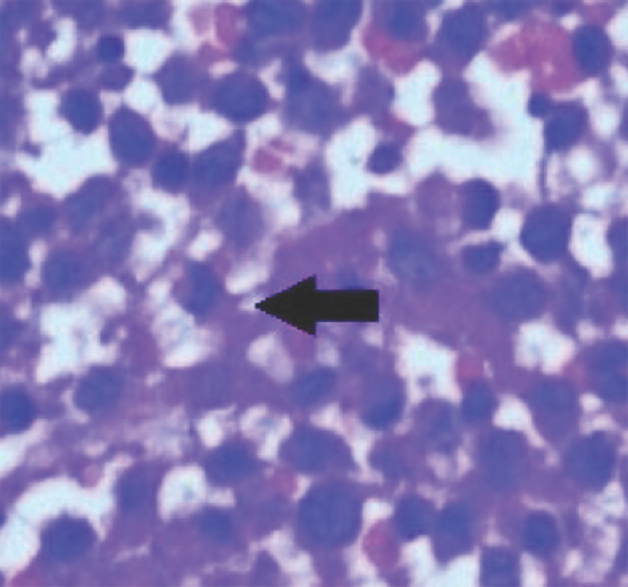
- Biopsy of induration wall showing Langerhans cell with blue reniform nucleus (arrow) (Hemotoxylin and Eosin, ×20).

- Biopsy showing diffuse positivity for CD1a antigen (brown precipitate) (immunohistochemical, 3'3 diaminobenzidine (DAB)-chromogen, ×20).
Conflicts of Interest: None.




