
Translate this page into:
Lack of association between FokI polymorphism in vitamin D receptor gene (VDR) & type 2 diabetes mellitus in the Tunisian population
Reprint requests: Dr Riadh Jemaa, Laboratoire de Biochimie, Hôpital la Rabta, 1007, Jabbari, Tunis, Tunisia e-mail: jemaa_riadh@yahoo.fr
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The impact of several environmental and genetic factors on diabetes is well documented. Though the association between the vitamin D receptor (VDR) gene polymorphisms and type 2 diabetes mellitus (T2DM) has been analyzed in different ethnic groups, the results have been inconsistent. The aim of this study was to evaluate the possible association between VDR FokI polymorphism and genetic susceptibility to T2DM in Tunisian population.
Methods:
A total of 439 unrelated patients with T2DM and 302 healthy controls were included in the study. Genomic DNA was extracted from blood and genotyped for the single nucleotide polymorphism (SNP) of FokI (T/C: (rs2228570) by polymerase chain reaction and restriction fragment length polymorphism (PCR-RFLP) analysis.
Results:
The genotype distribution and the relative allelic frequencies for the FokI polymorphism were not significantly different between T2DM and controls: in T2DM patients the frequencies of the CC, CT, and TT genotypes were 52.6, 41.0, and 6.1 per cent, respectively, and in controls the genotype frequencies were 55.6, 38.7, and 5.6 per cent, respectively. In our study, the TT genotype of the FokI polymorphism was not associated with T2DM (OR =1.19, 95% CI 0.63 - 2.25, P=0.577).
Interpretation & conclusions:
Our study showed no significant association of the FokI polymorphism in the vitamin D receptor gene with type 2 diabetes mellitus in Tunisian population.
Keywords
FokI
single nucleotide polymorphism
T allele
type 2 diabetes
VDR

The incidence of type 2 diabetes mellitus (T2DM) is increasing at an alarming rate worldwide. T2DM is a multifactorial metabolic disorder, influenced by both genetic and environmental factors and exhibits a wide range of disparities among different ethnic groups12345. The identification of genes predisposing to T2DM could provide means to better understand the pathogenesis of the disease and result in better prevention and treatment.
Vitamin D deficiency is shown to be associated with glucose intolerance, insulin resistance, metabolic syndrome, and increase risk for diabetes6. Vitamin D exerts its actions on target tissues through its binding to the cytosolic/nuclear vitamin D receptor (VDR), which is a member of the steroid/thyroid hormone receptor family that functions as a transcriptional activator of many genes. The gene encoding the VDR is located on chromosome 12q13.17, contains 11 exons and spans approximately 75 kb. Several polymorphisms have been identified in the VDR gene, and their functional significance and potential effects on disease susceptibility have been investigated8. Among these polymorphisms, the FokI polymorphism (ATG→ACG) located in the exon2 of the gene is the only known locus affecting the structure of the VDR protein produced. The T allele encodes a 427 amino acid protein while the C allele encodes a 424 amino acid protein91011. The shorter VDR protein variant seems to function more effectively and further increases its capacity of binding 1,25-dihydroxyvitamin D12, and the relatively higher level of vitamin D, in turn, can reduce the risk of T2DM by enhancing pancreatic b-cell secretion function and improve insulin resistance13. This biological mechanism could explain the association between the T allele of FokI polymorphism and susceptibility to T2D.
Several epidemiologic studies have examined the association of the FokI polymorphism of the VDR gene and T2DM, and the results are inconsistent across different populations141516171819. The aim of the present study was to analyze the association between the FokI polymorphism of the VDR gene and TD2M in a sample of the Tunisian population.
Material & Methods
A total of 741 individuals were included in this case-control study. Four hundred thirty nine unrelated patients with T2DM (263 women and 176 men) with mean age of 55.9 ± 9.7 yr were enrolled at the Department of Endocrinology of Rabta University Hospital of Tunis, Tunisia, from January 2007 to July 2009. Diabetes was diagnosed according to the World Health Organization (WHO) criteria20. Diabetes was defined as hyperglycaemia, requiring antidiabetic drugs or testing blood glucose level ≥ 7.0 mmol/l or a 2-h post-challenge glucose level ≥ 11.1 mmol/l. The control group consisted of 302 unrelated individuals (190 women and 112 men) with a mean age of 49.3 ±
9.6 yr, who underwent a medical checkup in our hospital. The exclusion criteria included fasting blood glucose levels of more than 100 mg/dl or a family history of diabetes. Diabetic patients with complications of malignancies were also excluded. Patients and controls were homogeneous Tunisian Arab lineage from Northern Tunisia. Informed written consent was obtained from all participants and the design of the study was approved by the local ethics committee.
Infromation on demography, socio-economic status, education, lifestyle and mental health was collected. Weight and height were measured. Body mass index (BMI; kg/m2) was calculated and obesity was defined as BMI ≥ 30 kg/m2 for both genders21. Hypertension was defined as systolic blood pressure (SBP) ≥ 140 mm Hg and/or diastolic blood pressure (DBP) ≥ 90 mm Hg, or the use of antihypertensive drug treatment or a combination of these. Dyslipidaemia was defined as a total cholesterol (TC) level > 6.47 mmol/l and /or triglyceride level (TG) > 2.26 mmol/l. Smoker definition included both ex-smokers and active smokers. A daily consumption of more than five cigarettes was considered a smoking habit22.
Laboratory analysis: Blood samples (10 ml) were obtained after an overnight fast. Blood glucose, TC, TG and high-density lipoprotein cholesterol (HDL-C) were measured in the hospital laboratory on a Hitachi 912 analyzer (Roche Diagnostics, Mannheim, Germany) using the respective reagent kits. Low-density lipoprotein cholesterol (LDL-C) was calculated according to the equation of Friedwald et al23.
DNA analysis: Genomic DNA was prepared from white blood cells by phenol extraction24. Genotyping of the FokI (T/C) (rs2228570) VDR polymorphism was performed with the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method as described previously25. Briefly, a fragment of 265 bp including the Fok1 polymorphism was amplified using two oligonucleotides25:
Forward: 5’-AGCTGGCCCTGGCACTGACTCTGCTCT-3’
Reverse: 5’-ATGGAAACACCTTGCTTCTTCTCCCTC-3’
The PCR product was digested by the restriction enzyme FokI (MBI Fermentas, Vilnius, Lithuania) followed by electrophoresis on a 3 per cent agarose gel stained with ethidium bromide and visualized using ultraviolet illumination. The wild type homozygote (CC), heterozygote (CT) and mutant homozygote (TT) showed one band (265 bp), three bands (265, 196 and 69 bp) and two bands (196 and 69 bp), respectively (Figure). The genotype of each sample was determined by two technicians working independently and for quality control, 20 per cent of the samples were selected at random for repeated genotyping and concordance was 100 per cent.
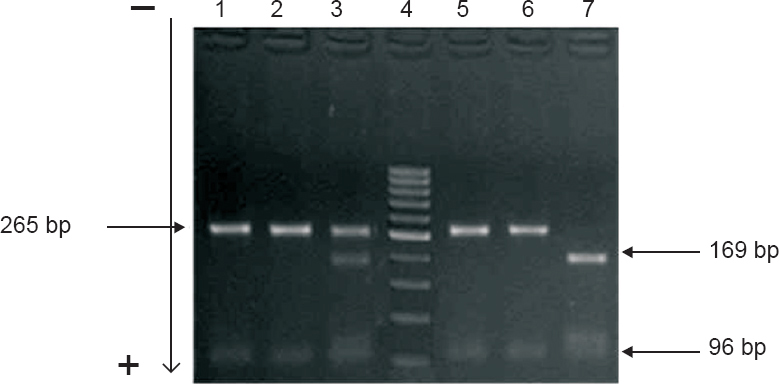
- The FokI digestion profiles of the 265 bp PCR product of the VDR gene homozygous (CC) individuals showing an undigested 265 bp product (lands 1, 2, 5 and 6); heterozygous (CT) individuals showing 265, 196, and 69 bp fragments (lane 3); homozygous (TT) showing 196 and 69 bp fragments (lane 7). GeneRuler DNA ladder (1000-50 bp) (lane 4).
Statistical analysis: Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS 15.0 for windows, SPSS Inc., Chicago, IL, USA). Distributions of continuous variables in groups were expressed as mean ± SD, and compared with unpaired Student's t test. c2 test was used to test for departures from Hardy-Weinberg equilibrium and to compare genotype distributions between groups. Odds ratio (OR) at 95% confidence interval (CI) was determined to describe the strength of association by logistic regression model.
Results
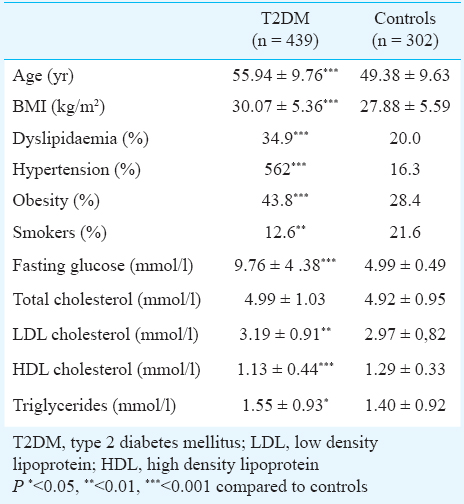
The clinical characteristics of the study population are shown in Table I. There was significant differences for age (P<0.001), and BMI (P<0.001), and the frequencies of dyslipidaemia (P<0.001), hypertension (P<0.001) and cigarette smoking (P<0.01) between T2DM and control groups. The baseline TG (P<0.05) and LDL-C concentrations were higher in the T2DM patients (P<0.01). In addition, T2DM patients presented lower HDL-C levels (P<0.001). The genotype distribution and the relative allele frequency of the FokI polymorphism at the VDR gene in T2DM patients and controls are shown in Table II. Genotype frequencies did not deviate from the Hardy-Weinberg equilibrium in control individuals and T2D patients. The frequencies of the CC, CT and TT genotypes among control group were 55.6, 38.7, and 5.6 per cent, respectively whereas the corresponding frequencies among the patients were 52.6, 41.0 and 6.4 per cent, respectively.
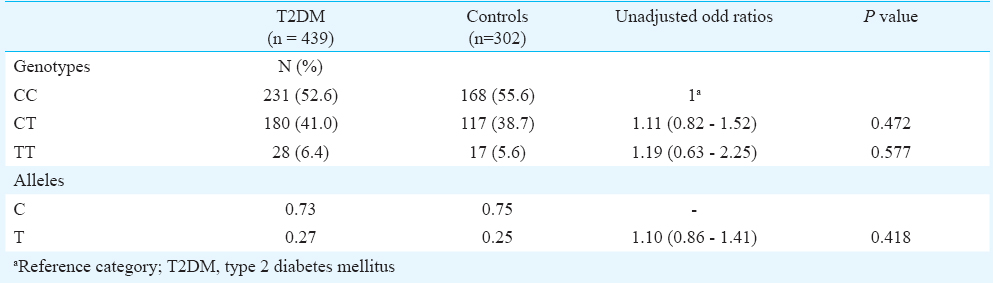
No significant difference in polymorphism, genotype distribution and allele frequency was observed between patients and controls (Table II). When the samples were subgrouped by gender, no significant association was noted between T2DM patients and the controls (data not shown).
Discussion
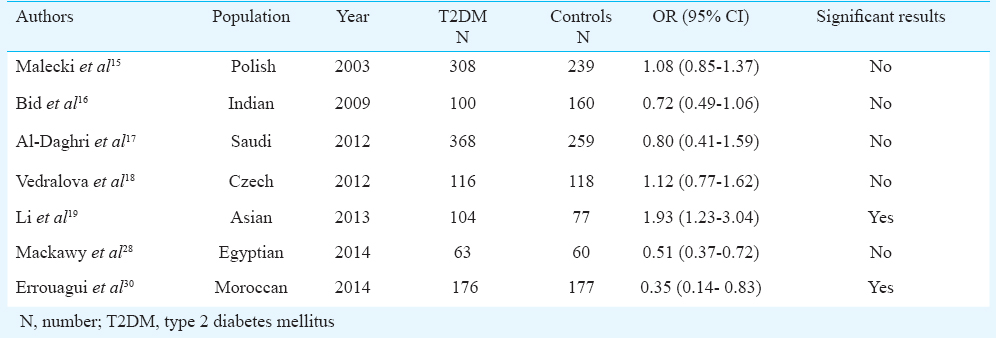
Type 2 diabetes mellitus is a complex disease caused by complex interplay between environmental and genetic factors. Vitamin D is essential for the function of the endocrine pancreas, and the VDR gene may be involved in the pathogenesis and progression of T2DM. Several studies have examined the association of various VDR genetic variants and T2DM, and the results are inconsistent2627. Our data showed that the FokI VDR polymorphism was not associated with T2DM in Tunisian population. The T allele frequency of FokI VDR polymorphism was similar between T2DM and control subjects. The FokI polymorphism, either singly or in combination with other VDR polymorphisms, has been investigated in a few studies on diabetes risk assessment and results were controversial (Table III). Bid et al16 using FokI, BsmI, and TaqI demonstrated that there was no link between polymorphisms in the VDR gene and T2DM. Malecki et al15 reported no significant difference in the distribution of the allele and genotype frequencies of the FokI polymorphism between 308 T2DM patients and 239 healthy controls from Poland similar to our study. However, in an Egyptian study, involving 63 patients with T2DM and 60 controls, the FokI variant was significantly associated with risk of T2DM only in patients with metabolic syndrome28. A meta-analysis of 10 studies involving 1562 cases and 1461 controls, showed that the FokI polymorphism was associated with an increased risk of T2DM (T vs. C: OR = 1.30, 95% CI = 1.17 - 1.45, P<0.001), especially in East Asians14. This was confirmed in another meta-analysis including five studies (1101 cases and 969 controls) of Li et al19, which showed that allele T and variant homozygote TT of FokI variant were significantly associated with T2DM, especially in an Asian population (T vs. C: OR = 1.25, 95% CI = 1.10 - 1.41; TT vs. CC: OR = 1.48, 95% CI = 1.13 - 1.94). A meta-analysis by Yu et al30 including 12 studies showed significant associations of FokI polymorphism with T2DM for three genetic models (TT vs. CC: OR = 1.57, 95% CI = 1.28 - 1.93, P<0.001; CT vs. CC: OR = 1. 54, 95% CI = 1.31 - 1.81, P<0.001; TT + CT vs. CC: OR = 1.57, 95% CI = 1.35 - 1.83, P<0.001), especially in Chinese population. On the other hand, a protective effect of the FokI T allele against T2DM was reported by Errouagui et al29 in a case-control study involving 176 patients with T2DM and 177 healthy controls subjects (OR = 0.35, 95% CI = 0.14 - 0. 83, P=0.018) in Moroccan population.
The discrepancies between the studies may be explained by the different allelic frequencies observed in different ethnic groups. For example, the C allele frequency was lower in Africans when compared to Caucasians and Asians9. Other explanation for the diversity of the results are selection criteria adopted for patients and controls, in particular age, ethnicity, extent of disease, concomitant environmental risk factors like differences in the lifestyles (smoking, diet and physical activity) and the gene-gene and gene-environment interactions.
The present study had some limitations. First, the small size of patients and controls groups which may limit the power (60%) to detect the FokI polymorphism effect on T2DM. Second, our results were limited by the absence of both dietary information and plasma vitamin D concentrations for our study participants. Studies have shown that the association between VDR polymorphisms and disease can vary by either past sun exposure or vitamin D level31. Our study was based on estimates without adjusting for sun exposure or vitamin D intake. Third, polymorphisms of other VDR genotypes, i.e., TaqI, ApaI, and BsmI, and their possible interactions with FokI variants were not evaluated.
In conclusion, our study indicated that the FokI variant of the VDR gene was not associated with T2DM in the Tunisian population. It is possible that the effect of FokI variant on T2DM risk is specific to some particular ethnic populations. The present results require confirmation in further and larger studies in the Tunisian population.
Acknowledgment
This work was supported by a grant from the “Ministry of Higher Education and Scientific Research” of Tunisia.
Conflicts of Interest: None.
References
- Genetics of non-insulin-dependent (type II) diabetes mellitus. Ann Rev Med. 1996;47:509-31.
- [Google Scholar]
- The involvement of microRNAs in type 2 diabetes. Biochem Soc Trans. 2010;38:1565-70.
- [Google Scholar]
- An interethnic comparison of the distribution of vitamin D receptor genotypes and haplotypes. Clin Chim Acta. 2007;384:155-9.
- [Google Scholar]
- Is vitamin D status a determining factor for metabolic syndrome. A case-control study? Diabetes Metab Syndr Obes. 2011;2:205-11.
- [Google Scholar]
- The human vitamin D receptor gene (VDR) is localized to region 12cen-q12 by fluorescent in situ hybridation and radiation hybrid mapping: Genetic and physical VDR map. J Bone Mineral Res. 1999;14:1163-6.
- [Google Scholar]
- Molecular epidemiology of vitamin D receptor gene variants. Epidemiol Rev. 2000;22:203-17.
- [Google Scholar]
- A vitamin D receptor gene polymorphism in the translation initiation codon: effect on protein activity and relation to bone mineral density in Japanese women. J Bone Miner Res. 1997;12:915-21.
- [Google Scholar]
- Comparative high-resolution analysis of linkage disequilibrium and tag single nucleotide polymorphisms between populations in the vitamin D receptor gene. Hum Mol Genet. 2004;13:1633-9.
- [Google Scholar]
- Vitamin D endocrine system and the genetic susceptibility to diabetes, obesity and vascular disease. A review of evidence. Diabetes Metab. 2005;31:318-25.
- [Google Scholar]
- The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2007;92:2017-29.
- [Google Scholar]
- Quantitative assessment of the associations between four polymorphisms (FokI, ApaI, BsmI, TaqI) of vitamin D receptor gene and risk of diabetes mellitus. Mol Biol Rep. 2012;39:9405-14.
- [Google Scholar]
- Viamin D receptor gene polymorphisms and association with type 2 diabetes mellitus in a polish population. Exp Clin Endocrinol Diabetes. 2003;111:505-9.
- [Google Scholar]
- Vitamin D receptor (FokI, BsmI, and TaqI) gene polymorphisms and type 2 diabetes mellitus: A North Indian study. Indian J Med Sci. 2009;63:187-94.
- [Google Scholar]
- Vitamin D receptor gene polymorphisms and HLA DRB1*4 cosegregation in Saudi type 2 diabetes Patients. J Immunol. 2012;188:1325-32.
- [Google Scholar]
- Polymorphisms in the vitamin D receptor gene and parathyroid hormone gene in the development and progression of diabetes mellitus and its chronic complications, diabetic nephropathy and non-diabetic renal disease. Kidney Blood Press Res. 2012;36:1-9.
- [Google Scholar]
- Vitamin D receptor gene polymorphisms and type 2 diabetes: A meta-analysis. Arch Med Res. 2013;44:235-41.
- [Google Scholar]
- Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabet Med. 1998;15:539-53.
- [Google Scholar]
- World Health Organization. Physical status: the use and interpretation anthropometry: Report of a WHO Expert Committee, WHO Technical Report Series, no. 854. Geneva: WHO; 1995. p. :321-44.
- Adult cigarette smoking and exposure to other's smoke. In: Craig R, Shelton N, eds. Health lifestyles: knowledge, attitudes and behaviour. London: NHS Information Centre for Health and Social Care; 2008. p. :149-76.
- [Google Scholar]
- Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499-502.
- [Google Scholar]
- Dupont B, ed. Standardized Southern blot workshop techniques. Histocompatibility testing. New York: Springer; 1987. p. :587-90.
- Association of FokI and BsmI polymorphisms in vitamin D receptor gene with susceptibility to rheumatoid arthritis and Behçet's disease in the Tunisian population. Rev Rumathol. 2012;79:132-6.
- [Google Scholar]
- Vitamin D receptor polymorphisms in type 2 diabetes in Southeastern Iranian patients. Lab Med. 2011;42:32-5.
- [Google Scholar]
- Association of vitamin D receptor gene G>T and T>C polymorphisms in young onset diabetes mellitus in a Bangladeshi population. J Mol Pathophysiol. 2013;2:33-7.
- [Google Scholar]
- Association of vitamin D and vitamin D receptor gene polymorphisms with chronic inflammation, insulin resistance and metabolic syndrome components in type 2 diabetic Egyptian patients. Meta Gene. 2014;2:540-56.
- [Google Scholar]
- Vitamin D receptor gene polymorphisms and vitamin D status and susceptibility to type 2 diabetes mellitus in Moroccans patients. Int J Sci Res Pub. 2014;4:1-8.
- [Google Scholar]
- Association of vitamin D receptor gene polymorphism with the risk of type 2 diabetes mellitus: an update meta-analysis. Nutr Diabetes Complications. 2013;11:213-26.
- [Google Scholar]
- Daily consumption of vitamin D- or vitamin D + calcium-fortified yogurt drink improved glycaemic control in patients with type 2 diabetes: a randomized clinical trial. Am J Clin Nutr. 2011;93:764-71.
- [Google Scholar]




