
Translate this page into:
Klebsiella pneumoniae with pathological intercostal lung herniation
*For correspondence: drmadhusmita1@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 45 yr old male†, non-smoker, with chronic renal disease stage V and type II diabetes mellitus presented to the Pulmonary Medicine department of Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER), Puducherry, India, with cough, foul-smelling reddish expectoration and intermittent fever for one month. He had a bulge with positive cough impulse on the right infraclavicular chest wall (Video) . On examination, the patient was afebrile and non-toxic. Chest wall swelling (Figure A) was irregular, 4 cm × 4 cm, boggy, mildly tender with positive cough impulse, no bruit or crepitus, no local rise of temperature and absent breath sounds on auscultation. His total leucocyte count was 10,400 cells/μl. Sputum sputum culture for acid-fast bacilli and fungus was negative, but positive for Klebsiella pneumoniae. Chest X-ray (Figure B) and plain computed tomography (CT) thorax with Valsalva manoeuvre (Figure C) showed necrotizing consolidation, rib erosion, loss of muscular plane with thick organized pus in the right anterior chest wall. Culture of bronchoalveolar wash and CT-guided aspirated thick pus confirmed K. pneumoniae. Gram staining of sputum yielded Gram-negative bacilli in chains (Figure D). Sputum culture showed pink lactose fermenting colonies of K. pneumoniae (Figure E). The patient was referred to the Cardiothoracic Surgery department where the right upper lobe lobectomy, decortication and resection of the 2nd and 3rd osteomyelitic ribs were done. Histopathology of the excised specimen showed acute necrotizing inflammation with no evidence of granuloma or malignancy. The patient came for follow up after two weeks with improvement in symptoms.
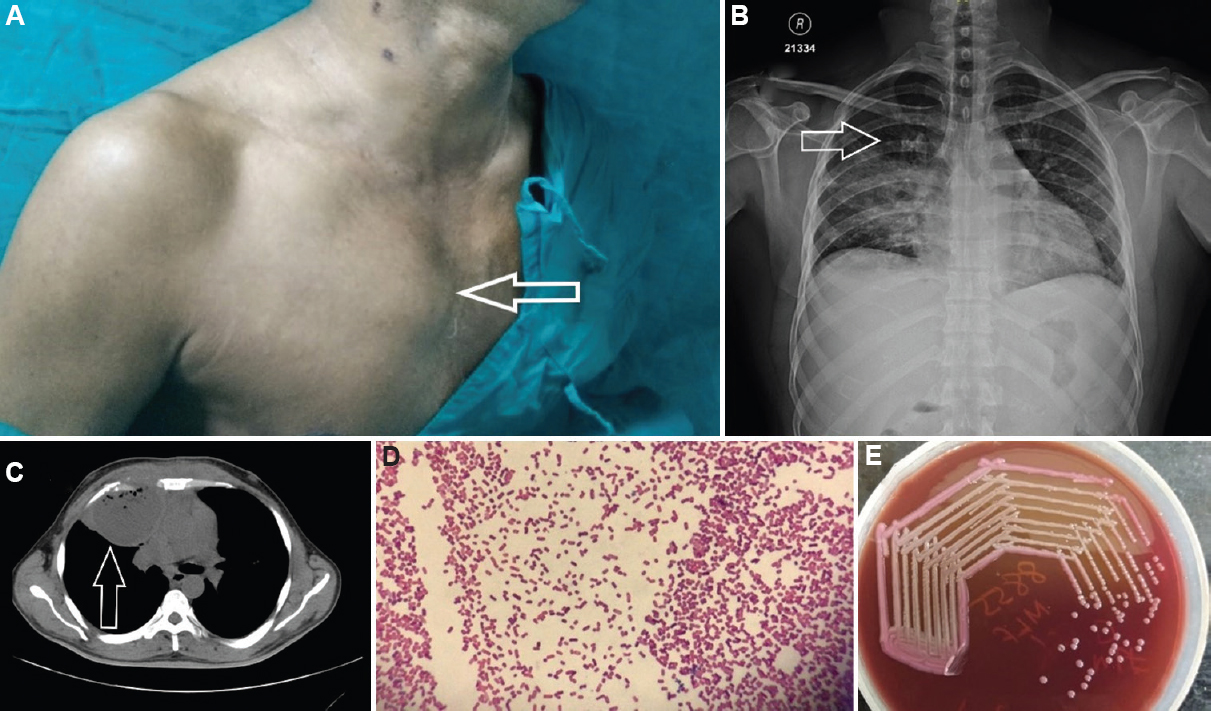
- (A) Right-sided chest wall swelling (arrow). (B) Chest X-ray showing right upper lobe consolidation with cavitation (arrow). (C) Computed tomography scan thorax showing right-sided empyema with rib erosion (arrow). (D) Gram staining of sputum under ×100 magnification shows Gram-negative bacilli in chains. (E) Sputum culture done in MacConkey agar shows pink lactose fermenting colonies of Klebsiella pneumoniae.
 Video available at ijmr.org.in
Video available at ijmr.org.in
Acknowledgment
Authors acknowledge Dr Subathra Adithan, Department of Radiodiagnosis, JIPMER, Puducherry, for her advice for the interpretation of the radiological signs.
Conflicts of Interest: None.




