
Translate this page into:
Intralesional zoledronate: A novel therapy to treat fibrous dysplasia
*For correspondence: bhadadask@rediffmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 10 yr old male child† presented to the Endocrinology Department, Postgraduate Institute of Medical Education & Research (PGIMER), Chandigarh, India, in June 2018, with progressive deformity and pain in the right leg. Examination revealed thickened, deformed, irregular right tibial diaphysis. Pain score, assessed using the subjective numeric pain rating scale, was 8/10. Plain radiographs (Figure A), magnetic resonance imaging and right tibial biopsy with histopathology were suggestive of fibrous dysplasia (FD). Skeletal scintigraphy negated polyostotic involvement. The boy was treated with intralesional zoledronate (0.025 mg/kg). A Jamshidi needle was inserted into the right tibial shaft (Figure B); the trocar was removed and the drug mixed with radiopaque contrast medium was injected slowly under C-arm fluoroscopy guidance (Figure C). There were no intra- or post-procedural complications. When followed up in November 2019, there was no progression of deformity and pain scores had markedly improved to 2/10.
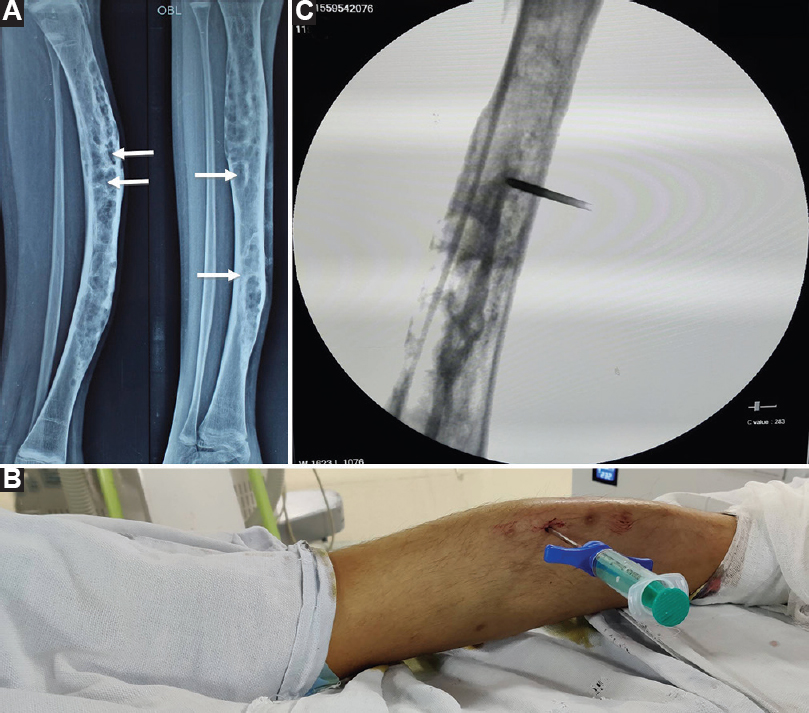
- (A) Plain radiograph (lateral and oblique views) showing deformed right tibia with multiple lytic sclerotic lesions (arrows) giving a ground-glass appearance suggestive of fibrous dysplasia. (B) Photograph showing Jamshidi needle inserted into the right leg. The right leg looks deformed. (C) Fluoroscopy image showing flow of zoledronate mixed with radio-opaque contrast into the right tibia.
The efficacy of systemic bisphosphonates in FD is limited with minimal functional improvement and pain relief. However, intralesional bisphosphonates lead to greater local concentration of drug. This ensures a profound suppression of osteoclasts lining the FD lesions, thereby reducing dysplastic bone turnover and improving pain and physical functioning. Intralesional zoledronate will minimize systemic side effects and simultaneously reduce dosing frequency, and hence economically viable.
Acknowledgment:
Authors acknowledge Dr Rimesh Pal, department of Endocrinology, PGIMER, Chandigarh, in helping us draft the manuscript.
Conflicts of Interest: None.




