
Translate this page into:
Ileo-ureteric with Ileo-uterine fistula: Double trouble
*For correspondence: drvarshney09@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 62 year old female† presented in the department of Surgical Gastroenterology, All India Institute of Medical Sciences, Jodhpur, India in February 2018, with complaints of feculent discharge per vagina and pneumaturia since one month. She had no history of tuberculosis (TB) and was taking analgesics with steroids for polyarthropathy. Computed tomography reported a thick walled loculated collection (~5.5 x 3.5cm) in right adnexal region communicating with the uterus and ileum (Fig. 1A). Right distal ureter was communicating with this collection with moderate hydroureteronephrosis (Fig. 1B-D). There were no features of TB seen on imaging.
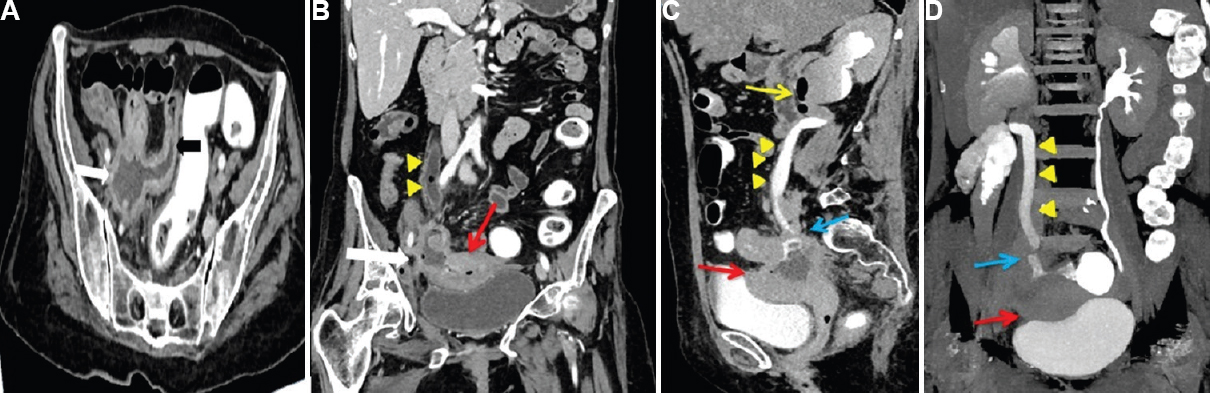
- (A) Computed Tomography image with rectal contrast showing a collection in right adnexal region (white arrow) communicating with terminal ileum (black arrow); (B) Coronal reformat shows dilated right ureter (yellow arrowheads) with air foci in it. Ileal fistula (white arrow) with uterus (red arrow) is also noted along with air foci in endometrial cavity; (C and D) Delayed imaging showed dilated, contrast filled right ureter (yellow arrowheads) with hydronephrosis and air foci in renal pelvis and upper ureter (yellow arrow). Ileo-ureteric fistula (blue arrow) is seen posterior to uterus (red arrow).
Percutaneous nephrostomy was performed to drain the infected right kidney. Exploratory laparotomy revealed adherent terminal ileum to the uterus (Fig. 2A). After dismantling, stricture with perforation was noted in ileum, which was resected and ileo-ascending anastomosis was done. Hysterectomy with bilateral salpingo-oophorectomy was performed and boari flap of urinary bladder was created to anastomose with ureter (Fig. 2B-D). Histopathology (HP) of ileum suggested non-specific chronic ileitis and typhilitis with reactive lymphoid proliferation. HP of uterus and resected ureter also revealed chronic inflammation with no evidence of TB or malignancy.
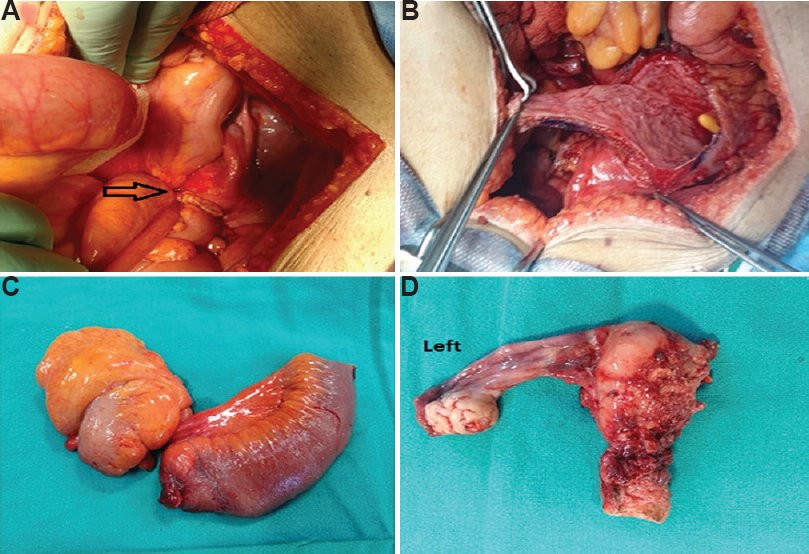
- Intra-operative images: (A) Densely adherent ileum to posterior wall of uterus; (B) Boari's flap being created to bridge the distal ureter; (C) Resected terminal ileum with narrowing and perforation noted; (D) Left salpingo-oophorectomy with hysterectomy specimen with involved posterior surface (right adnexa completely ruined by the disease process).
To summarise, a silent ileal perforation secondary to chronic use of analgesic and steroids led to a pelvic abscess that eroded into the ureter and uterus leading to a complex fistula.




