
Translate this page into:
IgG4-related disease: A missed cause of hypereosinophilia
*For correspondence: doctoranimeshray@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 44 yr old male† presented to the department of Medicine, All India Institute of Medical Science, New Delhi, in December 2018, for evaluation of his previously diagnosed chronic kidney disease. Investigations revealed anaemia with hypereosinophilia (absolute eosinophil count = 2030 cells/mm3) with bilateral shrunken kidney and eosinophils in urine. After ruling out common causes of eosinophilia, a bone marrow biopsy was done. This showed increased eosinophilic precursors with no abnormal cells (Figure A). Mutations (BCR-ABL-1, FIP1L1/PDGFRα fusion mutation, PDGFRβ, FGFR1) and interleukin (IL)-5 levels were negative. A positron emission tomography-computed tomography showed an fluorodeoxyglucose (FDG)-avid retroperitoneal mass (Figure B and C). Biopsy revealed obliterative phlebitis, fibrosis, lymphoplasmacytic and eosinophilic infiltrate (Figure D). Immunohistochemistry stained positive for IgG4 plasma cells (Figure E), and serum IgG4 level was elevated with low serum C3 level. A diagnosis of IgG4-related disease with tubulointerstitial nephritis was made. He was started on 0.5 mg/kg of prednisolone with maintenance haemodialysis but was lost to follow up after discharge. This case highlights IgG4-related disease as an uncommon aetiology in a patient presenting with hypereosinophilia.
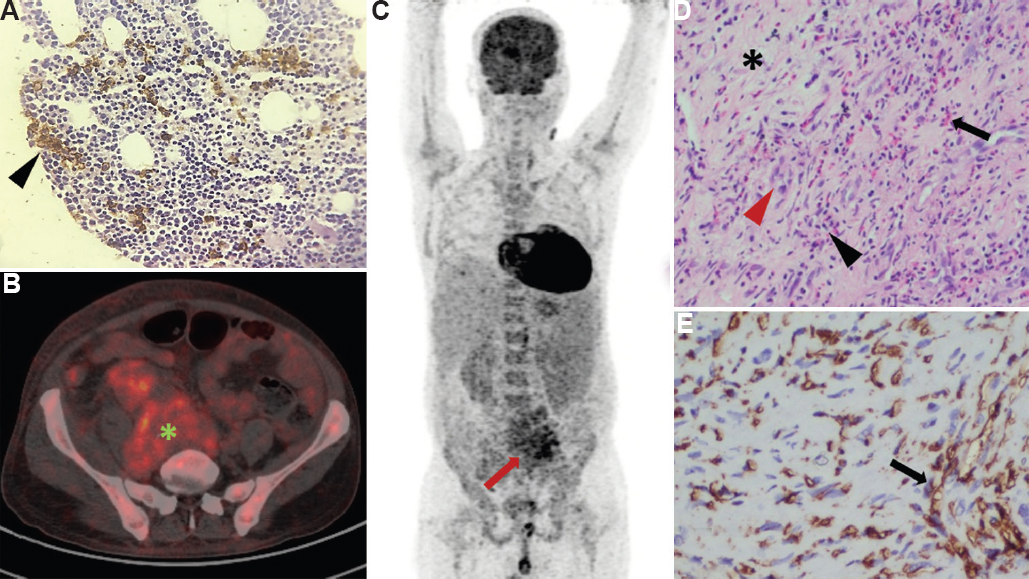
- (A) Bone marrow immunohistochemistry showing eosinophilic precursors with no abnormal cells (black arrowhead). (B) Cross-section of positron emission tomography-computed tomography (PET-CT) showing FDG-avid irregular retroperitoneal mass (green asterisk). (C) Maximum intensity projection of PET-CT showing FDG-avid retroperitoneal mass (red arrow). (D) Histopathology of the retroperitoneal mass showing fibrosis (black asterisk), obliterative phlebitis (red arrowhead), lymphoplasmacytic (black arrowhead) and eosinophilic infiltrate (black arrow). (E) Immunohistochemistry of the biopsy showing IgG4-positive plasma cells staining brown (black arrow).
Conflicts of Interest: None.




