
Translate this page into:
Hypermetabolic pseudotumour of the chest wall
*For correspondence: yaser_ali_kamal@yahoo.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 65 yr old woman† was referred to the department of Cardiothoracic Surgery, Minia University, El-Minya, Egypt, from the departments of Oncology and Radiology at the same institution, in February 2018. The patient had a two-month history of upper back pain associated with right infrascapular swelling and pain on shoulder mobilization. The swelling was not tender or adherent to the underlying structures. On computed tomography (CT), there was poorly-defined right subscapular isodense soft-tissue mass (Fig. 1A). Tissue-guided biopsy was performed and recommended larger sample. On magnetic resonance imaging (MRI), the heterogeneous mass (5 cm×2 cm in axial dimensions) located below the latissimus dorsi muscle, with hypo-intense signal on all pulse sequences and interlacing strands of fat (Fig. 1B). As there were subcentimetric reactive-looking lymph nodes on MRI, fused positron emission tomography (PET)-CT was performed and showed low-level fluorodeoxyglucose (FDG) uptake by the mass (Fig. 1C). The combination of classic symptoms, typical location, appearance on CT and MRI, and absence of the features of soft tissue sarcoma on biopsy increased the suspicion of elastofibroma dorsi (ED). Awareness of this benign hypermetabolic pseudotumour with slight FDG uptake could prevent unnecessary excessive resection. Therefore, marginal excision was decided. The excised specimen was non-encapsulated, irregular and rubbery (Fig. 2A). Microscopically, ED was composed of elastic fibres admixed with mature adipose and fibrous tissues (Fig. 2B). The post-operative course and follow up period of one year were uneventful.
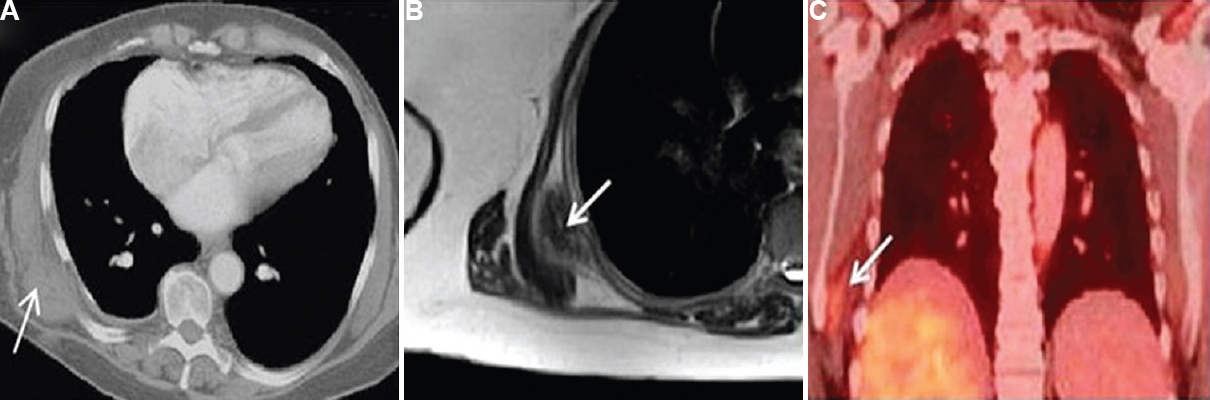
- (A) Axial view chest computed tomography (CT) showing a right-sided subscapular isodense soft-tissue mass (arrow). (B) Axial view of T2-weighted magnetic resonance imaging (MRI) image showing a heterogeneous hypointense signal interlaced with strands of fat (arrow). (C) Fused positron emission tomography (PET)-CT showing low-level fluorodeoxyglucose uptake less than that of the liver (arrow).
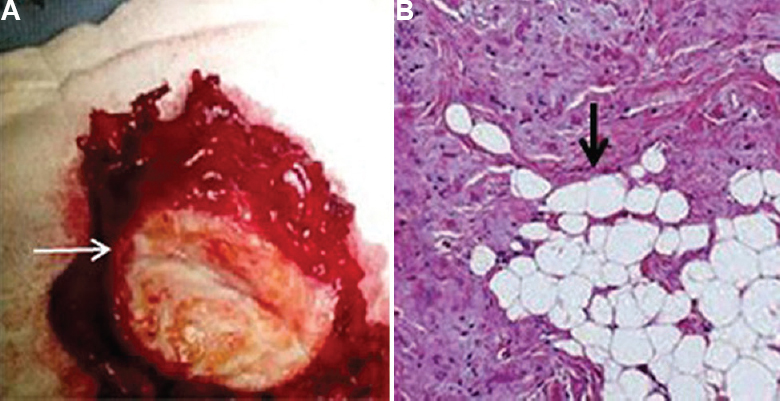
- (A) Grossly, the excised elastofibroma dorsi was irregular rubbery (white arrow), and non-capsulated. (B) Microscopically (H and E, ×100), elastin fibres admixed with fibrous tissue and mature fatty cells (black arrow).
Conflicts of Interest: None.




