
Translate this page into:
Health-related quality of life in Indian children: A community-based cross-sectional survey
Reprint requests: Dr. Manu Raj, Department of Pediatric Cardiology & Public Health Research, Amrita Institute of Medical Sciences & Research Centre, Kochi 682 041, Kerala, India e-mail: drmanuraj@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
There are limited data on health-related quality of life (HRQOL) related to Indian children. The objective of this study was to construct a generic HRQOL reference for children aged 2-18 yr from a community setting.
Methods:
The study was a community-based cross-sectional survey. A total of 719 children/adolescents in the age group of 2-18 yr were enrolled using stratified random cluster sampling. A total of 40 clusters (cluster size 18) were selected for the study. The data contained child self-report and parent proxy report from healthy children and their parents/caretakers. The Pediatric Quality of Life Inventory 4.0 (PedsQL4.0) Generic Core Scale was used to collect HRQOL data. Questionnaires were self-administered for parents and children aged 8-18 yr. In the age group of five to seven years, parents assisted the children in filling questionnaires.
Results:
The mean HRQOL total scores from child self-report and parent proxy report were 87.50±11.10 and 90.10±9.50 respectively, for children aged 2-18 yr. Social functioning had the highest scores and emotional functioning had the lowest scores for the entire sample and subgroups. The mean values for HRQOL in the current study were significantly different from the reference study for both child (87.39 vs. 83.91, P<0.001) and parent proxy reports (90.03 vs. 82.29, P<0.001) when compared between children aged 2-16 yr.
Interpretation & conclusions:
The study provided reference values for HRQOL in healthy children and adolescents from Kerala, India, that appeared to be different from existing international reference. Similar studies need to be done in different parts of India to generate a country-specific HRQOL reference for Indian children.
Keywords
Adolescents
children
health-related quality of life
Pediatric Quality of Life Inventory

Quality of life (QOL) is a standard concept that conveys an overall sense of well-being and comprises several aspects of happiness and satisfaction with life as a whole1. The concept of health-related QOL (HRQOL) and its determinants has evolved to incorporate those aspects of overall QOL that can be clearly shown to affect health - either physical or mental2. Self-assessed health status is a powerful predictor of future mortality and morbidity3.
Rapid advancements in medicine have revolutionized the care of children with acute as well as chronic medical conditions. Measuring HRQOL in childhood and adolescence is essential to quantify the impact of these illnesses on overall QOL. HRQOL instruments currently available for children and adolescents are multi-dimensional and include the physical, psychological (emotional and cognitive) and social health sub-domains. These instruments generally have a generic module as well as several disease-specific modules. The purpose of a generic module is to enable comparisons across several paediatric chronic conditions and benchmarking with healthy population samples. On the other hand, disease-specific modules enhance measurement sensitivity for health domains appropriate and/or unique to a particular chronic condition45.
Several tools are currently available to measure HRQOL in childhood and adolescence4. The most accepted version for paediatric and adolescent HRQOL is the Pediatric Quality of Life Inventory (PedsQL 4.0) by Varni et al5. The PedsQL 4.0 has a generic core scale and several disease-specific scales including separate versions for cardiac illness, asthma, cancer and rheumatologic disorders. Data on paediatric HRQOL constructed using this tool have been used to evaluate HRQOL across a variety of paediatric illnesses/conditions including asthma, cardiac illness, cancer, cerebral palsy, diabetes, end-stage renal disease, rheumatological disorders and psychiatric illnesses6. These reference data were constructed from children aged 2-18 yr from California, USA, and applied on a global scale. The QOL concept is likely to be influenced by several cultural, societal, religious, ethnic and geographic factors and may be perceived differently by children as well as parents from different populations7891011. In a study done among children from the USA, the mean total HRQOL score mentioned was 83.8 (12.7) while a study among Thalassemia children from Thailand recorded a score of 76.7 (11.4), both from child self-reports78. Another study among Palestinian preschool children from conflict zones found the total HRQOL score to be 62 (16) as per parent report9. All three studies used PedsQL 4.0 to measure HRQOL. HRQOL data from the Indian sub-continent collected using PedsQL from normal and abnormal children are also available. Awasthi et al10 reported a mean HRQOL of 73.8 (10.4) and 75.3 (11.9) for adolescents aged 10-19 yr studying in Hindi and English medium classes, respectively, using self-reports. Banerjee et al11 reported a mean HRQOL of 75.8 (14.9) for self-report and 70.3 (21.2) for the parent proxy report among children aged 8-12 yr. This heterogeneity may in turn distort the benchmarking process by which children/adolescents from a unique population are compared to a single dataset that may not represent them. In this context, there is a need to examine if the reference population nomogram is appropriate for generic as well as disease-specific comparisons of HRQOL for children and adolescents from the Indian subcontinent.
The primary objective of this study was to construct a generic HRQOL reference nomogram for children aged 2-18 yr from a representative community setting in Kerala, India, utilizing the PedsQL 4.0 Generic Core Scales. The secondary objectives were to examine the feasibility and reliability of the generic core scales in the Indian context. The study null hypothesis was that the reference nomogram and the one constructed from study data were not significantly different in terms of means of total HRQOL as measured by parent reports using PedsQL 4.0. PedsQL tool was used for measuring HRQOL because of its high levels of reliability, validity, sensitivity, responsiveness and feasibility121314.
Material & Methods
The study was coordinated by Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala, India. The study period was six months (January-June 2015). A sample of 719 children aged 2-18 yr was selected for the study using multi-stage stratified random cluster sampling method. An expected difference of 4.0 in the parent-reported total HRQOL score from the reference (for ages 2-16 yr together) was hypothesized for the sample size calculation (effect size 0.25)14. We selected an alpha of 0.05 and 0.80 of desired power which provided a sample size of 249. Design effect for cluster sampling was calculated using cluster size (k=18) and intra-class correlation coefficient (ICC, 0.1) giving an inflation factor of 2.7. The design adjusted sample size was 672. The same was adjusted to 720 considering addition of two years (adolescents aged 17 and 18 yr) to provide a broader reference range for the proposed HRQOL nomogram.
A total of 40 clusters (cluster size 18) were selected from a geographical area within 10 km radius from the study site. These clusters were chosen from local self-governing (LSG) units and included 12 Panchayats, three Municipalities and one Corporation. The number of clusters from each LSG was determined using population proportionate to size based on the 2011 Census data15. Children and parents were included in the study as respondents. The study inclusion criteria were (i) children aged 2-18 yr, and (ii) those residing in the selected clusters for more than one year. Children with ongoing acute illness or those with a history of chronic illness in the preceding six months were excluded from the study.
The study personnel visited the households (sequentially from a random starting point) under the randomly selected electoral wards of each LSG (40 clusters from 40 different electoral wards). The tool administrations were conducted within household premises under the supervision of the study personnel. All the clusters were visited by the same team on separate days (one day/cluster). All instructions were given to study respondents by the same study personnel (psychologist) in a standard format during household visits.
The data contained a combination of child self-report and parent proxy report from healthy children and their parents/caretakers. Written informed consent and assent was obtained from study participants before collecting data. The PedsQL 4.0 Generic Core Scale was used to collect data regarding HRQOL. Questionnaires were self-administered for parents and children aged 8-18 yr. In the age group of five to seven years, parents assisted the children in filling the questionnaires. Socio-economic class was determined using modified Kuppuswamy's socio-economic scale (2012)16. The research protocol was approved by the Institutional Review Board.
Study tool: Pediatric Quality of Life Inventory (PedsQL 4.0): The PedsQL 4.0 consists of 23 items in four domains: (i) physical functioning (8 items), (ii) emotional functioning (5 items), (iii) social functioning (5 items), and (iv) school functioning (5 items)12. The tool was available in English. This was translated to Malayalam by the study team. The Malayalam version was back-translated into English by a separate team not exposed to the original English version. The two versions were checked for content validity by a team of experts including a child psychologist, senior paediatrician and a medical social worker. The tool was provided in the local language (Malayalam) for ease of self-administration by study participants.
The PedsQL 4.0 Generic Core Scales comprised parallel child self-report and parent proxy report formats. Child self-report included ages 5-7, 8-12 and 13-18 yr. Parent proxy report included ages 2-4 (toddler), 5-7 (young child), 8-12 (child) and 13-18 (adolescent). A five-point Likert response scale was utilized across child self-report for ages 8-18 yr and parent proxy report. For the child self-report from younger age group (5-7 yr), a three-point pictorial scale was used for ease of self-administration by younger children. Items were reverse-scored and linearly transformed to a 0-100 scale (0=100, 1=75, 2=50, 3=25, 4=0). Scale scores were computed as the sum of the items divided by the number of items answered. A higher score on total score as well as individual components signified better HRQOL12. The six study variables in the study included HRQOL - total score and its sub-domain/summary scores for physical functioning, psychosocial functioning, emotional functioning, social functioning and school functioning.
Statistical analysis: The feasibility of the tool was determined from the percentage of missing values for each item and distribution of item responses. Scale internal consistency reliability was checked by calculating Cronbach's coefficient alpha. The minimal clinically important difference (MCID) for PedsQL 4.0 scale scores was quantified by calculating the standard error of measurement (SEM). Agreement between child self-report and parent proxy report was determined through two-way mixed effect model (absolute agreement, single measure) intra-class correlation coefficients (ICC). Statistical analyses were conducted using SPSS version 20.0 for Windows (IBM Corporation Armonk, NY, USA).
Results
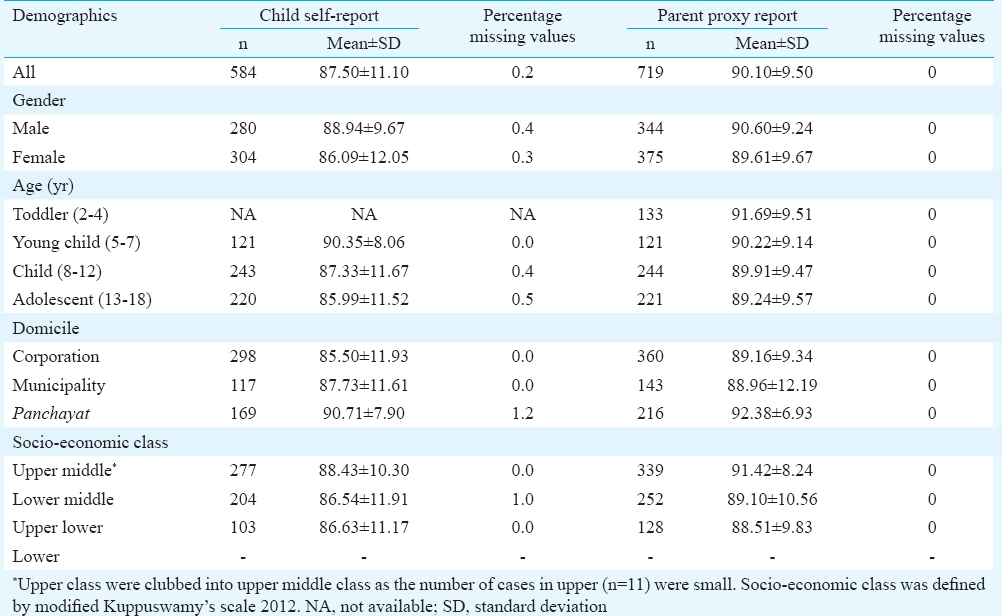
The details of the study population are presented as Table I. A total of 719 children/adolescents in the age group of 2-18 yr (mean age 9.6±4.5 yr) were enrolled from 40 randomly selected clusters. The overall response to the household survey was 99.17 per cent (719 participants enrolled from 725 contacted). Among the participants, 47.8 per cent were males. Among those enrolled, 70 per cent were from urban areas. Approximately 47.1 per cent were from upper middle socio-economic class. The mean HRQOL total scores of the overall sample from child self-report and parent proxy report were 87.50 (11.10) and 90.10 (9.50), respectively.
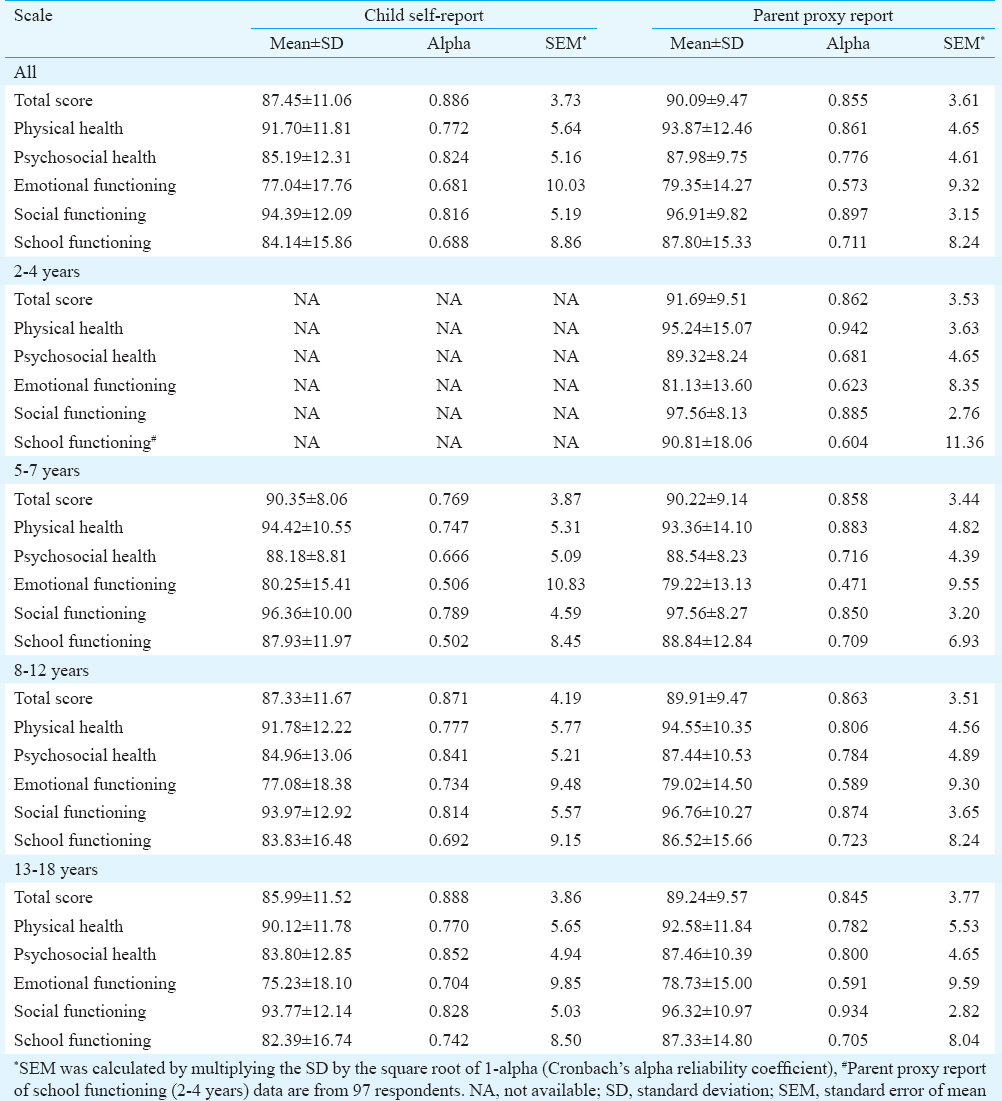
Scale descriptives: The scale descriptives from the study sample are presented in Table II. Among the domains, social functioning had the highest scores and emotional functioning had the lowest scores for the entire sample or age based subgroups. This pattern was similar for both child self-report and parent proxy report.
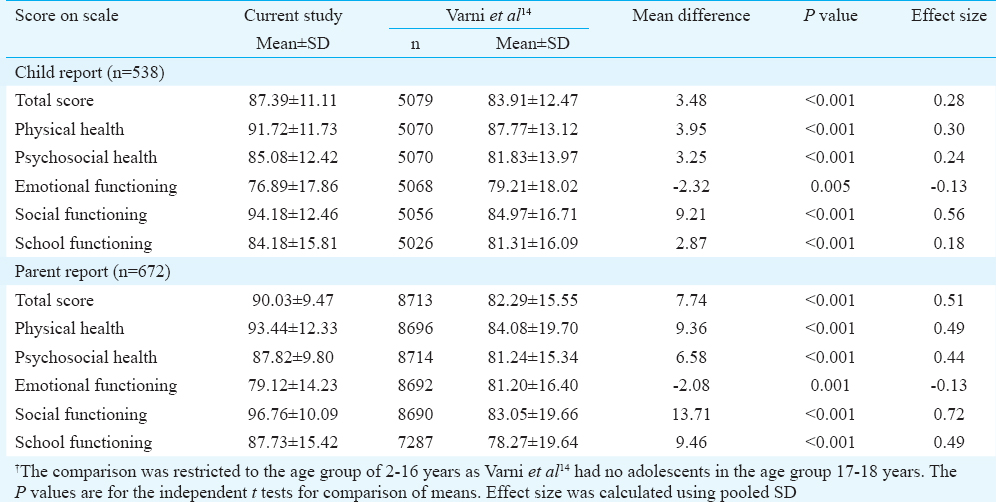
The mean values for total HRQOL score in the current study (age group 2-16 yr) were significantly different from the reference paper by Varni et al12 for both child (87.39 vs. 83.91, P<0.001) and parent proxy reports (90.03 vs. 82.29, P<0.001). This comparison was made after constructing a comparable sample (children aged 2-16 yr only) from the total sample as the reference data were constructed from children aged 2-16 yr. In addition, differences were seen among mean scores for physical health, psychosocial health, emotional functioning, social functioning and school functioning in both child and parent reports between the two studies on age appropriate comparisons. The details are presented in Table III.
Internal consistency reliability: The internal consistency reliability for the total HRQOL score was 0.89 for child form and 0.86 for parent form (Table II). Overall, the sample showed good internal consistency reliability (Cronbach's alpha >0.7) across domains for both child and parent reports, except for emotional functioning (child & parent forms) and school functioning in child form. When the scores were stratified for age, both emotional functioning and school functioning showed lower internal consistency among the domains. This pattern was seen for both child and parent forms across all age groups.
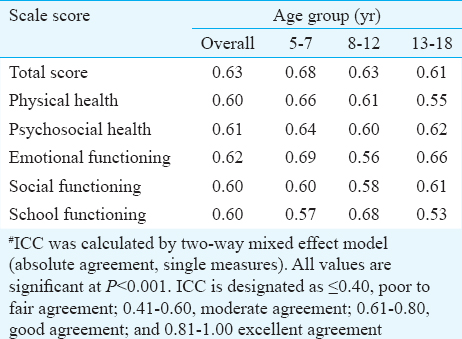
Parent-child agreement in HRQOL reporting: The agreements between the parent/caretaker and the child in reporting HRQOL total as well as sub-scores were examined by ICC (two-way mixed effects). There was a good agreement (ICC 0.61-0.80) between the two groups for all HRQOL domains in the five to seven years age group, except for school functioning. In the 8-12 yr age group, good agreement was seen in all HRQOL domains, except emotional and social functioning. In the 13-18 yr age group, the same was seen except for physical health and school functioning. Overall, all age groups exhibited moderate to fair agreement between child and parent reports in all the HRQOL domains. The details are available in Table IV.
Subgroup comparisons: Total score as well as scores of individual domains were compared across subgroups based on age, sex, area of domicile and socio-economic status (SES) levels. Younger children (5-7 yr) reported significantly higher HRQOL total scores as compared to both older children (8-12 yr) (90.4 vs. 87.3, P=0.042) and adolescents (13-18 yr) (90.4 vs. 86.0, P=0.001). A similar trend was lacking in parent proxy report. In the sub-domains, younger children reported higher HRQOL scores than adolescents for physical health (94.4 vs. 90.1, P=0.004), psychosocial health (88.2 vs. 83.8, P=0.005), emotional functioning (80.2 vs. 75.2, P=0.037) and school functioning (87.9 vs. 82.4, P=0.006) (data not shown).
Male children reported significantly higher HRQOL scores than females in terms of total score (88.9 vs. 86.1, P=0.002) as well as physical health (93.3 vs. 90.3, P=0.002), psychosocial health (86.6 vs. 83.9, P=0.007) and emotional functioning (79.9 vs. 74.5, P<0.001) as compared to females. On the contrary, parent proxy reports did not demonstrate any significant sex-based differences for HRQOL.
The data was also analyzed based on rural (child report, n=169; parent report, n=216) or urban (child report, n=415; parent report, n=503) domicile. Rural children (90.7 vs. 86.1, P<0.001) and their parents (92.4 vs 89.1, P<0.001) reported higher total HRQOL scores compared to their urban counterparts. Similar trends were seen for sub-domains, except for emotional functioning in parent proxy report. Children did not report any significant differences in HRQOL scores across SES groups. On the contrary, parents reported significant differences (P<0.05 - 0.001) for HRQOL scores (total as well as individual domains) between SES groups, except for social functioning domain score.
Discussion
The current study provides data on HRQOL of normal children and adolescents in both direct and proxy report formats. The study also enables an age appropriate comparison of HRQOL between children/adolescents in the US and their counterparts from Kerala, India. In addition, it also provides several subgroup stratified total HRQOL scores that enabled detailed inter-group comparisons.
The comparison of HRQOL scores (total, summary as well as sub-domains) between the reference study and the current study showed a significant difference between HRQOL scores between the two populations. All HRQOL scores were significantly higher for children/adolescents from the current study as compared to their US counterparts, except for emotional functioning12. The wide range for mean differences (-2.08 to 13.71) as well as their corresponding effect sizes (-0.13 to 0.72) suggests that HRQOL reference values for children/adolescents need to be derived from respective populations that share ethnic, cultural and socio-economic scenarios. In addition, the MCID as denoted by the corresponding SEM values is lower for study children compared to US children, except for emotional functioning12. It appears more appropriate and logical to use MCID values from the same population for clinical decisions and therapeutic strategies, rather than an external reference.
There are several methodological differences between the two studies that can contribute to the observed differences. The sample selection was uninsured population in reference study versus all inclusive population in the current study. There was a significant difference in response rate for enrolment between the reference and the current study (51 vs. 99%). The type of data collection was also different between the two studies (mailed questionnaire vs. home visits). Other probable reasons for this observed difference may be period of study (2001 vs. 2015), language of administration (five different languages vs. one) and ethnicity (multi-ethnic vs. single ethnic).
The study results suggested that the PedsQL 4.0 has good feasibility and reasonable reliability for both child and parent proxy reports among Indian children across all HRQOL scores. Among the sub-domains, emotional functioning showed lower reliability in the current study. The reliability parameters of the current study were similar to those published by Varni et al12.
The child versus parent report agreement levels in the current study as assessed by ICC were comparable with those reported by Varni et al1417. A review on parent-child agreement across paediatric HRQOL instruments concludes that the clinical significance of actual difference between child and parent reporting of HRQOL is unclear18. The review states two prominent reasons - either a lack of parental knowledge concerning children's experiences and beliefs or a difference in the perspective of self and others. It also adds that parents may vary in their awareness, sensitivity and tolerance of children's health concerns18. The same reasons may have played a role in the differential reporting of HRQOL by children and parents in the current study.
In our study younger children reported better HRQOL scores as compared to older children. This age trend was similar to the findings of a previous review that covered 37 studies related to self-report QOL among children and adolescents19. No such trend was visible among parent proxy reports in the current study as well as in the review reported earlier19.
The current study data were compared with HRQOL data from developing countries such as China and Brazil2021. The data from China showed a pattern similar to that of our study. Both studies showed maximum score for social functioning and minimum score for emotional functioning. The same pattern was seen in both child and parent reports. On the contrary, the data from Brazil showed a pattern similar to that of Varni et al14. Both Brazilian and US data showed maximum scores for physical health (for both child and parent forms) contrary to the current study and the study from China. The lowest scores for the US, as well as Brazilian data were for emotional functioning as per both child and parent forms, similar to the current study and the study from China142021.
Sex-based differences noted in the current study for HRQOL total as well as several sub-domain-based scores were in agreement with previously published studies from other countries2223. A study from Estonia reported that female adolescents had significantly lower total HRQOL values as well as for physical health, emotional functioning and psychosocial health domains compared to their male counterparts22. On the contrary, sex difference was noted only for emotional functioning sub-scale in one Norwegian study23. This finding was restricted to direct (child) reports and not in proxy (parent) reports for HRQOL in the current study.
The fact that rural children from low-resource settings as well as their parents reported better HRQOL than their urban counterparts is an interesting observation in the domain of HRQOL research. This rural-urban differential in HRQOL visible in both forms of reporting could probably be due to differences in perception and/or expectations about QOL as well as life amenities between the rural and urban populations.
Our study had good response rate for enrolment that minimized selection bias. The study represented both rural and urban population and covered multiple socio-economic levels for better generalizability. The age structure of the study sample was comparable to that available from Census 2011 adding to the generalizability of the findings to the base population. However, there were a few limitations. The cross-sectional study design, single-point measurement and subjective nature of the HRQOL measurements might have influenced the quality of data collected in the study. Collecting the same data during multiple visits from each respondent on a longitudinal basis would have reduced random error and provided us with better average estimates. This was not attempted due to feasibility issues related to personnel and time available for house visits. The relationship between observed variables of HRQOL and their underlying latent constructs was not examined by a confirmatory factor analysis due to resource limitations.
In conclusion, our study provides reference values for HRQOL in healthy children and adolescents from Kerala, India. This HRQOL nomogram, together with several others from various parts of the country will help researchers in constructing a pooled country-specific HRQOL reference for Indian children. Such an HRQOL reference may assist researchers to adopt them across various paediatric diseases/disorders and to compare the same with HRQOL of their normal counterparts in a contextually appropriate process.
Acknowledgment
The principal study “Psychosocial and economic impact of surgery for congenital heart disease on Indian families” was funded by the Indian Council of Medical Research (ICMR), New Delhi. The current study was a sub-study under this main study.
Conflicts of Interest: None.
References
- 2000. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion. Measuring healthy days: Population assessment of health-related quality of life. Atlanta: Centers for Disease Control and Prevention; Available from: http://www.cdc.gov/hrqol/pdfs/mhd.pdf
- Health status assessment methods for adults: Past accomplishments and future challenges. Annu Rev Public Health. 1999;20:309-35.
- [Google Scholar]
- Self-rated health and mortality: A review of twenty-seven community studies. J Health Soc Behav. 1997;38:21-37.
- [Google Scholar]
- Generic and disease-specific measures in assessing health status and quality of life. Med Care. 1989;27(3 Suppl):S217-32.
- [Google Scholar]
- The PedsQL: Measurement model for the pediatric quality of life inventory. Med Care. 1999;37:126-39.
- [Google Scholar]
- Impaired health-related quality of life in children and adolescents with chronic conditions: A comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQL 4.0 Generic Core Scales. Health Qual Life Outcomes. 2007;5:43.
- [Google Scholar]
- Health-related quality of life of children and adolescents with cerebral palsy: Hearing the voices of the children. Dev Med Child Neurol. 2005;47:592-7.
- [Google Scholar]
- Factors affecting health-related quality of life in Thai children with thalassemia. BMC Blood Disord. 2010;10:1.
- [Google Scholar]
- Health-related quality of life of Palestinian preschoolers in the Gaza Strip: A cross-sectional study. BMC Public Health. 2011;11:253.
- [Google Scholar]
- Assessment of Health-Related Quality of Life in school-going adolescents: Validation of PedsQL instrument and comparison with WHOQOL-BREF. Natl Med J India. 2012;25:74-9.
- [Google Scholar]
- HRQoL in HIV-infected children using PedsQL 4.0 and comparison with uninfected children. Qual Life Res. 2010;19:803-12.
- [Google Scholar]
- PedsQL 4.0: Reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39:800-12.
- [Google Scholar]
- The PedsQL 4.0 Generic Core Scales: Sensitivity, responsiveness, and impact on clinical decision-making. J Behav Med. 2002;25:175-93.
- [Google Scholar]
- The PedsQL 4.0 as a pediatric population health measure: Feasibility, reliability, and validity. Ambul Pediatr. 2003;3:329-41.
- [Google Scholar]
- 2011. Census of India. Available from: http://www.censusindia.gov.in/2011census/dchb/3208_PART_B_ERNAKULAM.pdf
- Kuppuswamy's socioeconomic scale: Updating income ranges for the year 2012. Indian J Public Health. 2012;56:103-4.
- [Google Scholar]
- How young can children reliably and validly self-report their health-related quality of life? an analysis of 8,591 children across age subgroups with the PedsQL 4.0 Generic Core Scales. Health Qual Life Outcomes. 2007;5:1.
- [Google Scholar]
- Parent-child agreement across child health-related quality of life instruments: A review of the literature. Qual Life Res. 2008;17:895-913.
- [Google Scholar]
- Self-reported quality of life of young children with conditions from early infancy: A systematic review. Pediatrics. 2014;134:e1129-48.
- [Google Scholar]
- Measuring health-related quality of life in children with cancer living in Mainland China: Feasibility, reliability and validity of the Chinese Mandarin version of PedsQL 4.0 Generic Core Scales and 3.0. Cancer Module Health Qual Life Outcomes. 2011;9:103.
- [Google Scholar]
- Quality of life of children and adolescents from São Paulo: Reliability and validity of the Brazilian version of the Pediatric Quality of Life Inventory version 4.0 Generic Core Scales. J Pediatr (Rio J). 2008;84:308-15.
- [Google Scholar]
- Health-related quality of life of Estonian adolescents: Reliability and validity of the PedsQL™ 4.0 Generic Core Scales in Estonia. Acta Paediatr. 2011;100:1043-7.
- [Google Scholar]
- Measuring health-related quality of life in young adolescents: Reliability and validity in the Norwegian version of the Pediatric Quality of Life Inventory 4.0 (PedsQL) Generic Core Scales. Health Qual Life Outcomes. 2006;4:61.
- [Google Scholar]




