
Translate this page into:
Growth pattern of skinfold thicknesses in term symmetric & asymmetric small for gestational age infants
For correspondence: Dr Anil Kumar Bhalla, Child Growth & Anthropology Unit, Department of Paediatrics, Postgraduate Institute of Medical Education & Research, Chandigarh 160 012, India e-mail: drakbhallashgp@gmail.com
-
Received: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
A etiologically symmetric and asymmetric small for gestational age (SGA) infants are two distinct entities. In view of absence of longitudinal information on growth pattern of skinfold thicknesses (SFTs) among Indian infants, this study was conducted to assess the auxological dynamics of SFTs (sub-cutaneous fat) of symmetric and asymmetric SGA infants.
Methods:
Triceps, sub-scapular, biceps, mid-axillary and anterior thigh SFTs among full-term, 100 symmetric SGA, 100 asymmetric SGA and 100 appropriate for gestational age (AGA) infants were measured at one, three, six, nine and 12 months. Ponderal Index (PI) was used to categorize infants into symmetric SGA (PI ≥2.2 g/cm3) and asymmetric SGA (PI <2.2 g/cm3). Intra-group (symmetric vs. asymmetric), inter-group (SGA vs. AGA) and gender differences were quantified.
Results:
SFTs among symmetric, asymmetric SGA infants increased to attain peak by six months. Maximum fat deposition in SGA infants was noticed for triceps, minimum for mid-axillary SFT. Mean triceps and sub-scapular skinfolds were measured higher in symmetric SGA than in asymmetric infants. SGA infants had significantly (P≤0.05) thinner SFTs than AGA. Growth velocity for SFTs, among symmetric and asymmetric SGA, was measured maximum between one and three months, threreafter it declined and relatively, steepness of fall was maximum for mid-axillary SFT followed by sub-scapular SFT.
Interpretation & conclusions:
Thinner SFTs obtained for symmetric and asymmetric SGA as compared to AGA infants reveal their compromised adiposity and nutritional status. Comparatively, higher SFTs in symmetric than in asymmetric SGA infants appear to suggest that the former have a tendency to accumulate more fat, than the latter during infancy.
Keywords
Appropriate for gestational age
asymmetric small for gestational age
longitudinal data
skinfold thickness
small for gestational age
sub-cutaneous fat
symmetric small for gestational age

Small for gestational age (SGA) is described as a neonate whose weight at birth is less than 10th percentile for gestational age and sex of the accepted reference standards1. Depending upon timing and severity of insult during antenatal period, SGA is classified into symmetrical and asymmetrical subgroups2. Symmetric and asymmetric SGA infants demonstrate different implications for postnatal growth and quality of survival. Previous studies reveal that children born as SGA accumulate more of sub-cutaneous fat and develop obesity, later345678. Some studies have suggested that SGA infants remain lighter and have less body fat compared to appropriate for gestational age (AGA) infants59. Information on the growth pattern of sub-cutaneous fat of term SGA infants is scarce, except for data provided by Rodriguez et al10 on infants of Spanish origin. In view of the non-availability of longitudinal information on the growth of sub-cutaneous fat of two types of SGA infants, we attempted to study auxological dynamics of triceps, sub-scapular, biceps, mid-axillary, anterior thigh skinfold thicknesses (SFTs) of full-term symmetric SGA, asymmetric SGA as well as AGA infants of Indian origin.
Material & Methods
A total of 200 full-term SGA infants (symmetric SGA: male 50, female 50; asymmetric SGA: male 50, female 50) born consecutively in the labour room of the department of Obstetrics and Gynaecology, Postgraduate Institute of Medical Education & Research, Chandigarh, India, and fulfilling eligibility criteria envisaged sample for this mixed-longitudinal study. The enrolment of infants in the study began in January 2006 and continued until October 2007. In addition, 100 (50 males and 50 females) full-term, AGA infants born during the same time period served as controls. Enrolment of infants in the study was made in the department of Paediatrics, PGIMER, after obtaining informed written consent of either or both of the parents. The study protocol was approved by the Institutional Ethics Committee as well as the Department Review Board.
Infants with birth weight within 10th to 90th percentile of intrauterine growth curves11 were considered as AGA, while those weighing less than 10th percentile as SGA. Ponderal Index (PI) was used to categorize infants into symmetric SGA (PI ≥2.2 g/cm3) and asymmetric SGA (PI <2.2 g/cm3)12. Socio-economic status of the infants was determined using standardized scale13. Of these, 48.6 per cent were from Punjab, 18.3 per cent from Haryana, 13.7 per cent hailed from Himachal Pradesh, 9.8 per cent from Uttar Pradesh, 4.6 per cent represented the Union Territory of Chandigarh, 2.7 per cent were from Gharwal (Uttarakhand) and 2.3 per cent from the State of Rajasthan. Sixty six per cent of AGA and 55 per cent of SGA infants inhabited urban localities, while the remaining resided in rural areas. Neonates with multiple gestation, major congenital/chromosomal/body anomalies or with moderate-to-severe illness (meningitis, septicaemia, bone or joint infections, necrotizing enterocolitis) and on mechanical ventilation were excluded from the study1415.
Each infant was measured for triceps, sub-scapular, biceps, mid-axillary and anterior thigh SFTs using Harpenden’s Skinfold Calliper (Holtain Limited, Crymych, UK, Least count: 0.2 mm) at one month (±3 days), three, six, nine and at 12 months (±15 days) using mixed-longitudinal method of studying human growth. This is defined as a serial study in which a group of children is followed periodically, at fixed time intervals such that some children may leave the study and others, if desired join it at some age points16. All measurements were taken by the trained anthropometrist on pre-appointed date and time. The follow up of the study infants continued up to October 2008. The same calliper was used during the entire period of this study. The magnitude of intra/inter-observer error for all SFTs was ±0.2 mm. Intra-class correlation coefficient and Cronbach’s alpha were applied to see the reliability of inter and intra-observer error for 10 per cent of data, which was found to be ≥0.7.
Infants who missed follow up on appointed dates were contacted through telephone, postal correspondence and were even examined in their homes. The parents of some of these infants who belonged to far-off places had been staying in and around Chandigarh during the study period which permitted their successful time bound follow up. The net sample attrition rate observed for symmetric male and female infants was 5.6 and 2.7 per cent, respectively. Among asymmetric SGA male and female infants, it was four and 6.7 per cent, while in AGA infants, the attrition rate was two per cent in male and 3.7 per cent in female infants. Besides, conducting health examination, dietary intake of each infant at each visit was also recorded using 24 h dietary recall method.
Statistical analysis: The sample size for this serial study was calculated considering 7.7 kg as an average weight for term SGA and 8.1 kg for term AGA infants at one year of age based on the available data1718. To detect a difference of 400 g between mean birth weights, with one tailed α=0.05 and power=95 per cent, the number of infants required per group was 50 (Power and Precision ver2 Biostat, USA). However, assuming 10 per cent sample attrition due to en route mortality, dropouts and loss to follow up, it comes to be 55. We enrolled 100 infants per group (i.e. symmetric SGA, asymmetric SGA and AGA).
Mean and standard deviation (SD) were computed for different SFTs measured among male and female symmetric SGA, asymmetric SGA and AGA infants at each age level. Student’s t test was used to calculate magnitude of intra-group (symmetric vs. asymmetric), inter-group (SGA vs. AGA) and gender differences in the mean growth attainments computed for different SFTs. To assess inter-population comparison between SGA and normal infants, comparison with already published data on normal children by Bhalla et al19 and WHO20 was attempted.
Results
Of the total 200 SGA and 100 AGA infants enrolled in the study, 87 per cent SGA and 85 per cent AGA belonged to upper middle socio-economic status, 10 per cent SGA and 12 per cent AGA were in the high socio-economic status group and only three per cent of each of the SGA and AGA infants belonged to upper high socio-economic status. Breastfeeding among all SGA and AGA infants was initiated within 24 h of birth. By three months, 72 per cent of SGA and 87 per cent of AGA infants were exclusively breastfed. Semi-solid food items were introduced around five months of age in majority of the children. However, mothers of three children did not give semi-solid food items until one year of age, despite repeated advice. A thorough health examination of every infant was carried out. Each infant included in the study was duly immunized as per age. Initially, every infant had feeding difficulties and some had upper respiratory tract infections, mild fever, cold, cough, short-term episodes of diarrhoea and constipation, for which they were treated accordingly.
The mean (SD) computed for triceps, sub-scapular, biceps, mid-axillary and anterior thigh SFTs among symmetric, asymmetric SGA and AGA infants are shown in Figures 1-5. All SFTs uninterruptedly increased from one to six months, except mid-axillary SFT which did so till three months. Triceps, sub-scapular, mid-axillary, biceps and anterior-thigh SFT was measured more in symmetric SGA male infants than their asymmetric counterparts. On the other hand, symmetric SGA female infants possessed fatter triceps, mid-axillary and anterior thigh SFTs than asymmetric infants. In general, male and female AGA infants possessed higher mean triceps, sub-scapular, biceps, mid-axillary and anterior thigh SFTs than symmetric and asymmetric SGA infants, but these differences became significant for triceps and anterior thigh SFTs.
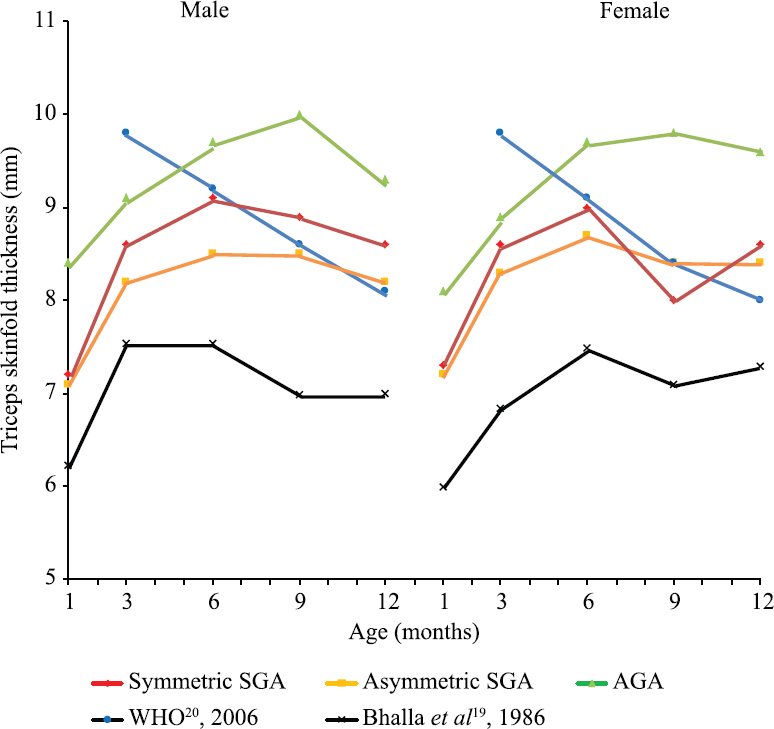
- Comparison of triceps skinfold thickness (mm) of male and female symmetric small for gestational age (SGA), asymmetric SGA and appropriate for gestational age (AGA) and normal infants.

- Comparison of sub-scapular skinfold thickness (mm) of male and female symmetric small for gestational age (SGA), asymmetric SGA and appropriate for gestational age (AGA) and normal infants.

- Comparison of biceps skinfold thickness (mm) of male and female symmetric small for gestational age (SGA), asymmetric SGA and appropriate for gestational age (AGA) and normal infants.

- Comparison of mid-axillary skinfold thickness (mm) of male and female symmetric small for gestational age (SGA), asymmetric SGA and appropriate for gestational age (AGA) and normal infants.

- Comparison of thigh (anterior) skinfold thickness (mm) of male and female symmetric small for gestational age (SGA), asymmetric SGA and appropriate for gestational age (AGA) and normal infants.
As compared to their normal counterparts from Punjab19, our SGA and AGA infants had greater triceps, sub-scapular and mid-axillary SFTs. Triceps and sub-scapular skinfolds in both symmetric and asymmetric SGA infants measured lesser than their MGRS (WHO multicentre growth reference study)20 counterparts during first half of infancy; thereafter, SGA infants possessed more of sub-cutaneous fat.
The male and female symmetric and asymmetric SGA infants had almost similar mean triceps and biceps SFTs. Mean sub-scapular SFT was measured more in female SGA infants of two types than their male counterparts. However, gender differences became significant at three months (P≤0.05) among symmetric and at nine (P≤0.01) and 12 (P≤0.05) months in asymmetric infants. In general, female symmetric and asymmetric SGA infants had fatter anterior thigh SFT than the males. Mid-axillary SFT in male and female symmetric SGA infants did not differ significantly, while it measured significantly (P≤0.05) fatter in female asymmetric SGA infants than males beyond one month of age.
Discussion
The SFTs among all SGA and AGA infants depicted a rapid increase up to three (mid-axillary) and six months (triceps, sub-scapular, biceps, thigh, sum of SFTs) of age to attain a peak before commencing to decline. Attainment of a similar peak at four to six months of life in infants of US origin has also been documented23. Kuzawa24 reported that though born plump, human newborns attain peak adiposity only during early infancy before commencing to decline, which is similar to the trend observed for our sample infants. This shows that infants irrespective of their being born either SGA or AGA have tendency to lose fat from three months onwards until the end of first year of life. Dobbing and Sands25 also proposed that human newborns are fatter than expected because of increased energy requirements.
Symmetric SGA infants had greater deposition of sub-cutaneous fat at triceps, sub-scapular, biceps, mid-axillary and thigh sites than their asymmetric counterparts; however female symmetric SGA infants measured thinner for biceps and mid-axillary SFT than their asymmetric counterparts beyond three months. The relatively more of sub-cutaneous tissue noticed among symmetric SGA infants than the asymmetric ones may be a protective response of these severely affected infants towards their postnatal healthy survival through which they attempt to maintain body temperature. Similar findings on term symmetric and asymmetric SGA infants of Spanish origin10 are in consonance with our results. These authors opined that despite an overall small body size and lesser amount of sub-cutaneous fat than the reference population, symmetric SGA term newborns possessed proportionate body fat distribution, while asymmetric SGA remained thinner with lesser central subcutaneous fat percentage than symmetric SGA. On the contrary, higher triceps and sub-scapular SFT noticed among infants with intrauterine growth retardation having low ponderal index (IUGR-LPI) compared to those with adequate ponderal index (IUGR-API) during the first year of life26 remains at variance with our results. In general, the fatter SFTs noticed among our two types of SGA and AGA female infants than their male counterparts corroborated with the findings of Luque et al27 who also reported lesser deposition of fat among male than female infants.
Symmetric and asymmetric SGA infants possessed significantly thinner SFTs as compared to AGA infants. On the contrary, Hediger et al28 did not notice a significant difference for fat deposited among SGA and AGA infants representing US-born non-Hispanic black, non-Hispanic white and Mexican-American population stocks. Davies29 reported that light-for-date infants accumulated fat at a faster rate as compared to infants who were heavy-for-date. Beltrand et al30 did not find difference in total sub-cutaneous fat among infants of French origin with foetal growth restriction as compared to those without foetal growth restriction. Another study reported catch-up in fat of SGA infants than in weight and height31. Both types of SGA and AGA infants representing present study exhibited a tendency to accumulate more fat in the peripheral (i.e. triceps and anterior thigh) as compared to truncal region (i.e. sub-scapular and mid-axillary) between one and 12 months.
Greater accumulation of sub-cutaneous fat in all SGA infants as compared to normal Indian19, MGRS20 and western counterparts2122 shows that our SGA infants tend to accumulate more fat during their first year of life possibly to make up for intrauterine insufficiencies experienced by them. A phenomenon of catch-up growth in fat among SGA infants born thinner who later caught up with AGA peers32 corroborated with our findings. Yoshikawa et al33 reported that the sum thickness of four skinfolds (triceps, biceps, suprailiac and sub-scapular) in SGA infants was less at birth and caught up to AGA infants within one month, which supported a rapid postnatal catch-up fat phenomenon in SGA infants.
The tendency of symmetric SGA infants to accumulate more of sub-cutaneous fat than their asymmetric counterparts may have postnatal health consequences which need to be further explored from the standpoint of the foetal origin of adult disease hypothesis343536, particularly in context of Indian children who grow under a variety of environmental, nutritional, socio-economic conditions and constraints.
Financial support & sponsorship: None.
Conflicts of Interest: None.




