
Translate this page into:
Good's syndrome: Thymoma with hypogammaglobulinaemia
*For correspondence: doc.chengappa@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 49 yr old male† presented to the department of Clinical Immunology, Jawaharlal Institute of Postgraduate Medical Education & Research, Puducherry, India, in May 2016, with a two-year history of recurrent sinopulmonary infections, diarrhoea and weight loss. On evaluation, HIV serology was negative and routine biochemistry was normal except for hypogammaglobulinaemia. Chest X-ray (Figure A) showed mediastinal widening. Computed tomography of the thorax (Figure B) revealed a mass and later on confirmed to be thymoma-WHO Type-A (Figure C) on histopathology. Investigations for repeated infections revealed decreased levels of serum immunoglobulins (Ig) G, M, A and E. Flow cytometry analysis confirmed absent CD19+ B cells. Thymomas are known to cause numerous immune dysregulation syndromes, and Good's syndrome like in this case is one among them. The patient was started on maintenance intravenous immunoglobulin (IVIG) therapy and co-trimoxazole prophylaxis and is doing well on follow up. Good's syndrome is a rare cause of acquired B- and T-cell immunodeficiency, causing increased susceptibility to bacterial infections, and opportunistic fungal and viral infections. In adult-onset hypogammaglobulinaemia, an active search for thymoma may be warranted.
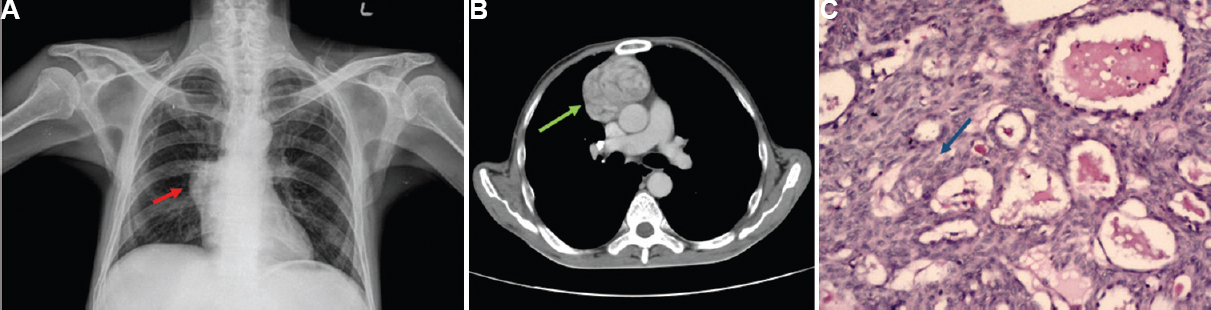
- (A) Chest X-ray PA view showing mediastinal widening (red arrow). (B) Axial section of computed tomographic scan showing anterior mediastinal mass (green arrow). (C) H and E section (×100) of the mass showing parenchyma comprising sheets of spindle cells with minimal lymphoid cells (arrow), arranged in short, storiform fascicles, vague whorls and interrupted by cystic spaces with focal microcystic pattern. Vascularity is increased with prominent perivascular spaces. Consistent with WHO-Type A thymoma.
Conflicts of Interest: None.




