
Translate this page into:
Global positioning system & Google Earth in the investigation of an outbreak of cholera in a village of Bengaluru Urban district, Karnataka
Reprint requests: Dr N.R. Ramesh Masthi, Department of Community Medicine, Kempegowda Institute of Medical Sciences, Banashankari 2nd stage, Bengaluru, 560 070, Karnataka, India e-mail: ramesh.masthi@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The global positioning system (GPS) technology along with Google Earth is used to measure (spatial map) the accurate distribution of morbidity, mortality and planning of interventions in the community. We used this technology to find out its role in the investigation of a cholera outbreak, and also to identify the cause of the outbreak.
Methods:
This study was conducted in a village near Bengaluru, Karnataka in June 2013 during a cholera outbreak. House-to-house survey was done to identify acute watery diarrhoea cases. A hand held GPS receiver was used to record north and east coordinates of the households of cases and these values were subsequently plotted on Google Earth map. Water samples were collected from suspected sources for microbiological analysis.
Results:
A total of 27 cases of acute watery diarrhoea were reported. Fifty per cent of cases were in the age group of 14-44 yr and one death was reported. GPS technology and Google Earth described the accurate location of household of cases and spot map generated showed clustering of cases around the suspected water sources. The attack rate was 6.92 per cent and case fatality rate was 3.7 per cent. Water samples collected from suspected sources showed the presence of Vibrio cholera O1 Ogawa.
Interpretation & conclusions:
GPS technology and Google Earth were easy to use, helpful to accurately pinpoint the location of household of cases, construction of spot map and follow up of cases. Outbreak was found to be due to contamination of drinking water sources.
Keywords
Cholera
Google Earth
GPS receiver
outbreak
spatial map
spot map

The global positioning system (GPS) technology is being used in various fields including agriculture, aviation, environment, defence, navigation, public safety, railways, etc., and also in the field of medicine. GPS provides much needed contextual information (e.g. location), and helps in exploring potential associations of how people are influenced by environmental factors such as housing, density of population and external environment1. GPS receiver and Google Earth (a geobrowser) together can be used to measure (spatial map) the distribution of the diseases in a specific geographical area.
Cholera occurs in sporadic, endemic, epidemic and pandemic forms. Large deltaic areas of Ganges and the Brahmaputra rivers are considered to be the homeland of cholera. In India epidemics of cholera are quite frequent. An average of 22,000 cases occur annually with a case fatality ratio (CFR) of 0.52 per cent2. In most parts of the world Vibrio cholerae El Tor biotype is the main cause of the outbreaks, which causes mild and asymptomatic diarrhoea as compared to the classical type toxigenic strains of V. cholerae belonging to the O1 and O139 serogroups which cause a devastating type of diarrhoa3.
In India there are no published studies regarding investigation of cholera outbreaks using GPS technology and Google Earth. Hence, this study was undertaken with the primary objective to find out the role of GPS technology and Google Earth in the investigation of a cholera outbreak and also to identify the cause of the outbreak so as to recommend control measures.
Material & Methods
Field survey: A cholera outbreak occurred in June 2013 at Maruthinagara village of Bengaluru Urban district, Karnataka, India. This village was covered under the field practice area of the rural health training centre (RHTC), department of Community Medicine, Bangalore Medical College, Bengaluru. The outbreak lasted for a period of 11 days (8-18 June, 2013). The Community Medicine department investigated this outbreak. All 3180 people living in the affected village were included in the study. A house-to-house survey for acute watery diarrhoea cases was done using a standard questionnaire which had information on age, sex, socio-demographic profile, source of water, environmental sanitation, food intake, travel history, etc. Standard case definition of cholera was used in the classification of cases: (i) in an area where disease is not known to be present, severe dehydration or death from acute watery diarrhoea in a patient aged 5 yr or more. (ii) laboratory criteria for diagnosis: isolation of V. cholerae O1 or O139 from stool samples of any patients with diarrhoea45. In case of locked houses, information was obtained from their neighbours. The neighbouring villages were excluded as no cases of acute watery diarrhoea were reported from them.
Spatial mapping using GPS coordinates: A handheld GPS receiver (Garmin GPS 72H) was used in the investigation. GPS receiver was switched on in front of the household of cases and the GPS information page displayed information regarding speed, elevation, satellite location, satellite signal, date, time and GPS receiver's current location (i.e. latitude and longitude in terms of degrees and minutes). These values were recorded in the standard questionnaire. All households with cases in the village were located to be spatial mapped. Similarly, GPS coordinates of suspected water sources were also recorded to be spatial mapped.
Spot map using Google Earth: On entering the GPS coordinates (obtained during the household survey) in a computer with Google Earth map (software) installed, the locations of households of the cases were pinpointed and displayed on the map. Subsequently locations of households were integrated with the thematic layers of Google Earth to generate the spot map.
Laboratory sample collection: Water samples were collected from all suspected sources which included three borewells and three household taps. After flaming the mouths of the taps, water was collected in sterile bottles with alkaline peptone water as transport medium and sent to the microbiology laboratory in reverse cold chain (vaccine carrier). The sample was cultured in bile salt agar with peptone water tellurite (PWT) as enrichment medium.
Results
The spot map generated using GPS coordinates and Google Earth showed clustering of cases around the suspected sources of water. These waypoints and routes saved in the GPS receiver were useful in the follow up of the cases. The Google Earth aerial view also identified the affected area from its surroundings, and gave information on the area which required action in the village. The spatial distribution of cases also showed the distance of the household from each other, from the source of water supply and distance to the nearest government health care provider. The spatial mapping of the cases is shown in Fig. 1.
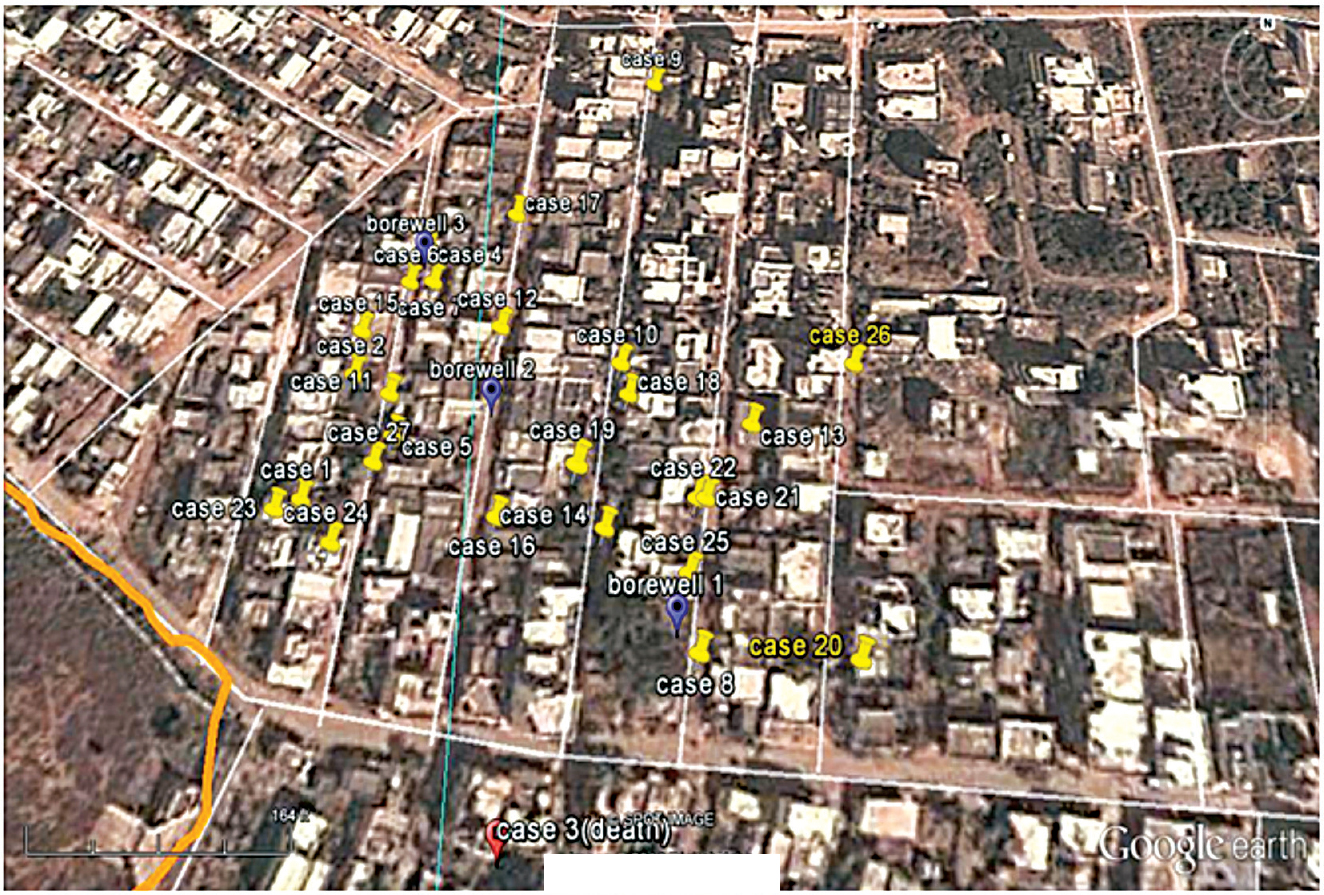
- Spot map showing spatial distribution of the cases using GPS and Google Earth.
Of the 3180 residents in the village, 390 (185 males, 205 females) consumed water from a particular source and all the 27 cases occurred amongst them (Hence, only 390 were taken as denominator for calculating attack rate). The primary case was a 21 yr old female who developed acute watery diarrhoea on June 8, 2013. None of the patients gave any history of travelling.
The age distribution of the cases ranged from 5 months to 93 yr. Male to female ratio was 1:1.55 (Table). The time distribution or epidemic curve of acute watery diarrhoea outbreak is shown in Fig. 2. The peak of the epidemic was seen on the third and fourth day of the outbreak. The course of the disease was on an average 2-7 days. The attack rate was 6.92 per cent (27 cases) and case fatality rate was 3.7 per cent (1 death). The attack rate was highest among 0-4 yr age group, 15.62 per cent (5/32) and among females 7.80 per cent (16/205). All cases presented with diarrhoea, 11 (40.74%) cases with vomiting, six (22.22%) with nausea, five (18.52%) with nausea and vomiting both and two (7.4%) with blood and mucus in stools. Three patients were hospitalized. Eight patients were treated with oral rehydration solution (ORS) and antibiotics, seven with ORS, intravenous fluids and antibiotics, two (7.4%) with iv fluid and antibiotics, five were given only ORS and another five cases did not take any treatment.

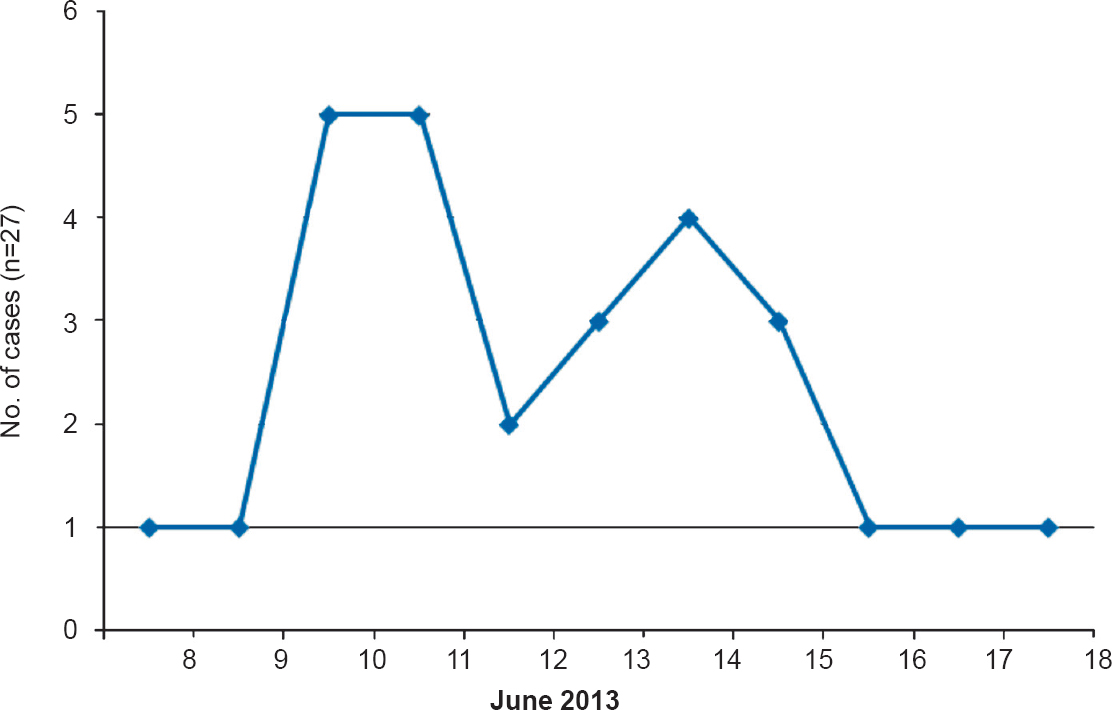
- Epidemic curve of cholera outbreak, June 2013.
The residents in the affected part of the village received water supply from three bore wells through pipelines which were interconnected. These pipelines were in close proximity with surface drains and at some places due to damage in pipelines the drinking water had come in contact with drainage water. There was indiscriminate garbage dumping in the area and open air defecation by children. Overcrowding was observed and housing standards were poor.
Water samples were collected from the three bore wells suspected to be the source of outbreak and three household taps. V. cholerae O1 Ogawa (only one strain) was isolated from all water samples. Stool sample microscopy (hanging drop preparation) of the index case done at the government hospital, revealed organisms with darting motility resembling V. cholerae. Preventive measures undertaken were cleaning of surface drains, disinfection of water source by chlorination, distributing of halogen tablets (chorine) for household purification of water and removal of garbage. Damaged pipes were repaired. Health education on prevention of water borne diseases was also given to the residents through distribution of pamphlets in local language.
Discussion
The advantage of spot map constructed with GPS technology and Google Earth was that an accurate identification of households where cases occurred, suspected source of contamination, the locality, topography and distance to nearest health centre was made available. Appropriate documentation of morbidity and mortality data is an issue in a resource scarce and vast country like India. Now with GPS technology, the location of the cases can be recorded permanently, and can be cross-checked independently. GPS technology and Google Earth will also be very useful in the data storage and retrieval at a later date for comparison and trend analysis. The advantage is that the GPS technology and Google Earth can be used at an affordable cost, thus avoiding use of expensive sophisticated software like Geographical Information System and other technologies available.
A study revealed that the GPS data could be used for mapping out the distribution of malaria vector mosquitoes, along with monitoring and evaluation of malaria control activities in various countries and also for risk mapping in analyzing the past as well as the present trends6. Another study used GPS data to show the geographical distribution of HIV infected patients and observed that the data could be used to implement the rollout of treatment as prevention in an efficient manner7. We have earlier shown the effectiveness of GPS in describing accurately the distribution of anaemia and malnutrition among 5-10 yr children8.
The cholera outbreak in this study was possibly due to the leakage in water supply, open air defecation near the source of water supply, water for drinking purposes not purified before drinking, no chlorination of water, and low socio-economic status of the population leading to poor environmental hygiene. The present outbreak was in concordance with sporadic outbreaks of cholera reported in most parts of India throughout the year. The attack rate and case fatality rate observed for various cholera outbreaks were 53 per cent and none5, 11.6 and 0.8 per cent9, respectively. Adults constituted majority of cases similar to that reported earlier1011. V. cholera O1 Ogawa was found to be the causative agent in other outbreaks reported312. Cholera outbreaks have been reported due to human consumption from contaminated water sources31314. Cholera continues to be a growing concern in most developing countries and constantly changing causative strains1516.
In conclusion, GPS technology and Google Earth were easy to use, helpful to accurately pinpoint the location of household of cases, and construction of spot map for the cholera outbreak.
Acknowledgment
The authors acknowledge the help and support provided by the PHC staff in carrying out the investigation, Microbiology department of the medical college and Dr Anwith, Tutor cum PG (Department of Community Medicine).
Conflicts of Interest: None.
References
- Global positioning system: a new opportunity in physical activity measurement. Int J Behav Nutr Phys Act. 2009;6:73.
- [Google Scholar]
- World Health Organization (WHO). Weekly Epidemiological Record, No. 40. 2015. Geneva, Switzerland: WHO; 90:517-44. Available from: http://www.who.int/wer/2015/wer9040/en
- [Google Scholar]
- Vibrio cholerae O1 Ogawa serotype outbreak in a village of Ambala district in Haryana, India. Indian J Community Med. 2011;36:66-8.
- [Google Scholar]
- Directorate of Health and Family Welfare, Karnataka. Notes on surveillance, prevention of communicable diseases. Bangalore: Government of Karnataka; 2004. p. :21-9.
- [Google Scholar]
- Directorate General of Health Services (DGHS), Government of India. Integrated disease surveillance project. Training manual for state & district surveillance officers. New Delhi: DGHS, Government of India; 2005. p. :71-2.
- [Google Scholar]
- Application of spatial technology in malaria research and control: some new insights. Indian J Med Res. 2009;130:125-32.
- [Google Scholar]
- Mapping HIV epidemics in sub-Saharan Africa with use of GPS data. Lancet Glob Health. 2013;1:251-3.
- [Google Scholar]
- Global positioning system: a new tool to measure the distribution of anaemia and nutritional status of children (5-10 years) in a rural area in south India. Indian J Med Sci. 2012;66:13-22.
- [Google Scholar]
- A cholera epidemic in a rural area of northeast India. Trans R Soc Trop Med Hyg. 2004;98:563-6.
- [Google Scholar]
- An El Tor cholera outbreak in Maldah district, West Bengal. J Commun Dis. 1999;31:49-52.
- [Google Scholar]
- An epidemic outbreak of Vibrio cholerae El Tor 01 serotype ogawa biotype in a Lalpur town, Jamnagar, India. J Postgrad Med. 2012;58:14-8.
- [Google Scholar]
- Severe cholera outbreak following floods in a northern district of West Bengal. Indian J Med Res. 2000;112:178-82.
- [Google Scholar]
- Transmission of epidemic Vibrio cholerae O1 in rural western Kenya associated with drinking water from Lake Victoria: an environmental reservoir for cholera? Am J Trop Med Hyg. 1999;60:271-6.
- [Google Scholar]
- New variants of Vibrio cholerae O1 biotype El Tor with attributes of the classical biotype from hospitalized patients with acute diarrhoea in Bangladesh. J Clin Microbiol. 2002;40:3296-9.
- [Google Scholar]
- Vibrio cholerae O139 Bengal: odyssey of a fortuitous variant. Microbes Infect. 2003;5:329-44.
- [Google Scholar]




