Translate this page into:
Frequency & specificity of RBC alloantibodies in patients due for surgery in Iran
Reprint requests: Dr Gharehbaghian A., Iranian Blood Transfusion Organization Research Center, Hemmat Exp. Way, Next to Milad Tower, Tehran, Iran e-mail: Gharehbaghian@ibto.ir
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Red blood cell alloimmunization is common in patients receiving multiple blood transfusions. Since the probability of repeat transfusion increases with longer life expectancy, it is important to study to which extent alloimmunized patients with a history of transfusion are prone to form alloantibodies after transfusion events. The aim of this study was to retrospectively analyze the alloimmunization against RBCs among transfused patients who were to undergo elective surgery in Tehran, Iran.
Methods:
A total of 3092 occasionally transfused patients, who were to undergo elective surgery, in four hospitals in Tehran were included in the study. For patients with alloantibodies, the data about sex, date of birth, history of transfusion, surgery, abortion and alloantibody specificity were collected.
Results:
Clinically significant alloantibodies were found in 30 patients. The presence of positive antibodies in the patients for whom cross-match had been done was one per cent. Most of them had surgery history or transfusion record during the preceding year. The three most frequent alloantibodies were anti-K (23.53%), anti- E (20.59%) and anti-c (17.56%).
Interpretation & conclusions:
The most common clinically significant alloantibodies identified in men and women were anti-K and anti-E, respectively. The most common causes of alloimmunization for men were surgery history and transfusion record and for women pregnancy.
Keywords
Alloimmuization
RBC antigens and antibodies
serological testing
transfusion-surgery

Alloimmunization is a common problem in patients undergoing blood transfusion. Most studies have been carried out on patients who chronically receive blood transfusions12345. In patients affected with haemoglobinopathies, haematologic diseases, various types of cancer, recipients of organ transplantation, and patients with renal failure, the prevalence of alloimmunization has been reported to be up to 60 per cent, while in hospitalized patients receiving transfusions alloimmunization has been seen in about 1 to 10 per cent12345.
The phenomenon of alloimmunization can lead to several problems varying from delay in getting similar blood to (delayed) haemolytic transfusion reactions1. Along with alloantibodies RBC autoantibodies are also developed. These autoantibodies may shorten the life span of RBCs of the blood recipients, and can lead to clinical haemolysis6.
It has been demonstrated that autoantibodies formation against RBC antigens after alloimmunization is not limited to patients who chronically receive blood transfusion7. The rate of RBC alloimmunization depends on the characteristics of the population being studied1289. The differences among the various populations, including race and sex differences make generalization of the results difficult. The frequency of blood group antigens is known among Iranian population10, but so far the relative frequencies of RBC alloantibodies in a general population of alloimmunized patients who occasionally receive blood transfusion, have not been determined. Previously performed studies have concentrated mainly on multiply transfused patients29 or patient groups like those affected with thalassaemia10. Therefore, the current study was designed to assess the frequency of alloimmunization to RBC antigens in the occasionally transfused patients due for surgery in Iran.
Material & Methods
Patients characteristics: To prevent any selection bias, antibody screening was done on randomly selected patients undergoing elective surgeries during 2008 and 2009 and the sample size was calculated based on obtained results from previous and similar studies. This study was conducted by the Iranian Blood Transfusion Organization (IBTO), Research Center, Tehran, Iran, and patients’ samples were collected from four general hospitals in Tehran viz. of Milad, Chamran, Imam Khomeini and Mofid hospitals with the number of samples being 2128 (68.8%), 600 (19.4%), 301 (9.7%), and 63 (2%), respectively. Of the total collected samples (n=3092), 1114 (36%) were for men and 1978 (64%) from were women. The patients were occassionally transfused patients and pregnant women to undergo elective surgery during 2008 and 2009. The study protocol was approved by the ethics committee of IBTO Research Center, Tehran. The patients’ samples were tested in the Immunohaematology department at IBTO Research Center. Each alloimmunized subject record was unique, and no individual was entered twice irrespective of the number of multiple antibody screening tests, some of them might have taken. Information on ABO, Rh typing, and gender was available for alloimmunized patients. The patients were divided into two subgroups: patients with alloantibody and patients without alloantibody.
The patient's age at the time of antibody detection, sex, the medical history, and the antibody specificity were entered into a registry for all positive antibody screens. It was possible to find anti-D in patients who had received Rh immunoglobulin (RhIg). While a patient may have had multiple antibody screens identifying a given antibody, that antibody was entered into the database only once, at the beginning. The information on both male and female patients’ profile and medical history was collected: sex, age, history of transfusion, history of surgery, history and frequency of pregnancy, history and frequency of abortion, history and frequency of D&C (Dilation and Curettage), and specificity of RBC alloantibodies. These data were collected from hospital medical records.
Serological testing: A standard protocol was performed on collected samples and a three-cell panel (Biotest cell-P3 LOT: 1922011, Germany) was used to screen for RBC alloantibodies using tube test method11. Albumin (Rinderalbumin 22% Biotest) was used for indirect antiglobulin method. After adding two part albumin to a mixture of two part serum and one part RBCs at room temperature, the resulted mixture was incubated for 15-30 min at 37°C. The cells were then washed three times in phosphate-buffered saline (PBS, pH=5.2, Iran Daru, Iran), and polyspecific anti-human globulin (AHG) serum (IBRF, Iran) was then added before spinning and final reading. All pretransfusion serum samples that had a positive antibody screen were investigated to identify the specificity of the alloantibody. Antibody specificity was determined using a commercial RBC panel (IBTO, Iran). The test was performed against the patient's serum in the same phases following antibody screening. The criteria for antibody specificity were based on recommendations by American Association of Blood Banks11.
Statistical analysis: The frequency of each alloantibody was assessed based on gender, date of birth, and history of transfusion, surgery, pregnancy, abortion, and alloantibody specificity. The test was performed to determine the difference in antibody distribution by gender, age, and history of surgery, abortion, and transfusion; P<0.05 was considered significant. The analyses and data management were performed using SPSS software version 16 (SPSS Inc, USA). The chi-square test was used for comparison of proportions in the two groups.
Results
Of the 3092 patients, 30 (1%) were positive for red cell alloantibodies. Of these 30, 29 patients showed clear specificity while one patient showed pattern of reactivity for which no specificity could be determined. The presence of antibodies in females with alloantibody was slightly higher, though not significant, than in males. Among the 30 patients who demonstrated true alloimmunization, 20 (67%) were females and 10 (33%) males.
Patients were also categorized according to their decade of birth. Patients born between 1971 and 1990 (20-39 yr old) comprised the largest group in the study, representing 1440 (47.2%) of the total population. The mean age in the alloimmunized patients group was 45.8 ± 3.2 yr, while the mean age in the non-alloimmunized patients group was 39.7 yr. No alloantibodies were detected in patients born after 2000.
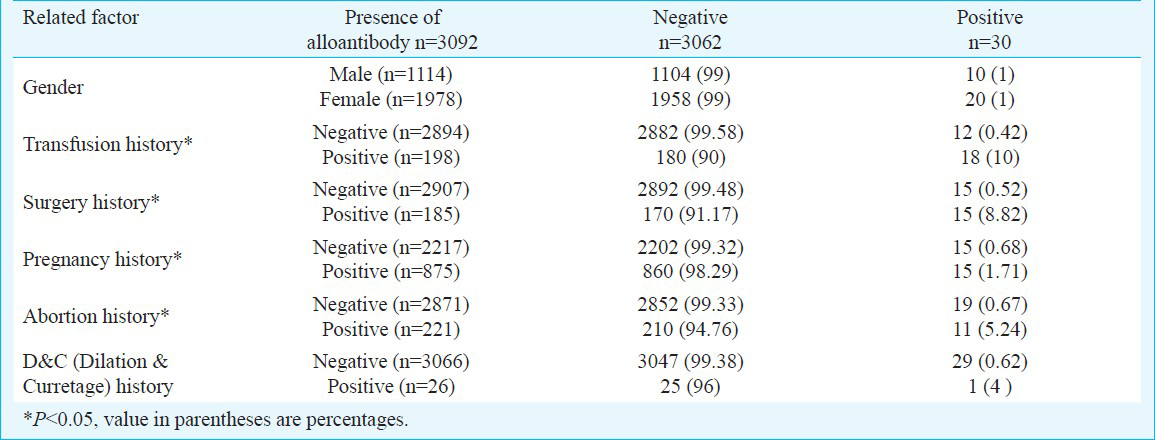
In this study, 0.42 per cent patients with no transfusion history and 10 per cent with transfusion history were positive for alloantibodies which showed significant difference between these two groups (P<0.05). Similarly, the difference between the negative and positive groups with hisotry of surgery, pregnancy and abortion was significant (P<0.05) (Table I). Of the 30 patients with alloanibodies, 18 (60%) had recorded history of previous transfusion; 15 (50%) had history of surgery; and 15 (50%) had history of pregnancy (Table I).
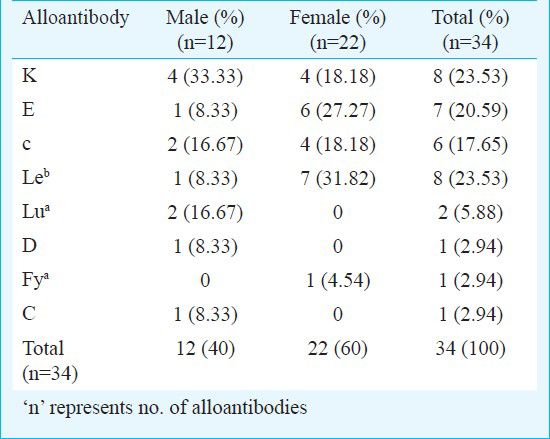
A total of 34 RBC alloantibodies were identified in 30 patients (35% in males, 65% in females). Of these, 26 (87%) had one alloantibody and four (13%) had two antibodies. Eight alloantibodies were detected with six having clinically significant RBC alloantibodies, listed by specificity and frequency as anti-K with 23.53 per cent (8/34), anti-E with 20.59 per cent (7/34), anti-c with 17.65 per cent (6/34), anti-D, anti-Fya, and anti-C with 2.94 per cent each (1/34); the other two cases were not shown to have clinically important RBC alloantibodies, listed by specificity and frequency as: anti-Leb with 23.53 per cent (8/34), anti-Lua with 5.88 per cent (2/34) (Table II). Overall, the most frequently identified alloantibody in men, as a percentage of total male antibodies, was anti-K with 33.33 per cent; and the most frequently identified alloantibody in women, as a percentage of total female antibodies, was anti-E with 27.27 per cent, followed by anti-K and anti-c with 18.18 per cent each (Table II).
Antibodies to E and Leb were more frequent among females with positive antibody screens. Antibodies to D, C and Lua were seen only among males with positive antibody screens.
Discussion
Transfusion of incompatible RBCs may lead to an immune-mediated haemolytic transfusion reaction, and to avoid such cases, pre-transfusion compatibility testing is carried out1112. The steps of pre-transfusion testing involve reviewing the acceptability of blood sample, checking the ABO group and Rh D type, antibody screening test, determining the specificity of antibodies detected unexpectedly, choosing donor RBC units suitable for recipients, and carrying out cross-match12. Thus, to avoide ABO-incompatible transfusions and unnecessary exposure to Rh D positive RBCs, determination of ABO group, Rh D typing, antibody detection, antibody identification, and cross- matching are recommended512.
Compared with the cross-match test, screening for the atypical antibody employs carefully selected cells, which were diluted optimally, and kept in a preservative solution. This test can be regularly controlled, preferably with every batch performed. The task can be carried out by inclusion of a control antibody, for instance a weak anti-D13.
In our study, 33 per cent patients who had alloantibodies were men, and 67 per cent were women. On the other hand, considering the total number of males and females tested, 10 (1%) of 1114 men and 20 (1%) of 1978 women had alloantibodies. Therefore, the current study has shown no difference in gender. The obtained results did not indicate a higher predominance of RBC alloimmunization in females compared to males, as shown by Natukunda et al5.
Our results showing the most probable causes for the alloimmunization in women and men as history of pregnancy and transfusion history, respectively, were similar to a study from India8. Further, alloimmunization rate in women with pregnancy history in our study was also comparable with this study8.
Since almost 60 per cent of patients with alloantibodies had transfusion history, it seems that transfusion has an important role as an alloimmunization factor. Almost 50 per cent patients with alloantibodies had surgery history, they would have probably been given transfusions during surgery. Therefore, surgery-related transfusion appears to be an important alloimmunization factor.
In this study the most frequently shown alloantibody was anti-K followed, by anti-E. In Western Europe and the United States the most frequently reported alloantibodies in alloimmunized patients were alloantibodies against Rh and Kell antigens5. The most frequently detected alloantibody in a study carried out in Olmsted County in Minnesota was anti-E; with anti-K as the second most frequently observed antibody9. Use of different enhancement methods can be considered as an explanation for this difference. In studies using methods that enhance detection of antibodies to Rh specificities, anti-E is detected more frequently9. We used albumin, which is a method that does not enhance Rh antibody detection.
Our study demonstrated that anti-E was the second most common alloantibody among females, followed by anti-K and anti-c. Currently, there exists no policy that obligates transfusion of ABO, and D-compatible blood for fertile women in State or private hospitals. Moreover, ABO, Rh grouping and alloantibody screening test (followed by antibody identification if alloantibody test is positive) for every women who is willing to have a baby is mandatory in Iran. This could be the reason for the obvious sex difference associated with anti-E and anti-c.
The high frequency of Leb in women during pregnancy age observed in our study was comparable to what has been shown by other studies914. During pregnancy, Lewis antigens become weaker, which occurs most often through associated appearance of anti-Leb914.
In most of studies done in Western societies, due to administration of anti-D immunoglobulin, a decrease has been observed in the frequency of anti-D (in women and subsequently in total population), accompanied with an increase in the prevalence of anti-K and anti-E19. In RhD-negative women, prophylaxis with anti-D immunoglobulin is routinely administered as an antenatal prophylaxis. This could have resulted in the lack of existence of anti-D observed in women in the current study.
The finding of anti-D alloantibody in a male patient was unexpected. This can be explained by the transfusion practice of using blood products untyped for the D antigen or mismatched RBC grouping or error in performing patient blood grouping or misinterpretation due to lack of comprehensive training. It was proposed to perform additional antigen compatibility (e.g., c, E, and K) to avoid the development of RBC antibodies in patients who chronically receive or need blood transfusion. Putting this policy into action has resulted in a considerable decline in alloimmunization rate and delayed haemolytic transfusion reactions in some studies15. However, regarding the selection of target patient populations for this policy, the discussion remains15.
In conclusion, our study demonstrated alloimmunization against RBC antigens among occasionally transfused patient population. The most common alloantibodies identified were anti-k in men and anti-E in women. However, the relative prevalence of RBC alloantibodies in the general population has not been determined.
Acknowledgment
This work was supported by a research fund allocated by Research Center of Iranian Blood Transfusion Organization. Authors thank Mrs M. Hadi, Mr G. Lotfi, and the technicians of the Blood Transfusion Laboratory of the Milad Hospital; Mr H. Bahrami Nasab, and the technicians of the Blood Transfusion Laboratory of the Imam Khomeini Hospital; Mrs Hoseini, and the technicians of the Blood Transfusion Laboratory of the Chamran Hospital; and Mrs F. Jadali, and the technicians of the Blood Transfusion Laboratory of the Mofid Hospital for technical help, and Mrs M. Rahbari, for statistical methodology.
References
- Additional red blood cell alloantibodies after blood transfusions in a nonhematologic alloimmunized patient cohort: is it time to take precautionary measures? Transfusion. 2006;46:630-5.
- [Google Scholar]
- A prospective study of the incidence of red cell allo-immunisation following transfusion. Vox Sang. 1996;71:216-20.
- [Google Scholar]
- Evaluation of transfusion reactions in thalassemic patients’ referred to the Thehran adult thalassemia clinic. ZUMS J. 2008;16:57-66.
- [Google Scholar]
- Antibody screening and identification by gel method in thalassemic patients. J Khoon. 2008;5:99-108.
- [Google Scholar]
- Prevalence and specificities of red blood cell alloantibodies in transfused Ugandans with different diseases. Vox Sang. 2010;98:167-71.
- [Google Scholar]
- Autoantibody formation in the alloimmunized red blood cell recipient: clinical and laboratory implications. Arch Intern Med. 2001;161:285-90.
- [Google Scholar]
- Autoantibody formation after alloimmunization: are blood transfusions a risk factor for autoimmune hemolytic anemia? Transfusion. 2004;44:67-72.
- [Google Scholar]
- The prevalence of irregular erythrocyte antibodies among antenatal women in Delhi. Blood Transfus. 2011;9:388-93.
- [Google Scholar]
- RBC alloantibody specificity and antigen po-tency in Olmsted County, Minnesota. Transfusion. 2001;41:1413-20.
- [Google Scholar]
- Blood group antigens frequency: a comparative study in intermediate thalassemics versus healthy people in Isfahan. J Khoon. 2005;2:23-9.
- [Google Scholar]
- Technical Mannual. (16th ed). Bethesda MD: American Association of Blood Banks; 2008.
- [Google Scholar]
- North American Pretransfuion Testing Practices, 2001-2004: results from the College of American Pathologists. Interlaboratory Comparison Program survey data 2001-2004. Arch Pathol Lab Med. 2005;129:984-9.
- [Google Scholar]
- Red blood cell alloantibody frequency, specificity, and properties in a population of male military veterans. Transfusion. 2008;48:2069-76.
- [Google Scholar]
- Alloimmunization and erythrocyte autoimmunization in transfusion-dependent thalassemia patients of predominantly Asian descent. Blood. 2000;96:3369-73.
- [Google Scholar]




