
Translate this page into:
Expression of p16INK4a in oropharyngeal squamous cell carcinoma from a tertiary cancer centre of South India: A preliminary study
For correspondence: Dr Sangeetha K. Nayanar, Department of Clinical Laboratory Services & Translational Research, Malabar Cancer Center, Thalassery, Kerala 670 103, India e-mail: sgeethanayanar@yahoo.com
-
Received: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Human papillomavirus (HPV) and oropharyngeal squamous cell carcinoma (OPSCC) are found to be strongly associated with each other with an increase in incidence has been noted globally over the years. A literature search for data depicting the role of HPV in oropharyngeal carcinoma in South India, however, has resulted in little information, thus, the present study was aimed to assess a possible association between the two among OPSCC patients from a tertiary care cancer centre in South India.
Methods:
One hundred and fourty three OPSCC cases were included in the study and analyzed for age, gender, marital status, habits, clinical TNM staging, site, laterality, symptoms, histological type (keratinizing and non-keratinizing), primary treatment and follow up period. All the cases were subjected to p16INK4a immunostaining. Statistical analysis was done using SPSS software.
Results:
Of the 143 cases 12 were found to be p16 positive with no significant difference between the study variables among p16 positive and negative cases. Base of the tongue was the most commonly involved site for the p16 positive cases. The p16 positive cases presented at an elderly age, early stage and were mainly the keratinizing type.
Interpretation & conclusions:
The p16 positive OPSCC cases constituted a small proportion in the present study and behaved similar to p16 negative cases. Usage of tobacco and alcohol appear to be the susceptible factors even in p16 positive cases. More studies from other States would be helpful to determine if HPV-related SCC in the Indian subcontinent behave differently or similarly to cases from Western countries.
Keywords
Immunostaining
keratinizing
HPV
oropharyngeal
p16
South India
squamous cell carcinoma

A robust association is well established between human papillomavirus (HPV) and oropharyngeal squamous cell carcinoma (OPSCC) and an increase in incidence has been noted over the years1. It has also been estimated that approximately 38,000 cases of head and neck cancer are attributable to HPV worldwide, out of which 21,000 cases are of OPSCC occurring more in developed countries2. The prevalence of HPV in cancer cases is howbeit mainly derived from the studies conducted in the western countries of Europe and North America, yielding an average prevalence of approximately 40 per cent2.
The latest WHO blueprint of head and neck cancers has segregated oropharyngeal carcinomas into HPV positive and negative categories3. Both subtypes show a significant difference in age, histopathology, p16 immunostaining as well as in the overall survival rate. Lewis4 opined that diffuse immunostaining of p16 in OPSCC is a reliable surrogate marker and may thus be used as a standalone test for the HPV status in tumours with appropriate morphology arising in the oropharynx. Extensive p16 immunostaining correlates significantly with transcriptionally active HPV4. The p16 immunostaining has now been adopted both by the fourth edition of WHO classification of head and neck tumours as well as the eighth edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual35.
The clinical characteristics including the HPV status in this distinct entity vastly vary across geographical regions and with different ethnicities1. Based on HPV genotyping by consensus polymerase chain reaction and reverse line-blot hybridization assay in north Indian population, Bahl et al6 found 22.8 per cent prevalence of HPV in OPSCC with no significant associations between tobacco or alcohol consumption with HPV status. In another single institution study from India on p16 and HPV status in SCC of oropharynx, hypopharynx and larynx, Murthy et al7 observed p16 expression in 20 per cent cases and HPV positivity was detected in 39.4 per cent cases. A search in the English literature for data depicting the role of HPV in oropharyngeal carcinoma in South India has resulted in dearth of information, thus, in the present preliminary study, OPSCC cases were subjected to p16INK4a immunostaining to assess if there was an association between HPV and OPSCC among South Indian patients.
Material & Methods
Study design: The present study was designed and conducted in the department of Clinical Laboratory Services and Translational Research, Malabar Cancer Centre, Thalassery, Kerala, after obtaining approval from the Institutional Review Board and Ethical Committee. Over a period of six years (January 2012 - December 2017), 238 oropharyngeal cases were retrieved from the archival files of the department. Three cases of adenoid cystic carcinoma, nine cases of diffuse large cell lymphoma, one sarcomatoid carcinoma and ten cases where only epithelial dysplasia was noted on slides were excluded. Further, 72 cases without paraffin-embedded tumour specimens and/or slides were also not included. Thus, finally, a total of 143 satisfactory cases of OPSCC were included in the study. The complete demographic profile, clinical data and treatment detail of all study participants were retrieved from the medical records. Data were analyzed for age, gender, site, laterality, habits, marital status, symptoms, clinical TNM staging, histological type (keratinizing and non-keratinizing)3 primary treatment and follow up period. Cases where keratinization was absent/inconspicuous histologically without surface dysplasia were considered as non-keratinizing OPSCC while keratinizing OPSCC had ample evidence of keratinization and often associated surface dysplasia3. All the samples irrespective of histological type were subjected to p16 immunostaining.
Immunohistochemistry: Four micron thick sections were taken on Poly-L-Lysine coated slides, incubated overnight at 50°C in a hot air oven and de-paraffinized in three changes of xylene for 10 min each followed by rehydration through graded alcohols. Antigen retrieval was done by heating slides immersed in EDTA buffer (pH 9) in a pressure cooker and the procedure consisted of three whistles followed by cooling for 20 min. Tissue sections were blocked in PolyExcel hydrogen peroxide block for 5 min (PathnSitu Biotechnologies Pvt. Ltd., Hyderabad, India). The pH was maintained between all the steps using Tris buffered saline (pH 7.4). Subsequently, the sections were incubated in mouse anti-human p16INK4a monoclonal antibody (Clone MX007, Master Diagnostica S.L., Granada, Spain) for 10 min followed by treatment with PolyExcel Target Binder for 10 min, PolyExcel PolyHPR for 10 min and PolyExcel Stunn DAB (diaminobenzidine) working solution for 5 min at room temperature (PathnSitu Biotechnologies Pvt. Ltd. Hyderabad, India). Counterstaining was done with Harris haematoxylin. Slides were finally mounted in DPX. Prior antigenicity of the sections was tested by vimentin immunostaining. The p16 positive cases of cervical dysplasia were used as external positive control. Negative control sections were processed by omitting primary antibody.
Scoring and statistical analysis: Two pathologists evaluated histological type and p16 expression in OPSCC simultaneously, under a double-headed compound microscope at 400x magnification. All the cases were categorized in binary manner as positive or negative. The interpretation of p16 immunostaining was done based on DAHANCA/EORTC guidelines (https://www.dahanca.dk/uploads/TilFagfolk/Guideline/GUID_Scoring_and_classification_of_p16_2012.pdf) for scoring which states strong and uniform dual nuclear and cytoplasmic expression of p16 in 70 per cent of tumour cells was regarded as positive while the expression either in nucleus or cytoplasm alone and non-uniform weak or patchy staining was considered negative8.
Descriptive statistics were done for frequency counts followed by Chi-square and Fisher’s exact tests, as appropriate, were used to determine the association between clinico-demographic variables (other than age and pack years) and p16 status. Comparison of mean age and pack years between p16 and positive and p16 negative groups was done using Levene’s test for equality of variances and t test for equality of means. P<0.05 was considered statistically significant. Event of interest was death due to any cause. Survival curves were plotted using Kaplan–Meier graphs and Log rank test was used to compare p16 positive and negative cases. Statistical analysis was done on IBM SPSS software (IBM Analytics, Armonk, New York, U.S.).
Results
Socio-demographic, clinical and histological tumour characteristics of cases: Table I show details of various characteristics of p16 positive and negative OPSCC cases. Out of 143 cases, only 12 cases were p16 positive while remaining 131 cases were negative for p16 immunostaining. We observed that the mean age in p16 negative cases was 61.7 yr (±9.76). Males were clearly affected more than females. Smoking was the most common deleterious habit followed by alcohol and chewing. Mean pack years for p16 negative OPSCC cases was 36.33 (±13.05). One hundred and twenty-seven participants were married with left side being most commonly affected. Eighty one cases were of keratinizing squamous cell carcinoma and the remaining 50 were non-keratinizing. A similar trend was noted in p16 positive cases with no statistically significant difference between the two groups.
| Variables | Total (%) | p16 negative (131/143) (%) | p16 positive (12/143) (%) | P |
|---|---|---|---|---|
| Age (years) | 61.57 (9.78) | 61.37 (±9.76) | 63.75 (±10.21) | 0.423 |
| Gender | ||||
| Male | 134 (93.7) | 124 (94.7) | 10 (83.3) | 0.167 |
| Female | 9 (6.3) | 7 (5.3) | 2 (16.7) | |
| Habits | ||||
| Smoking | ||||
| Yes | 130 (90.9) | 120 (91.6) | 10 (83.3) | 0.299 |
| No | 13 (9.1) | 11 (8.4) | 2 (16.7) | |
| Mean pack years | 36.33 (±13.05) | 37.93 (±12.87) | 0.899 | |
| Alcohol | ||||
| Yes | 100 (69.9) | 94 (71.8) | 6 (50) | 0.184 |
| No | 43 (30.1) | 37 (28.2) | 6 (50) | |
| Chewing | ||||
| Yes | 35 (24.5) | 32 (24.4) | 3 (25) | 0.9999 |
| No | 108 (75.5) | 99 (75.6) | 9 (75) | |
| Marital status | ||||
| Married | 138 (96.5) | 127 (96.9) | 11 (91.7) | 0.359 |
| Unmarried | 5 (3.5) | 4 (3.1) | 1 (8.3) | |
| Laterality | ||||
| Right | 53 (37.1) | 48 (36.6) | 5 (41.7) | 0.648 |
| Left | 76 (53.1) | 71 (54.2) | 5 (41.7) | |
| Bilateral | 2 (1.4) | 2 (1.5) | 0 | |
| Central | 12 (8.4) | 10 (7.6) | 2 (16.7) | |
| Histological type | ||||
| Keratinizing | 89 (62.2) | 81 (61.8) | 8 (66.7) | 0.9999 |
| Non-keratinizing | 54 (37.8) | 50 (38.2) | 4 (33.3) | |
| Clinical T | ||||
| T1 | 21 (14.7) | 17 (13) | 4 (33.33) | 0.053 |
| T2 | 61 (42.7) | 57 (43.5) | 4 (33.33) | |
| T3 | 36 (25.2) | 35 (26.7) | 1 (8.33) | |
| T4 | 25 (17.5) | 22 (16.8) | 3 (25) | |
| Clinical N | ||||
| N0 | 47 (32.87) | 44 (33.59) | 3 (25) | 0.254 |
| N1 | 52 (36.36) | 47 (35.88) | 5 (41.7) | |
| N2 | 42 (29.37) | 39 (29.77) | 3 (25) | |
| N3 | 2 (1.4) | 1 (0.76) | 1 (8.3) |
The detailed description of 12 positive cases is shown in Table II. Twelve cases out of 143 (8.45%) showed both nuclear and cytoplasmic positivity in more than 70 per cent of tumour cells and were thus categorized as p16 OPSCC. Mean age of occurrence was 63.75 (±10.21) with a male predominance. All patients but one had a history of tobacco usage in any form. Eight positive cases were keratinizing type histologically (6 were well differentiated, 1 was moderately differentiated and another was keratinizing papillary type) (Fig. 1). Interestingly, only one p16 positive case was a female participant without any deleterious habit and the tumour was keratinizing papillary type histologically.
| Age (yr) | Gender | Smoking (pack years) | Alcohol | Chewing | Chief complaint | Site of involvement | Histological type |
|---|---|---|---|---|---|---|---|
| 55 | Male | Yes (32) | Yes | No | Dysphagia | BOT | Non-keratinizing |
| 67 | Male | Yes (43) | Yes | No | Swelling | Tonsil | Keratinizing |
| 50 | Male | Yes (34) | No | No | Pain | BOT | Keratinizing |
| 55 | Male | Yes (34) | No | No | Dysphagia | BOT | Keratinizing |
| 68 | Male | Yes (53) | Yes | No | Dysphagia | Tonsil | Non-keratinizing |
| 72 | Male | Yes (36) | No | No | Pain | BOT | Keratinizing |
| 70 | Female | No | No | No | Neck Swelling | Tonsil | Keratinizing (papillary) |
| 73 | Female | No | No | Yes | Ulcer | BOT | Non-keratinizing |
| 73 | Male | Yes (50) | Yes | Yes | Dysphagia | BOT | Keratinizing |
| 70 | Male | Yes (55) | Yes | No | Swelling | BOT | Keratinizing |
| 43 | Male | Yes (12) | Yes | Yes | Dysphagia | Soft palate | Keratinizing |
| 69 | Male | Yes (30.25) | No | No | Foreign body sensation | PPW | Non-keratinizing |
BOT, base of tongue; PPW, posterior pharyngeal wall
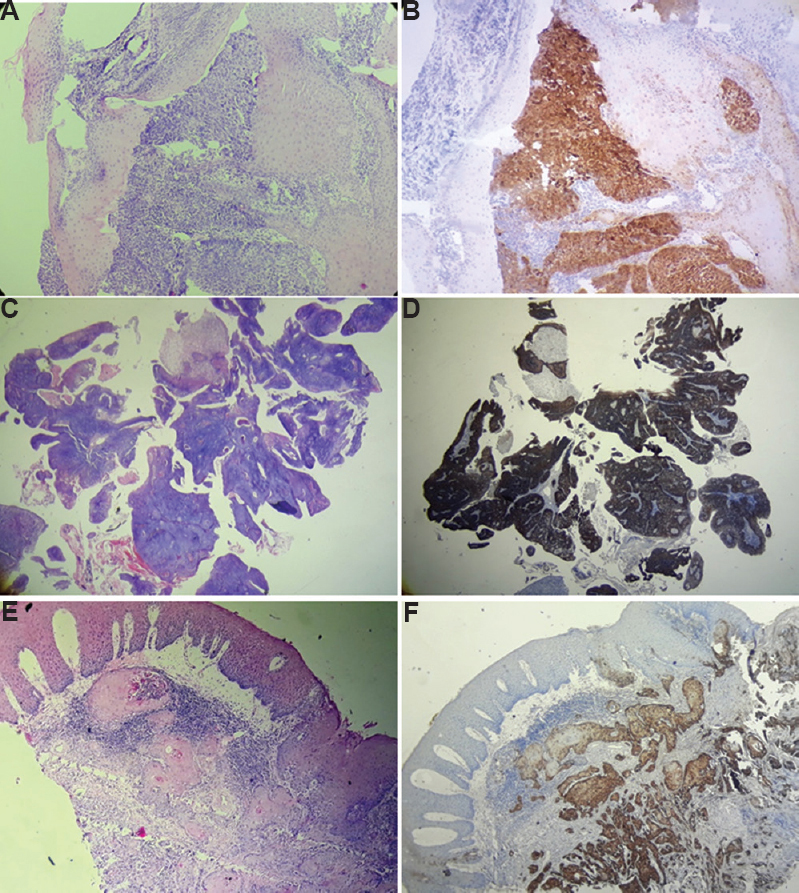
- (A) Haematoxylin eosin (H&E) photomicrograph of non-keratinizing OPSCC (10x) and, (B) corresponding p16 positivity by IHC (x10); (C) H&E photomicrograph of keratinizing papillary OPSCC (x4) and, (D) corresponding p16 positivity by IHC (x4) (E) H&E photomicrograph of keratinizing OPSCC (x10) and (F) corresponding p16 positivity by IHC (x10). OPSCC, oropharyngeal squamous cell carcinoma.
Chief complaints and site of involvement: 30.6 per cent of p16 negative cases (40/131) and 41.7 per cent of p16 positive cases (5/12) presented with dysphagia followed by pain (29%) and neck swelling (35%) in p16 negative and positive OPSCC cases, respectively. Fig. 2 shows comparative presentation of frequency of chief complaints for 131 cases of p16 negative OPSCC and 12 cases of p16 positive OPSCC.

- Comparative distribution of chief complaints of p16 positive and negative patients (n=143).
The oropharynx was subdivided into subsites according to AJCC Cancer Staging Manual5. p16 negative tumours mainly affected tonsils (48/131) followed by base of tongue (38/131) while reverse pattern was seen p16 positive tumours where base of tongue was most commonly affected (7/12) followed by tonsils (3/12). Detailed frequency-wise distribution for most commonly involved site in p16 negative and positive tumours is shown in Fig. 3.
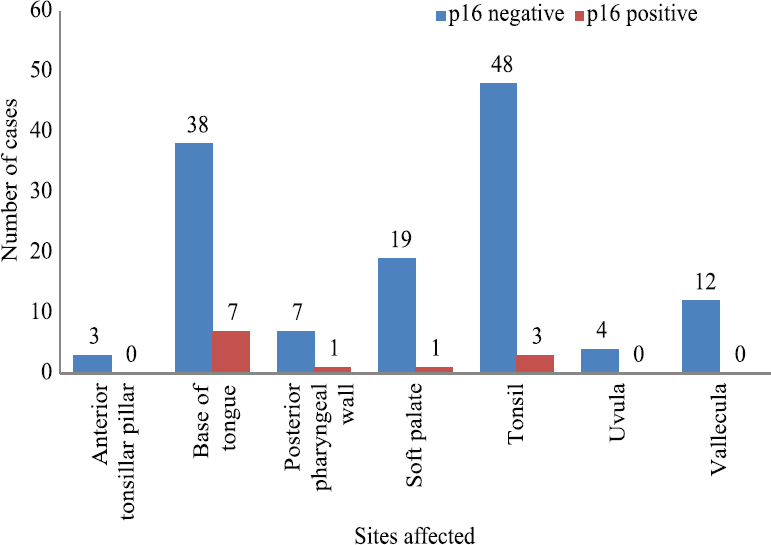
- Comparative distribution of sites affected by p16 positive and negative patients (n=143).
Treatment and survival analysis: Irrespective of the histological type external beam radiotherapy with or without concurrent chemotherapy was the most common type of therapy given. The mean disease-free survival for p16 negative participants was 36.134 months (median - 32 months) as compared to p16 positive OPSCC cases where it was 36.08 months (median - 36 months; Fig. 4). There was, however, no significant difference seen in the overall survival between the two groups (P=0.54).

- Kaplan–Meier curve for overall survival stratified by tumour p16 status.
Discussion
p16 negative and positive squamous cell carcinoma are now considered as two distinct entities with different risk factors, clinical and demographic profiles and outcomes, with the results mainly derived from western population. The results from India are, however, conflicting and insufficient679. The present study is one of its kind comprising of patients from the Malabar region of South India (Dravidian ethnicity, linguistically Malayalam). The cases in the present cohort were from the northern districts of the Kerala State of India, namely Kannur, Kasargode, Kozhikode and Wayanad. In a previous study from similar population, no role of HPV was found in oral cancers including nine cases of tonsillar squamous cell carcinoma9, methodology, however, was different from the present study.
This study aimed to describe the clinicopathological parameters of OPSCC and immunohistochemical analysis of p16 expression, a surrogate marker recommended by WHO for determining the HPV status. Since we did not know the status of p16 in our study population, all the cases irrespective of histological type were subjected to p16 IHC. It was found that 12/143 (8.39%) cases were truly positive with both nuclear and cytoplasmic staining in over 70 per cent of cells while rest of the 131 cases were p16 negative. The percentage of p16 positive cases was, however, much lower than that reported in studies from west and north India61011. In contrast to the previous studies6, we found no difference in mean age between p16 positive and negative cases. Furthermore, the mean age of p16 positive cases was higher than the previous reported cases. The age of occurrence was close to oropharyngeal SCC patients from Australia where median age was found to be 60 yr1. Rettig et al12 also concluded recently that the average age of HPV positive OPSCC is shooting up over the years. Similarly, no difference was found in gender, habits, histological types and staging between the two groups.
For 12 p16 positive cases, the mean age of occurrence was 63.75 yr (median=68.5) with a male-to-female ratio of 5:1. As reported and accepted previously, the p16 positive cases have a unique histology3. p16 positive OPSCC has been described to bear a non-keratinizing morphology with minimal keratinization. Tumour cells show high nucleo-cytoplasmic ratio with increased mitotic count and lack of stromal reaction. p16 negative carcinomas in contrast show histology similar to conventional keratinizing oral SCC. Chernock et al13 divided OPSCC into three histological categories as non-keratinizing, keratinizing and hybrid. OPSCC are divided into two broad categories, keratinizing and non-keratinizing type3. The same criteria were used in the present study to first segregate all cases into keratinizing and non-keratinizing types. However, these criteria seem unacceptable in the present cohort. In total, 54/143 cases showed non-keratinizing morphology suggestive of HPV association, however, only four cases showed positive immunostaining for p16. Remaining eight positive cases were of keratinizing SCC. One out of these eight positive cases had the morphology of keratinizing papillary SCC. HPV-related papillary SCC has been reported in literature1415. Cai et al16 opined that the p16 and HPV status carries more importance rather than the histological type of SCC.
In the present study, p16 positive cases mainly affected the base of the tongue followed by tonsils. p16 positive OPSCC are shown to affect mainly young males unlike in the present study. Apart from oral sexual practices and tobacco usage, poor oral hygiene is correlated with HPV infection in recent studies1718. Thus, HPV-related OPSCC could be multifactorial. Furthermore, HPV-related SCC has a tendency to present at high stage and with better patient survival1920. In contrast, we found that in both the groups, majority of the cases presented at early stage with no significant difference in survival.
However, there were some limitations. First, the HPV testing by an RNA-based method could not be done for p16 positive cases owing to resource constraints. However, this population-based study can still be considered a preliminary attempt. Second, the similarity in the outcome of the p16 positive and negative cases may be attributed to unequal number of cases and limited statistical power to show any significant difference. Another shortcoming was a lack of details of sexual practices, the marital status could be retrieved from the medical records but the sexual habits were not mentioned.
In summary, p16 positive OPSCC constitute a small proportion and may behave similar to p16 negative cases. No significant difference was found between p16 positive and negative cases in age, gender distribution, habits, stage and overall survival. Most p16 positive cases were of the keratinizing type, presented at an elder age and early stage contrary to previous reports. More studies from other States would be helpful to determine if HPV-related SCC in the Indian subcontinent behaves differently to the cases from Western countries or not.
Acknowledgment
Authors acknowledge Ms P.B. Amrutha for her help in immunohistochemistry and Medical Records Division, Malabar Cancer Centre, Thalassery, Kerala for timely providing the records of the patients.
Financial support & sponsorship: The project (Q3/AO/17/MCC/01) was intra-murally funded by Malabar Cancer Centre, Thalassery, Kerala.
Conflicts of Interest: None.




