
Translate this page into:
Expression of inflammatory proteins STAT & NFĸB for phenotypic diagnosis of gall bladder cancer: A pilot study
#Equal contribution
For correspondence: Dr Bela Goyal, Department of Biochemistry, All India Institute of Medical Sciences, Rishikesh 249 203, Uttarakhand, India e-mail: lifeline.bela@gmail.com
-
Received: ,
Accepted: ,
Abstract
Background & objectives
Gallbladder cancer (GBC) has a low overall survival rate due to late detection and poor prognosis. Chronic inflammation contributes to malignant conversion and metastasis in GBC. Expression of inflammatory proteins, such as signal transducer and activator of transcription factor (STAT) and nuclear factor kappa B (NFĸB) proteins, for diagnosis through immunohistochemistry (IHC) is a promising area of research; however, diagnosis of GBC through IHC-based methods is still in its infancy. So, the present pilot study explores the use of STAT proteins (STAT 3 and 6) and NFĸB as diagnostic biomarkers for GBC.
Methods
Histologically confirmed cases of GBC (n=13) and cholelithiasis (n=23) as controls, were recruited. IHC was performed for protein expression of STAT3, STAT6, and NFĸB. Subgrouping into high and low expression was performed based on the receiver operating curve (ROC) analysis. Diagnostic utility and its association with the aggressiveness of cancer were assessed.
Results
The mean age of GBC and cholelithiasis patients was 50.84±14.5 and 44.0±11.9 years, respectively. Liver infiltration and metastasis were observed in 61 per cent and 69 per cent of the patients, respectively. STAT3, STAT6, and NFĸB expressions were significantly higher in GBC as compared to cholelithiasis. Sensitivity and specificity for STAT3 and STAT6 were 91, 47 and 75, 39 per cent, respectively. STAT6 expression was associated with lymph node involvement. Whereas, both STAT3 and STAT6 expressions were associated with Liver infiltration.
Interpretation & conclusions
This pilot study demonstrated STAT3 and STAT6 as sensitive and specific molecular biomarkers for diagnosing and assessing the aggressiveness of GBC. These may be used as an adjunct to the diagnosis of GBC after validation on a larger sample size.
Keywords
Chronic cholecystitis
gall bladder cancer (GBC)
inflammatory proteins
NFĸB
STAT

Gallbladder cancer (GBC) is considered one of the most lethal forms of malignancies affecting the gastrointestinal tract, with a higher prevalence in women and an overall survival rate below one year1,2. The low survival rate is majorly due to non-specific presentation and asymptomatic progression, which results in detection at a very late stage3,4. Two major mechanisms for gall bladder carcinogenesis have been proposed to be recurrent cholecystitis secondary to cholelithiasis and, less commonly, anomalous pancreaticobiliary junction5.
Inflammatory responses play a pivotal role in tumour development, malignant conversion, and metastasis via cross-talk between tumour infiltrating immune cells and cancer cells. Member of signal transducer and activator of transcription factor (STAT) and nuclear factor kappa B (NFĸB) stimulate the synthesis of chemokines like IL-6, IL-4, and IL-13, which attract additional immune/inflammatory cells to exaggerate tumour-associated inflammation further6. Among the members of the STAT family,STAT6 and STAT3 are more commonly studied in various cancers. Nearly 20 per cent of human cancers are associated with chronic inflammation. Inflammatory proteins/chemokines have been utilised as biomarkers for the diagnosis and prognosis of cancers, including colorectal cancer and GBC7,8. Immunohistochemistry (IHC)-based cancer diagnosis, especially in assessing biomarkers, is commonly considered as gold standard for characterising tumour subtypes, tissue origin, distinguishing metastasising tumours from primary tumours and predicting therapy response in various cancers, including breast and pancreatic cancers9-11. However, the utilisation of this technique is still in its infancy in GBC. Moreover, inflammatory pathway proteins are increasingly being considered for targeted therapeutic approaches.
The present study is an attempt to explore the utility of STAT3, STAT6, and NFĸB as diagnostic biomarkers for GBC, which is able to discriminate GBC from chronic inflammatory conditions like cholelithiasis employing IHC.
Materials & Methods
This study was undertaken at the department of Biochemistry, All India Institute of Medical Sciences, Rishikesh between March 2020 to July 2023 and included histologically confirmed cases of GBC (n=13); patients with cholelithiasis (n=23) were recruited as controls. This study was approved by the Institute’s Ethics Committee (IEC), and informed consent was in accordance with the Declaration of Helsinki. Participants were recruited after obtaining informed consent. Individuals with metachronous and synchronous malignancies were excluded from the study. Clinical and demographic characteristics of all the study participants were recorded. Histological staging was carried as per the AJCC (American Joint Committee on Cancer) 8th edition12.
Sample collection and IHC
5 μm sections of formalin-fixed and paraffin-embedded tissue specimens were obtained from tissue biopsy specimens of GBC and cholelithiasis patients. IHC was performed to assess the protein expression of STAT3, STAT6, and NFĸB. Deparaffinisation and dehydration of blocks was done with xylene and ethanol. The overnight incubation was performed with primary antibodies (Invitrogen MA, USA) against pSTAT3 (dilution 1:10-1:100), pSTAT6 (Invitrogen, MA, USA) (dilution 1:75) and pNFĸBp65 (Invitrogen, MA, USA) (diluted 1:100 – 1:500). Next, incubation with HRP (Horseradish Peroxidase) conjugated secondary antibodies, followed by staining with DAB (3,3’-Diaminobenzidine) and counterstaining with haematoxylin was done.
Interpretation of IHC staining patterns
The intensity of immunostaining was evaluated at different magnifications, and tumour cells were counted in the hotspot region, defined as the area with the highest density of positively stained cells, with a minimum of 500 cells analysed. For positive staining, a brown precipitate in the nucleus and cytoplasm of cells was considered a positive reaction. Whereas the absence of significant staining within the tumour cells was considered negative staining. The semi-quantitative scoring system was used to assess the intensity and extent of staining (e.g., 0, 1+, 2+, 3+).
Scores for intensity (0: negative, 1: weak, 2: moderate, & 3: intense) and percentage of positive cells (0: negative, 1-25: 1, 26-50: 2, 51 -75: 3, and ≥76: 4) were added. The intensity of cells was graded as follows: Mild: 1+, Moderate: 2+, Intense: 3+, and the proportion of cells was <50 per cent focal and >50 per cent diffuse.
Subgrouping into high and low expression was done based on the optimal cut-off obtained by employing the Youden index in ROC analysis. The coordinate points and cut-off in ROC analysis were determined based on the maximum Youden index and using optimal cut-off, GBC cases were sub-grouped into high and low score groups. The pathological diagnosis was made by two pathologists independently, who were blinded to the clinico-pathological data and research content.
Statistical analysis
STATA version 11 statistical software (StataCorp LP; College Station, Texas, USA) was used for data analysis. The normal distribution of data was assessed using the Shapiro-Wilk W test. The Mann-Whitney U test was performed to analyse the difference in the expression of molecular markers in IHC between the study groups. The ROC analysis was performed in SPSS (IBM ver.21; IBM Corp., Armonk, NY, USA) to assess the discriminatory ability of STAT3, STAT6 and NFĸB expression score to identify GBC. Further, Youden’s index was utilised to determine the sensitivity and specificity of these scores at an optimal cut-off. Based on the optimal cut-off, GBC was sub-classified into high and low score groups. Chi-square (χ2) was used to determine the association of TNM (tumor, node, metastasis) and lymph node infiltration with high and low score GBC groups. P<0.05 was considered as a statistically significant difference.
Results & Discussion
In the present study, the mean age of participants with GBC and cholelithiasis was 50.84±14.5 yr and 44.0±11.9 yr, respectively. GBC was more common in females than males (69.23% female and 31% male). Similarly, in cholelithiasis, the percentage of male vs. female was 26.09 and 73.91 per cent. In several studies, gallstones and GBC have been found to be more prevalent in women globally as well as in the Indian population13-16, which supports the present study showing a 2.23 times higher incidence rate in the case of females compared to males.
In the present study, stages II, III, and IV of GBC were observed in 3 (23.08%), 8 (61.54%) and 2 (15.38%) participants, respectively. Liver infiltration was observed in 61 per cent of the GBC patients, whereas 69 per cent of the patients presented with lymph node involvement and metastasis. The baseline demographic and clinico-pathological parameters of the study participants have been summarised in supplementary table I.
Around 75 per cent of GBC patients in the current study presented at an advanced stage. This corroborates the large body of evidence that demonstrates, owing to the insidious onset of GBC and lack of typical clinical manifestations in the early stages, most patients presented at the advanced stage when diagnosed, resulting in a loss of opportunity for radical surgery17-19. This also explains the small sample size of the GBC patients in the present study.
The tissue expression of STAT3, STAT6, and NFĸB was significantly higher in GBC as compared to the cholelithiasis group. The mean ±SD scores for STAT3, STAT6, and NFĸB in GBC vs. cholelithiasis were 4 ±1.5, 1.3 ±1.2 (P<0.01); 3.8±2.4, 2.0±1.4; P<0.01 and 3.8±2.1, 2.4±2.0; P<0.05, respectively. Representative IHC images for both GBC and cholelithiasis have been shown in figure 1. ROC analysis showed a high area under the curve (AUC) of 0.9 and 0.73 for STAT3 and STAT6. While AUC for NFĸB was 0.69 (Fig. 2). The sensitivity and specificity for STAT3 and STAT6 were 91, 47 and 75, 39 per cent with optimal cut-off of 1.5 and 2.5, respectively. NFĸB showed a sensitivity of 58 per cent and specificity of 30 per cent at an optimal cut-off of 3.5.
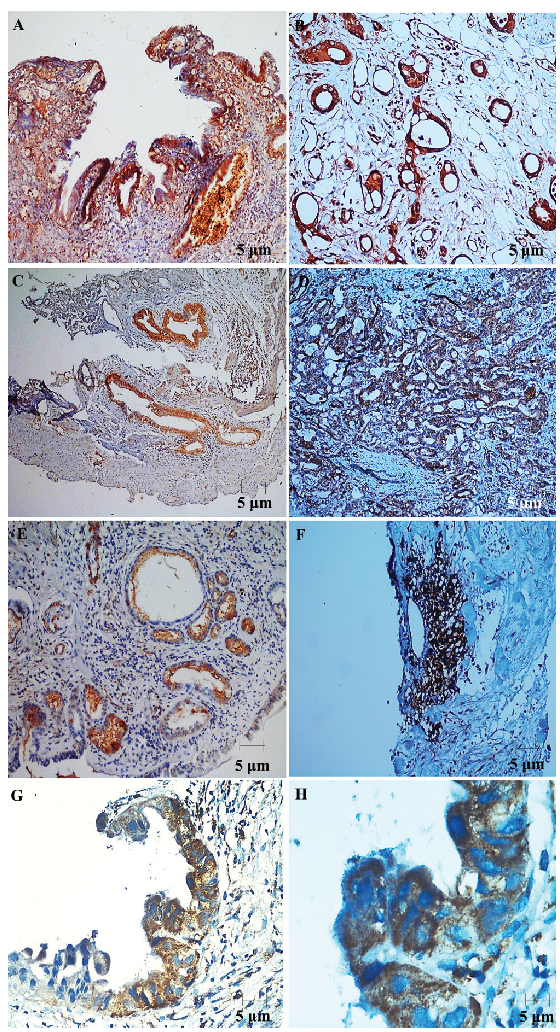
- Immunohistochemistry of STAT and NFĸB in GBC and cholelithiasis. Representative immunohistochemistry (IHC) staining images illustrating the expression of STAT3, STAT6, and NFĸB in cholelithiasis and gallbladder adenocarcinoma. Panels (A), (C), and (E) show nuclear and cytoplasmic expression of STAT3, STAT6, and NFĸB in cholelithiasis, while panels (B), (D), and (F) depict the expression in gallbladder adenocarcinoma. Images (A), (C), (D), (E), and (F) are captured at 20× magnification, whereas image (B) is captured at 40× magnification. Additionally, panels (G) and (H) present representative images of STAT6 expression in gallbladder adenocarcinoma at 40× and 100× magnification, respectively, highlighting tumor cells exhibiting predominantly cytoplasmic and focal nuclear immunopositivity for STAT6.
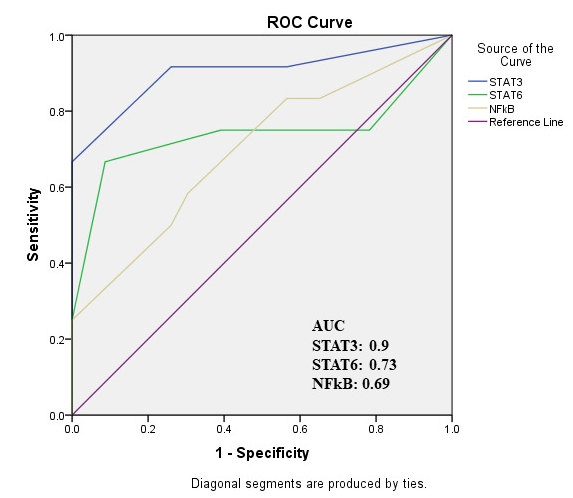
- Receiver operating characteristics curve for STAT and NFĸB. ROC curve for STAT3, STAT6 and NFĸB with corresponding AUC (area under curve) value.
Chronic Inflammation is long known to be a potential risk factor for GBC. NFĸB and STAT are key mediators of crosstalk between cancer and inflammation. There is a limited body of evidence elucidating the molecular mechanisms underlying GBC, particularly in relation to the involvement of the JAK/STAT signalling pathway. As per the evidence from several studies, IL-6/JAK/STAT3 signalling is believed as a key signalling pathway for tumour progression, and has been confirmed in many types of cancers, including hepatocellular cancer, breast cancer and lung adenocarcinomas20,21. A recent preclinical study demonstrated that GBC-associated fibroblasts promote vascular mimicry formation and tumour progression in GBC by upregulating NOX4 expression. This effect was driven via paracrine IL-6 mediating IL-6/JAK/STAT3 signalling pathway as evidenced by elevated expression levels of IL-6, JAK1, JAK2, and STAT3 in both in vitro and in vivo models21. Furthermore, another study22 reported that an increased expression of STAT3 and vascular mimicry in GCB tissues correlate with lower differentiation, greater malignancy, and advanced clinical stage. This suggests that STAT3 may facilitate vascular mimicry formation during tumour initiation, progression, and metastasis. Therefore, targeting STAT3 could inhibit tumour cell proliferation and invasion while preventing vascular mimicry development, making it a promising candidate for anti-angiogenic cancer therapy. This clearly shows the involvement of STAT3 and STAT6 in the molecular pathogenesis of cancer, and as potential candidates to be explored as biomarkers and therapeutic targets.
However, in the current study, NFĸB showed low sensitivity and specificity for discriminating cancer from chronic inflammatory conditions. The plausible explanation for this could be that NFĸB expression is more specific to inflammation per se and not specifically associated with cancer progression. Moreover, literature suggests the dual role of NFĸB as both pro-inflammatory and anti-inflammatory mediator in different phases of the disease23. Another reason for the low expression of NFĸB in the current study could be the involvement of a larger number of patients from an advanced stage of GBC.
In the present study, a significant association was observed between high expression of STAT6 and lymph node involvement (P<0.05). Likewise, liver infiltration was seen with a high proportion in individuals with high STAT3 and STAT6 expression compared to low expression (6:1). No association was observed with tumour stage or metastasis. NFĸB failed to show any association with clinico-pathological parameters. The association of clinico-pathological parameters with IHC expression of STAT3, STAT6 and NFĸB proteins in GBC has been depicted in supplementary table II. The association of STAT6 and STAT3 expressions with lymph node and liver infiltration indicate the role of STAT as a mediator of not only cancer-related inflammation but also as a promoter of tumour spread. This result is in agreement with the previous studies, which demonstrated a significant association of STAT6 expression with the histological tumour grade, node infiltration and distant metastasis in breast cancer24,25. However, GBC is still unexplored in this respect. Thus, the findings of the present study may pave the way towards STAT as a potential sensitive and specific biomarker for GBC and a potential therapeutic target with the potential to curtail the spread of such highly aggressive malignancy.
IHC has long been successfully employed in breast cancer for directing the targeted therapy10. Anti-inflammatory agents like aspirin and celecoxib are being explored for their therapeutic potential in colorectal cancer26. A randomised phase II clinical trial has also evaluated the efficacy of JAK2 inhibition in individuals with triple-negative inflammatory breast cancer27. Similarly, a recent clinical trial has investigated STAT3 inhibition as a therapeutic strategy in glioblastoma28 demonstrating target engagement and clinical efficacy. However, as per the authors’ knowledge and a researching Clinical Trial Registry (CTRI) and other internet sources no clinical trials have been conducted to date targeting the JAK/STAT pathway in GBC. The current proof-of-principle study may be an important step to direct further research and clinical trials for the utility of STAT proteins in otherwise difficult-to-manage GBC patients.
In conclusion, this study demonstrated STAT as a sensitive and specific molecular biomarker for diagnosis and assessing the aggressiveness of GBC. However, this is a pilot study where most of the patients were from an advanced stage and from a single geographical area. Therefore, a conclusive statement on the utility of STAT and NFĸB may not be possible. However, this can be a first step towards the targeted approach in reducing the disease burden of otherwise difficult-to-manage and aggressive diseases like GBC. It is recommended to conduct further research with a larger sample size.
Financial support & sponsorship
This study received financial support from the Uttarakhand Council for Science and Technology (UCOST), India (UCS&T/R&D-10/19-20/17602/1).
Conflicts of Interest
None.
Use of Artificial Intelligence (AI)-Assisted Technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing of the manuscript and no images were manipulated using AI.
References
- Risk factors associated with gall bladder cancer in high incidence areas in India: A systematic review protocol. BMJ Open. 2022;12:e056849.
- [Google Scholar]
- Genetic landscape of gallbladder cancer: Global overview. Mutat Res Rev Mutat Res. 2018;778:61-7.
- [Google Scholar]
- Common genetic variation and risk of gallbladder cancer in India: A case-control genome-wide association study. Lancet Oncol. 2017;18:535-44.
- [Google Scholar]
- Gallbladder carcinoma in the United States: A population based clinical outcomes study involving 22,343 patients from the surveillance, epidemiology, and end result database (1973-2013) HPB Surg. 2017;2017:1532835.
- [Google Scholar]
- Staging, treatment, and future approaches of gallbladder carcinoma. J Gastrointest Cancer. 2018;49:9-15.
- [Google Scholar]
- Circulating inflammatory proteins and gallbladder cancer: Potential for risk stratification to improve prioritization for cholecystectomy in high-risk regions. Cancer Epidemiol. 2018;54:25-30.
- [Google Scholar]
- Tumor biomarkers for diagnosis, prognosis and targeted therapy. Signal Transduct Target Ther. 2024;9:132.
- [Google Scholar]
- Significance of immunohistochemistry in breast cancer. World J Clin Oncol. 2014;5:382-92.
- [Google Scholar]
- Review of immunohistochemistry biomarkers in pancreatic cancer diagnosis. Front Oncol. 2021;11:799025.
- [Google Scholar]
- The 8th Edition American Joint Committee on Cancer Staging for Hepato-pancreato-biliary Cancer: A Review and Update. Arch Pathol Lab Med. 2021;145:543-53.
- [Google Scholar]
- Gallbladder cancer worldwide: Geographical distribution and risk factors. Int J Cancer. 2006;118:1591-602.
- [Google Scholar]
- Population-based study to estimate prevalence and determine risk factors of gallbladder diseases in the rural Gangetic basin of North India. HPB (Oxford). 2011;13:117-25.
- [Google Scholar]
- Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-42.
- [Google Scholar]
- Research progress on prognostic factors of gallbladder carcinoma. J Cancer Res Clin Oncol. 2024;150:447.
- [Google Scholar]
- Evaluation and management of incidental gallbladder cancer. Chin Clin Oncol. 2019;8:37.
- [Google Scholar]
- Epidemiological Study of gallbladder cancer patients from North Indian gangetic planes--a high-volume centre’s experience. J Gastrointest Cancer. 2016;47:27-35.
- [Google Scholar]
- Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat Rev Clin Oncol. 2018;15:234-48.
- [Google Scholar]
- Gallbladder cancer-associated fibroblasts promote vasculogenic mimicry formation and tumor growth in gallbladder cancer via upregulating the expression of NOX4, a poor prognosis factor, through IL-6-JAK-STAT3 signal pathway. J Exp Clin Cancer Res. 2020;39:234.
- [Google Scholar]
- Expression of STAT3 and vasculogenic mimicry in gallbladder carcinoma promotes invasion and metastasis. Exp Ther Med. 2021;22:738.
- [Google Scholar]
- The complexity of NF-κB signaling in inflammation and cancer. Mol Cancer. 2013;12:86.
- [Google Scholar]
- STAT-5 and STAT-6 in breast cancer: Potential crosstalk with estrogen and progesterone receptors can affect cell proliferation and metastasis. J Clin Med Res. 2022;14:416-24.
- [Google Scholar]
- Targeting the Stat6 pathway in tumor-associated macrophages reduces tumor growth and metastatic niche formation in breast cancer. FASEB J. 2018;32:969-78.
- [Google Scholar]
- Inflammation and tumor progression: Signaling pathways and targeted intervention. Signal Transduct Target Ther. 2021;6:263.
- [Google Scholar]
- TBCRC 039: a phase II study of preoperative ruxolitinib with or without paclitaxel for triple-negative inflammatory breast cancer. Breast Cancer Res. 2024;26:20.
- [Google Scholar]
- A first-in-human Phase I trial of the oral p-STAT3 inhibitor WP1066 in patients with recurrent malignant glioma. CNS Oncol. 2022;11:CNS87.
- [Google Scholar]




