
Translate this page into:
Expression analysis of apolipoproteins AI & AIV in hepatocellular carcinoma: A protein-based hepatocellular carcinoma-associated study
For correspondence: Dr. Premashis Kar, Department of Medicine, Maulana Azad Medical College, University of Delhi, New Delhi 110 002, India e-mail: premashishkar@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Hepatocellular carcinoma (HCC) is one of the leading causes of cancer mortality. The objective of this study was to find out the differential expression of apolipoproteins (ApoAI and ApoAIV) in HCC and cases of liver cirrhosis and chronic hepatitis (controls) without HCC and to compare ApoAI and ApoAIV expression with alpha-foetoprotein (AFP), the conventional marker in HCC.
Methods:
Fifty patients with HCC and 50 controls comprising patients with liver cirrhosis (n=25) and chronic hepatitis (n=25) without HCC were included in this study. Total proteins were precipitated using acetone precipitation method followed by albumin and IgG depletion of precipitated protein using depletion kit. Proteins were separated by sodium dodecyl sulphate-polyacrylamide gel electrophoresis. The expression changes of ApoAI and ApoAIV were confirmed by western blotting using specific primary and secondary polyclonal antibodies followed by densitometric protein semi-quantitative estimation. ApoAI, ApoAIV and AFP were measured in the plasma samples by ELISA method.
Results:
Semi-quantitative densitometric image analysis of the western blot images and the comparison between HCC patients with those without HCC (control) revealed differential expression of ApoAI and ApoAIV. Levels of ApoAI were significantly higher in patients with HCC compared to controls without HCC (0.279±0.216 vs 0.171±0.091 and 0.199±0.014; P <0.001). Levels of ApoAIV were significantly lower in patients of HCC compared to controls without HCC (0.119±0.061 vs 0.208±0.07 and 0.171±0.16; P <0.01). ELISA assays of apolipoproteins (ApoAI and ApoAIV) revealed similar results of expression of ApoAI and ApoAIV as detected in western blotting densitometric image analysis.
Interpretation & conclusions:
Increased expression of ApoAI and decreased expression of ApoAIV in HCC patients compared to controls without HCC revealed the abnormalities in HCC. These molecules need to be studied further for their use as potential biomarkers in the future diagnostic tools along with other conventional biomarkers for screening of HCC cases. It needs further analysis in higher number of patient population.
Keywords
Alpha-foetoprotein
apolipoprotein
apolipoprotein-AI
apolipoprotein-AIV
hepatocellular carcinoma

Hepatocellular carcinoma (HCC) is a major cause of mortality among patients with chronic liver disease. In India also, the number of cases of HCC is rising1. HCC represents the major histological subtype of primary liver cancers2, and it is one of the major causes of cancer-related death worldwide3. Moreover, HCC is one of the most common malignancies and an important cause of death all over Asia and Africa4. The representative data on epidemiology of HCC in India are scanty. HCC is usually diagnosed at an advanced stage leading to limited options for therapy and poor prognosis. Bruix et al5 have reported that HCC accounts for about 80 per cent of primary liver tumours in the Asian and Pacific regions.
Apolipoproteins bind to lipids to form lipoproteins and transport the lipids through lymphatic and circulatory systems. Apolipoprotein-AI (ApoAI) is the major protein component of high-density lipoprotein (HDL) in the plasma6. ApoAI is a 243 amino acid long, single polypeptide derived from a precursor, pre-ApoA. Apolipoprotein-AIV (ApoAIV) is a plasma protein which is a 377 amino acid long peptide that encodes 46 kDa proteins6. The levels of ApoAI and ApoAIV have been found to be the factors independently associated with HCC in comparison to cirrhosis and chronic hepatitis7.
The diagnosis of HCC cases is based on imaging techniques and also based on measurement of serum tumour markers such as alpha-foetoprotein (AFP), AFP lectin fraction L3 (AFP-L3) and des-gamma-carboxy-prothrombin (DCP). However, for detecting HCC in early stage, the sensitivity of AFP or DCP was only 30-60 per cent of the expected8. Although the combination of measurements of AFP and DCP can improve the diagnostic efficiency and performance, the diagnostic accuracy is low for HCC. As per the guidelines for American Association for the Study of Liver Diseases (AASLD)9, the sensitivity and specificity of AFP in diagnosis of HCC are poor. AFP-L3, a fucosylated variant of the AFP has been shown to have better specificity for diagnosis of HCC cases than that of AFP (63-91.6%), but with a low sensitivity (36-71%)810.
The plasma level of apolipoproteins (HDL) is inversely related to chronic liver diseases such as HCC and liver cirrhosis. Contribution of apolipoproteins on the biological functions of HCC and also aberrant expression of ApoAI and ApoAIV is correlated with the development and progression of cancers11. Based on these observations, it was thought that ApoAI and ApoAIV expression level may be useful as biomarkers for diagnosis and prognosis of HCC. Therefore, this study was designed to find out whether the differential expression of ApoAI and ApoAIV in HCC cases either alone or in combination could discriminate patients with HCC from those of liver cirrhosis and chronic hepatitis without HCC, and also to compare the expression of these apolipoproteins with the conventional marker of HCC, i.e. AFP.
Material & Methods
Recruitment and enrolment of patients: The confirmed patients with HCC, patients with liver cirrhosis without HCC and those with chronic hepatitis without cirrhosis and HCC were included in this study. A total of 50 HCC patients (n=50) with confirmed diagnosis were selected from the patients admitted to the medical ward and also from the Outpatient Departments (OPD) of Medicine and Gastroenterology of the Lok Nayak Jai Prakash Hospital, New Delhi, India. The sample size was calculated based on test of two-proportion statistical method and two means method12. Those patients who fulfilled the inclusion criteria and were willing to give written informed consent were included. The study protocol was approved by the ethics committee of the Maulana Azad Medical College and Associated Hospitals, New Delhi. The study was conducted during February 2013 to October 2014.
The AASLD 201113 updated guidelines were followed to select HCC patients. The imaging modalities used were triphasic computed tomography (CT) abdomen scan which showed arterial hypervascularization, washout in the portal venous or delayed phase13. AFP ≥200 ng/ml was an additional criterion for diagnosis of HCC cases.
The control group consisted of patients with chronic hepatitis without liver cirrhosis and HCC (n=25) and liver cirrhosis without HCC (n=25) and healthy individuals (n=10). The diagnosis of chronic hepatitis was based on the recommendation by AASLD 2009 updated guidelines14.
According to the AASLD recommendations, the patients were evaluated on the basis serological analysis for liver function test. The features for inclusion of chronic hepatitis were persistent or intermittent elevation in alanine aminotransferase (ALT)/aspartate aminotransferase (AST) levels, and liver biopsy showing chronic hepatitis (necroinflammatory score ≥4).
The diagnosis of liver cirrhosis was considered on the basis of following criteria: (i) presence of ascites, splenomegaly and shrunken liver, (ii) endoscopic examination showing oesophageal varices, and (iii) imaging features for liver cirrhosis viz. evidence of surface nodularity (88% sensitive, 82-95% specific), overall coarse and heterogeneous echotexture and segmental hypertrophy/atrophy15.
To ensure the presence of small HCC in patients with liver cirrhosis, triphasic CT abdomen scan was performed which showed the following features: arterial hypervascularization, washout in the portal venous or delayed phase and characteristics recommended by AASLD 201113.
The division of patients with HCC, liver cirrhosis and chronic hepatitis with respect to viral aetiology of hepatitis B or C viruses (HBV or HCV) was as follows: HCC with HBV (n=45), HCC with HCV (n=5), chronic hepatitis with HBV (n=20), chronic hepatitis with HCV (n=5), liver cirrhosis with HBV (n=18) and liver cirrhosis with HCV (n=7). All HBsAg-positive cases were HBV DNA positive. None of the cases had occult HBV infection. Patients with concomitant dyslipidaemia such as metabolic syndromes and congenital apolipoprotein abnormalities were excluded from the study.
Sample collection: Peripheral blood samples (5 ml) were collected from all patients and controls and serum stored at −80°C. Blood samples were collected in ethylenediaminetetraacetic acid (5.4 mg) vial for plasma and plasma aliquots were stored at −80°C for protein expression analysis and quantification using ELISA method for target ApoAI, ApoAIV and AFP.
Biochemical analysis: Complete panel of liver function tests including levels of AST, ALT, serum alkaline phosphatase, serum albumin, serum bilirubin, serum protein and international normalized ratio (INR) was determined using standard protocol of kit manufacturer (Erba Diagnostics, USA).
Serological analysis: Serological tests were performed for the detection of hepatitis B surface antigen (HBsAg), hepatitis B core IgG antibody (HBcIgG), hepatitis B envelope antigen (HBeAg) and anti-HCV antibodies. HCV RNA and HBV DNA were also quantified using PCR techniques. These experiments were done using commercially available kits (CUSABIO, USA) according to the manufacturer's protocol and ELISA method.
Expression analysis of ApoAI and ApoAIV depletion of albumin and IgG from human plasma: The plasma protein in the human blood comprises 70-90 per cent albumin and IgG16. To decrease the load and noise of albumin and IgG molecules in the sodium dodecyl sulphate (SDS) gels, all plasma samples were depleted against albumin and IgG using ‘ProteoPrep Blue Albumin and IgG Depletion Kit’ (Sigma Aldrich, USA) following the manufacturer's protocol. A volume of 50 μl plasma samples was depleted using 400 μl depletion medium provided in the kit and 35 μl was the final eluted protein volume. Blood plasma samples were treated with Triton X-100 buffer or radioimmunoprecipitation assay (RIPA) buffer to open up the protein folding. These samples were incubated overnight, and wherever necessary, treated with β-mercaptoethanol to break the disulphide bond found in protein to release the proteins of interest and to make the protein movable in the SDS-polyacrylamide gel electrophoresis (PAGE) gel and blot transfer to nitrocellulose membrane. Depleted plasma samples were precipitated using acetone precipitation method.
Protein estimation: Bradford assay method was used to estimate the protein levels17. Bradford protein assay kit - pre-diluted protein assay standards: BSA set (Thermo scientific, USA) was used for the protein estimation experiment.
SDS-PAGE: Depleted and acetone-treated plasma samples were subjected to SDS-PAGE gel electrophoresis to separate the protein present in the plasma. The separation of protein was analyzed by 12 per cent SDS-PAGE gel electrophoresis to determine the differential expression of ApoAI and ApoAIV protein in samples of HCC cases in comparison to those with liver cirrhosis and chronic hepatitis without HCC. PAGE Mark protein ladder (10Kd) (G Biosciences, India) having concentration 100 ng/μl was used for marking in SDS.
Conformation of apolipoprotein: ApoAI and ApoAIV were confirmed by western blotting using primary and secondary antibodies along with HRP (Horseradish Peroxidase) and TMB (3,3’,5,5’-tetramethylbenzidine) chromogen substrate using a femtoCHROMO™HRP chromogenic detection kit for western blots following the manufacturer's protocol (G Biosciences, Noida). For western blot, the protein separated by SDS-PAGE was immobilized on a nitrocellulose membrane using western blot transfer system (DCX-700, CBS Scientific Co., CA, USA). Subsequently, proteins were detected using primary polyclonal antibody [anti-human apolipoprotein rabbit 10 antibody (Assaypro, Russia)] and HRP-conjugated secondary antibody [anti-rabbit apolipoprotein goat 20 antibody (G Biosciences, India)] by fluorescence method using TMB chromogen substrate following by the manufacturer's protocol. For densitometry image analysis, western blots were scanned and analyzed by ImageJ software (NIH, USA).
Determination of ApoAI & ApoAIV and AFP using ELISA methods: Analysis of ApoAI, ApoAIV and AFP in all samples was done by the third-generation ELISA using Cusabio ApoAI, ApoAIV and AFP ELISA kit following the manufacturer's protocol (CUSABIO, USA).
Statistical analysis: Demographical and clinical data were evaluated for all the patients, and the odds ratios and 95 per cent confidence intervals (CIs) were calculated for each risk factor using Student's t test. Receiver operating characteristic (ROC) curve analysis was performed to determine the diagnostic power of apolipoproteins and AFP. Student's t test and correlation analysis was applied to evaluate all the ELISA data.
Results
The mean age (±standard deviation) of HCC patients and control without HCC was 56.55±9.53 yr and 51.33±10.65 yr, respectively. Of the 45 HCC cases, HBsAg were found to be positive in 91.1 per cent (n=41), while 31.11 per cent (n=14) were HBeAg positive. ALT and AST levels were significantly higher in HCC compared to control without HCC. The mean concentration of ALT and AST in cases was 84.44±35.04 IU/ml and 107.66±35.99 IU/ml, respectively.
Expression analysis of ApoAI and ApoAIV: Semi-quantitative digital densitometric image analysis of western blot images of the plasma samples and the comparison between patients with and without HCC revealed differential expression of ApoAI and ApoAIV. Levels of ApoAI were significantly (P <0.001) higher in patients with HCC than in controls without HCC (Table IA). Levels of ApoAIV were significantly (P <0.01) lower in patients of HCC than in patients with liver cirrhosis and chronic hepatitis without HCC (Table IA).
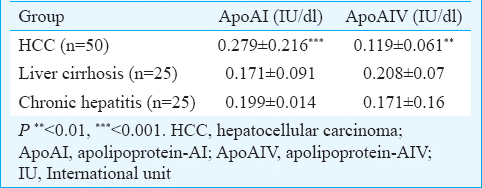
The plasma levels of ApoAI were significantly (P <0.001) higher in HCC cases compared to both the healthy and disease controls. On the other hand, plasma levels of ApoAIV were significantly (P <0.001) lower in HCC cases compared to those with liver cirrhosis and chronic hepatitis but without HCC (Table IB). Plasma levels of AFP were significantly (P <0.05) higher in HCC cases compared to healthy control but not with those with liver cirrhosis and chronic hepatitis without HCC.

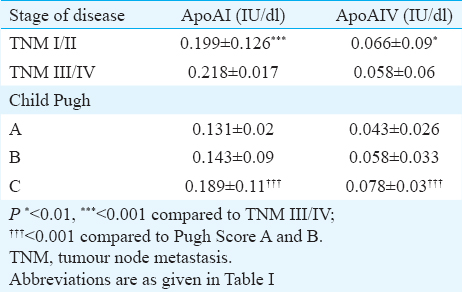
The expression of ApoAI was significantly (P <0.001) higher in HCC cases with tumour node metastasis (TNM) stage III-IV compared to HCC with TNM stage I-II (Table II). ApoAI expression was significantly higher in Child Pugh C compared to Child Pugh A and B (P <0.001; Table II). The expression of ApoAIV was significantly higher in HCC with TNM stage I-II compared to HCC with TNM stage III-IV (P <0.05, Table II). ApoAIV expression was significantly higher in Child Pugh C compared to Child Pugh A and B (P <0.001; Table II). ApoAI and ApoAIV expression levels and the risk factors such as tumour size and tumour number were found to be non-significant in HCC (Table II).
ApoAI, ApoAIV and AFP were further tested to find out whether quantitative measurement could be utilized as a diagnostic tool to distinguish patients with HCC from the controls without HCC. ROC curve analysis of all the ELISA data were analyzed for ApoAI, ApoAIV and AFP. For ApoAI, the ROC curve analyses of all the data rendered an area under the curve (AUC) of 0.901±0.031 (P=0.001; 95% CI 0.840-0.962) at a 4747.19 ng/ml cut-off (Table III). For ApoAIV, the ROC curve showed an AUC of 0.875±0.035 (P <0.01; 95% CI 0.758-0.913) at a 318.55 ng/ml cut-off (Table III). For AFP, ROC curve showed an AUC of 0.673±0.055 (P <0.01; 95% CI 0.564-0.781) with a sensitivity 66.0 per cent and specificity 59.0 per cent at a 210.72 ng/ml cut-off (Table III).

The relationship between the expression levels of ApoAI and ApoAIV with the viral load, ALT, AST, serum bilirubin, INR and albumin concentration was investigated. There was a significant positive correlation of ApoAI with viral load, INR and bilirubin in comparison to controls (Table IV). ALT, AST and albumin were negatively correlated. In controls, viral load and ALT were negatively correlated with significance. AST, INR, albumin and bilirubin had significant positive correlation. There was a significant positive correlation of ApoAIV with viral load, ALT, AST, INR, albumin and bilirubin in comparison to controls (Table IV). Tumour number and tumour size were considered to see the levels of apolipoproteins, and it was found that the levels of apolipoproteins were not dependent on tumour burden.

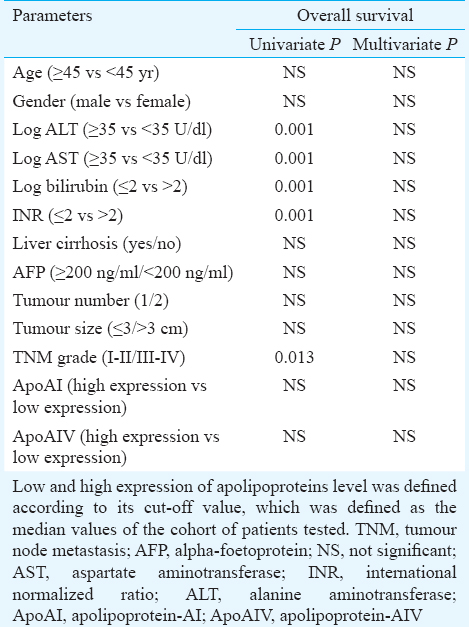
Univariate and multivariate analyses of the prognostic factors associated with HCC showed that there were no independent prognostic parameters as factors for HCC and for apolipoproteins (Table V). Multivariate analysis of expression level of apolipoproteins revealed that expression of ApoAI and ApoAIV in HCC was independent of other variables in HCC.
Discussion
HCC is a major cause of high mortality in India and Asia18. HCC involves the progressive accumulation of abnormal changes of gene and protein expression. Our study was aimed to find out the expression level of ApoAI and ApoAIV in the plasma as protein markers for HCC. Both ApoAI and ApoAIV were found to be abnormally expressed in HCC compared to controls without HCC.
Semi-quantitative densitometric image analysis of the western blot images revealed differential expression of ApoAI and ApoAIV. Levels of ApoAI were significantly higher in patients with HCC compared to controls without HCC in our study. Pleguezuelo et al7 established higher level of ApoAI expression in HCC compared to patients of liver cirrhosis without HCC. Levels of ApoAIV were significantly lower in patients with HCC compared to liver cirrhosis and chronic hepatitis without HCC in our study. Pleguezuelo et al7 also observed that ApoAIV expression levels in HCC were significant in HCC compared to liver cirrhosis and non-HCC patients, regardless of aetiology. A dysregulation in the expression of both ApoAI and ApoAIV proteins was observed in HCC cases compared to normal levels in the healthy controls. Low ApoAI was associated with advanced liver cirrhosis19. ApoAI was associated with an elevated risk of HCC while ApoAIV was associated with lower risk of HCC. Three isoforms of ApoAI were identified in murine serum where upregulation of isoform 1 was found in the serum of knockout MAT1A (−/−) mice model without any histological manifestation of liver disease20.
In another study, partial purification and protein identification analysis revealed ApoAI as a potential novel serum biomarker for screening of HCC mentioning the upregulation of ApoI fragments in the blood serum of HCC cases followed by confirmation of the same using immunoprecipitation21. Fye et al22 revealed differential expression of ApoAI among the controls and patients with liver cirrhosis and HCCs. ApoAI was also found to be closely related to vascular invasion feature of HCC23. The differentially expressed low molecular weight proteins might be potential biomarkers in an early prognostic prediction, and surveillance in the treatment for HCC. ApoAI was found to be downregulated in HCC patients compared to healthy group24.
ApoAI was significantly altered in the tumour tissue of HCC cases compared to the surrounding non-tumour tissues, and ApoAI precursor was reported as a novel candidate marker in HBV-related HCC25. ApoAI protein could be used as a diagnostic marker and target of therapy for HCC26. Teng et al27 have described that ApoAIV acts as a lipid metabolic gene and has been found to be significantly activated in HBx transgenic HCCs and human HBV-related HCCs. HBV tumourigenesis was found to be associated with metabolic syndrome28 indicating the involvement of metabolic genes such as ApoAIV. The dysregulation of lipid metabolic genes such as ApoAIV might predict the disease progression in chronic hepatitis B patients, leading to HCCs27. Protein analysis in a comparative way could be used to find out for characteristic alterations in the profile of serum of HCC patients. Differentially expressed apolipoprotein involved in HCC could provide the lead for management of candidate biomarkers for the development of diagnosis and therapy29. Sugimoto et al30 showed that ApoAIV were significantly reduced in liver cirrhosis (P <0.001) and HCC (P <0.01) patients compared to those with chronic hepatitis. Isoforms of ApoAIV might be the cause of different results in different studies31.
ROC curve analysis for ApoAI and ApoAIV suggested good specificity and sensitivity for both. Those can be used as appropriate markers and may be utilized to discriminate HCC from liver cirrhosis and liver cirrhosis from chronic hepatitis. In a study by Pleguezuelo et al7 ROC curve of both ApoAIV and ApoAI showed a sensitivity of 89 per cent and a specificity of 81 per cent for diagnosis of HCC. ApoAIV and ApoAI with high sensitivity and specificity might be used clinically as biomarkers of HCC7.
In our study, plasma levels of AFP were significantly higher in HCC cases than that of healthy controls. However, AFP levels in patients with HCC were not significantly different from disease controls without HCC. Bruix et al5 described poor sensitivity and specificity of AFP in HCC detection or diagnosis. Gupta et al31 described that the sensitivity and specificity of AFP for HCC diagnosis were 41-65 and 80-94 per cent, respectively, with a cut-off of 20 ng/ml. AFP-L3 showed better specificity (63-91.6%) and sensitivity (36-71%) for HCC diagnosis810. AFP was not associated with risk of HCC8. Poor prognosis and late diagnosis are associated with low survival rates due to a lack of curative treatment. Although AFP has been used mainly for the diagnosis of HCC, the sensitivity and specificity were found to be non-satisfactory32. Identification of the HCC-specific markers for the early prognosis or diagnosis of HCC and the discovery of potential targets for therapy of HCC are important areas of research.
The significant impairment of the hepatic function occurring during HCC can influence plasma apolipoprotein profiles as the liver plays a crucial role in lipoprotein metabolism. Circulating apolipoprotein concentration is correlated with hepatic status and a significant decrease in HCC and liver cirrhosis patients compared to controls represents an additional useful marker for a more complete assessment and monitoring of the liver function in patients with HCC and liver cirrhosis33. The specificity and sensitivity of AFP for HCC are dependent on the cut-off value above which AFP is considered positive. Increase in cut-off values decreases the sensitivity and increases the specificity.
In conclusion, the apolipoprotein profile showed various abnormalities in patients of HCC. Our study revealed various biochemical abnormalities with reference to the aberrant expression of ApoAI and ApoAIV in patients of HCC and the possibility of being used as a potential biomarker for the cases of HCC. The findings pertaining to the expression of ApoAI, AFP and ApoAIV suggest that these biochemical and molecular markers may have the potential to be used for screening cases of chronic hepatitis and those with liver cirrhosis for the early detection of HCC. ApoAI as compared to AFP and ApoAIV could be treated as a better marker for the diagnosis of HCC with better diagnostic power of sensitivity, specificity and expression level. However, the findings need to be validated in a study with large sample size.
Financial support & sponsorship: Authors thank the University Grant Commission and Delhi Government research project funding authority for financial support to carry out this research work in the PCR Hepatitis Laboratory, Department of Medicine, Maulana Azad Medical College, New Delhi
Conflicts of Interest: None.
References
- Epidemiology of hepatocellular carcinoma in India. J Clin Exp Hepatol. 2014;4(Suppl 3):S27-33.
- [Google Scholar]
- The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006;45:529-38.
- [Google Scholar]
- Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol. 2001;35:421-30.
- [Google Scholar]
- Impact of lipoproteins on the biological activity and disposition of hydrophobic drugs: Implications for drug discovery. Nat Rev Drug Discov. 2008;7:84-99.
- [Google Scholar]
- Proteomic analysis for developing new biomarkers of hepatocellular carcinoma. World J Hepatol. 2010;2:127-35.
- [Google Scholar]
- Clinical utility of AFP-L3% measurement in North American patients with HCV-related cirrhosis. Am J Gastroenterol. 2007;102:2196-205.
- [Google Scholar]
- The utility of Lens culinaris agglutinin-reactive alpha-fetoprotein in the diagnosis of hepatocellular carcinoma: Evaluation in a United States referral population. Clin Gastroenterol Hepatol. 2007;5:394-402.
- [Google Scholar]
- Apolipoproteins and their role in different clinical conditions: An overview. Indian J Biochem Biophys. 2005;42:73-80.
- [Google Scholar]
- Sample size calculations in clinical research (2nd ed). Boca Raton: Chapman & Hall/CRC; 2008.
- Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57:1651-3.
- [Google Scholar]
- Plasma proteome profiling to assess human health and disease. Cell Syst. 2016;2:185-95.
- [Google Scholar]
- Simple biochemical parameters and a novel score correlate with absence of fibrosis in patients with nonalcoholic fatty liver disease. Indian J Gastroenterol. 2015;34:281-5.
- [Google Scholar]
- Oxidation of specific methionine and tryptophan residues of apolipoprotein A-I in hepatocarcinogenesis. Proteomics. 2005;5:4964-72.
- [Google Scholar]
- Increased concentrations of apo A-I and apo A-II fragments in the serum of patients with hepatocellular carcinoma by magnetic beads-assisted MALDI-TOF mass spectrometry. Am J Clin Pathol. 2014;141:52-61.
- [Google Scholar]
- Protein profiling in hepatocellular carcinoma by label-free quantitative proteomics in two West African populations. PLoS One. 2013;8:e68381.
- [Google Scholar]
- Identification of two portal vein tumor thrombosis associated proteins in hepatocellular carcinoma: Protein disulfide-isomerase A6 and apolipoprotein A-I. J Gastroenterol Hepatol. 2011;26:1787-94.
- [Google Scholar]
- Screening low molecular weight protein biomarkers relevant to portal vein tumor thrombi in serum of patients with hepatocellular carcinoma. Zhonghua Gan Zang Bing Za Zhi. 2007;15:498-502.
- [Google Scholar]
- Proteome analysis of hepatocellular carcinoma by laser capture microdissection. Proteomics. 2006;6:538-46.
- [Google Scholar]
- A strategy for the comparative analysis of serum proteomes for the discovery of biomarkers for hepatocellular carcinoma. Proteomics. 2003;3:601-9.
- [Google Scholar]
- A biphasic response pattern of lipid metabolomics in the stage progression of hepatitis B virus X tumorigenesis. Mol Carcinog. 2016;55:105-14.
- [Google Scholar]
- The association between metabolic syndrome and hepatocellular carcinoma: Systemic review and meta-analysis. J Clin Gastroenterol. 2014;48:172-7.
- [Google Scholar]
- Proteomic analysis of sera from hepatocellular carcinoma patients after radiofrequency ablation treatment. Proteomics. 2005;5:4287-95.
- [Google Scholar]
- Serum protein isoform profiles indicate the progression of hepatitis C virus-induced liver diseases. Int J Mol Med. 2013;31:943-50.
- [Google Scholar]
- Test characteristics of alpha-fetoprotein for detecting hepatocellular carcinoma in patients with hepatitis C. A systematic review and critical analysis. Ann Intern Med. 2003;139:46-50.
- [Google Scholar]
- Serum proteomics and biomarkers in hepatocellular carcinoma and chronic liver disease. Clin Cancer Res. 2008;14:470-7.
- [Google Scholar]
- Lipoprotein(a) as a potential marker of residual liver function in hepatocellular carcinoma. Indian J Med Paediatr Oncol. 2011;32:71-5.
- [Google Scholar]




