Translate this page into:
Evaluation of an immunochromatographic test for discrimination between Mycobacterium tuberculosis complex & non tuberculous mycobacteria in clinical isolates from extra-pulmonary tuberculosis
Reprint requests: Dr T.N. Dhole, Professor & Head, Department of Microbiology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow 226 014, India e-mail: tndhole@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Accurate diagnosis of tuberculosis (TB) is crucial to facilitate early treatment of the patients, and to reduce its spread. Clinical presentation of Mycobacterium tuberculosis complex (MTBC) and non tuberculous mycobacteria (NTM) may or may not be the same, but the treatment regimen is always different for both the infections. Differentiation between MTBC and NTM by routine laboratory methods is time consuming and cumbersome. This study was aimed to evaluate an immunochromatographic test (ICT), based on mouse monoclonal anti-MPT64, for simple and rapid discrimination between MTBC and NTM in clinical isolates from extra-pulmonary tuberculosis cases.
Methods:
A total of 800 clinical samples were collected from patients suspected to have extra-pulmonary tuberculosis. Preliminary diagnosis has been done by direct Ziehl–Neelsen (ZN) staining followed by culture in BACTEC system. A total of 150 clinical isolates, which were found positive in BD 460 TB system during September 2009 to September 2010 were selected for the screening by ICT test. p-nitro-α-acetylamino- β-hydroxy propiophenone (NAP) test was performed for differentiation of MTBC and NTM. M. tuberculosis complex was further confirmed by IS6110 PCR of BACTEC culture positive isolates, this served as the reference method for MTBC identification and comparative evaluation of the ICT kit.
Results:
Of the 150 BACTEC culture positive isolates tested by ICT kit, 101 (67.3%) were found positive for MTBC and remaining 49 (32.7%) were considered as NTM. These results were further confirmed by IS6110 PCR that served as the reference method for detection of MTBC. H37Rv reference strain was taken as a control for ICT test and IS6110 PCR. The reference strain showed the presence of MPT64 antigen band in the ICT test. Similar bands were formed in 101 of 102 MTBC isolates tested, proving 99.1 per cent sensitivity and no bands were detected in 48 (100%) NTM isolates tested, proving 100 per cent specificity of the ICT kit.
Interpretation & conclusions:
Our findings show that ICT test can be used on direct culture positive specimens. It does not require any special equipment, is simple and less time consuming. It can easily discriminate between MTBC and NTM and thus can help in appropriate management of tuberculosis.
Keywords
Immunochromatographic test
Mycobacterium tuberculosis complex
non tuberculous mycobacteria
tuberculosis

Tuberculosis (TB) is one of the major causes of morbidity and mortality worldwide. In India, about 1.8 million new cases of TB are reported annually, that account for a fifth of new cases in the world - a greater number than in any other country1. The situation is further worsened by the increasing number of drug-resistant cases of TB. Thus, there is a need for rapid and correct identification of mycobacteria and rapid drug sensitivity testing for effective treatment of the disease. Strategies used for the clinical management of patients with Mycobacterium tuberculosis complex (MTBC) and non tuberculous mycobacteria (NTM) are different, therefore, prompt detection, isolation, and discrimination is necessary for suitable management23. Although conventional biochemical methods are able to identify mycobacterial species; but these are tedious, time-consuming and require elaborate safety precautions. The recent objective of World Health Organization (WHO) is to reduce the time for culture, identification, and drug resistance detection to as short as two days by employing Line probe assays4. Although molecular methods of identification are very accurate and reliable, but require a specialized set up, sophisticated and expensive equipment, trained laboratory personnel and are expensive for resource-poor countries5. In recent years, major advances in the understanding of the genetic structure of mycobacteria have been achieved. Various genetic probes and amplification systems for diagnosis of TB have been developed, and several of these are available as commercial kits for direct detection and identification of M. tuberculosis in clinical specimens67. Early and reliable identification of mycobacteria may spare patients from unnecessary treatments in cases of NTM8. Studies have revealed that the M. tuberculosis protein 64 (MPT 64) is specific for MTBC, including M. tuberculosis, M. africanum, M. bovis, and some, although not all, substrains of M. bovis BCG59–12. The MPT 64 is a M. tuberculosis complex specific antigen secreted during the bacterial growth, and is an excellent antigen for the identification of MTBC912. This study was carried out to evaluate clinical usefulness of immunochromatographic test (ICT) kit based on mouse monoclonal anti-MPT 64 for simple discrimination between M. tuberculosis complex and non tuberculous mycobacteria in clinical isolates from patients with extra-pulmonary tuberculosis.
Material & Methods
This prospective study was undertaken at Mycobacteriology Laboratory, Department of Microbiology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India. Specimens were collected from Kasturaba Chest Hospital, Department of Pulmonary Medicine, Chhatrapti Shahuji Maharaj Medical University, Lucknow, India, and from various wards of Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India. A total 800 clinical specimens (2-10 ml) as lymph node aspirate and cold abscesses, pleural fluid, cerebrospinal fluid (CSF), synovial fluid, ascitic fluid, urine, gastric aspirate, pus, bone marrow aspirates, wound swabs and biopsy materials were collected from suspected cases of extra-pulmonary tuberculosis during September 2009 to September 2010. The study was approved by the institutional ethics committee of Chhatrapati Shahuji Maharaj Medical University, Lucknow, India. The age of patients varied from 12-65 yr and included both male and female population in urban and rural settlements. Written informed consent was obtained from the subjects before enrollment into the study.
Microbiological analysis for M. tuberculosis: For decontamination of specimens from normal bacterial flora, specimens were treated by N-acetyl- L- cysteine-NaOH Method13. Smears were stained with Ziehl-Neelsen (ZN) for detection of acid-fast bacilli (AFB). For the BACTEC method (Becton Dickinson, Cockeysville, MD, USA), 0.5 ml of processed specimen was inoculated into the BACTEC 12B vial supplemented with PANTA (a mixture of five different antibiotics: polymyxin B, amphotericin B, nalidixic acid, trimethoprim and azlocillin) and incubated at 37°C. Readings were taken twice a week for the first two wk and once a wk thereafter for culture positivity for 8 wk. After 8 wk if the growth index (GI) was zero, the specimens were considered as negative. AFB smears were made from vials with a GI of 50-100, and further identification of MTBC was done by the BACTEC NAP (p-nitro-α-acetylamino-β-hydroxy propiophenone) differentiation test (Becton Dickinson, Sparks, MD, USA)14.
Molecular confirmation of M. tuberculosis complex by IS6110 PCR: The final confirmation of MTBC was done by IS6110 PCR of BACTEC culture positive isolates. Extraction of DNA was done by the cetyl-tri-methyl-ammonium bromide (CTAB)-phenol chloroform extraction method15. Identification of MTBC was done by using a specific pair of primers designed to amplify an insertion sequence IS6110 (~123-bp). The sequence of these FP1 and RP2 primers were: 5’-CCT GCG AGC GTA GGC GTC GG3’ and 5’ CTC GTC CAG CGC CGC TTC GG 3’, respectively16. PCR reaction mixture (20 μl) contained 2× Pyrostart Fast PCR Master Mix (Fermatas, India), 10 pmole of each primer (SBS Gentech Co. Ltd., India) and 5 μl of extracted DNA. Amplification was carried out in a thermal cycler (MJ Research ,PTC-100 Thermal Cycler , GMI, Inc , USA ), which involved 40 cycles of denaturation at 94°C for 2 min, annealing of primers at 68°C for 2 min, and primer extension at 72°C for 1 min. The amplified products were separated on 2 per cent agarose gels, visualized on a UV- light transilluminator (Bangalore Genei, Bangalore, India). The presence of 123bp fragment indicated a positive test for M. tuberculosis complex. Positive control included the DNA of H37Rv reference strain and negative control included PCR grade water (Fig. 1).
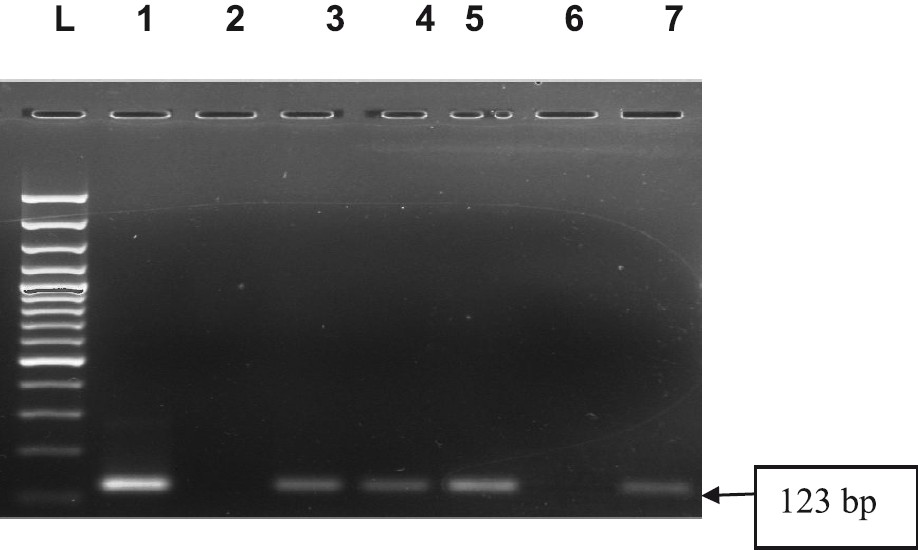
- IS6110PCR-based detection of M. tuberculosis complex. Electrophoretic separation of the amplicon into 2% agarose gel is documented across lanes 1-7. The presence of a 123 bp amplicon in lanes 3, 4, 5, 7 indicated the presence of the target while the absence of the amplicon in lane 6 showed absence of the target. Lane 2 was negative control and lane 1 was positive control (H37Rv). L-Ladder 100 bp was well shown.
ICT tuberculosis test: A volume of 100 μl of broth from BACTEC culture was added to the well of SD TB Ag MPT 64 Rapid ICT kit cassette (Standard Diagnostics Ltd., Korea). Inoculated ICT cassettes were kept at room temperature for 20 min and were examined for the presence of control and test bands. Appearance of band in the ‘C’ region confirmed the validity of test. Additional appearance of Band in the ‘T’ region was interpreted as positive for MPT 64 antigen (Fig. 2). No band in the ‘C’ region was interpreted as invalid test. Standard reference strain H37Rv was used as positive control.
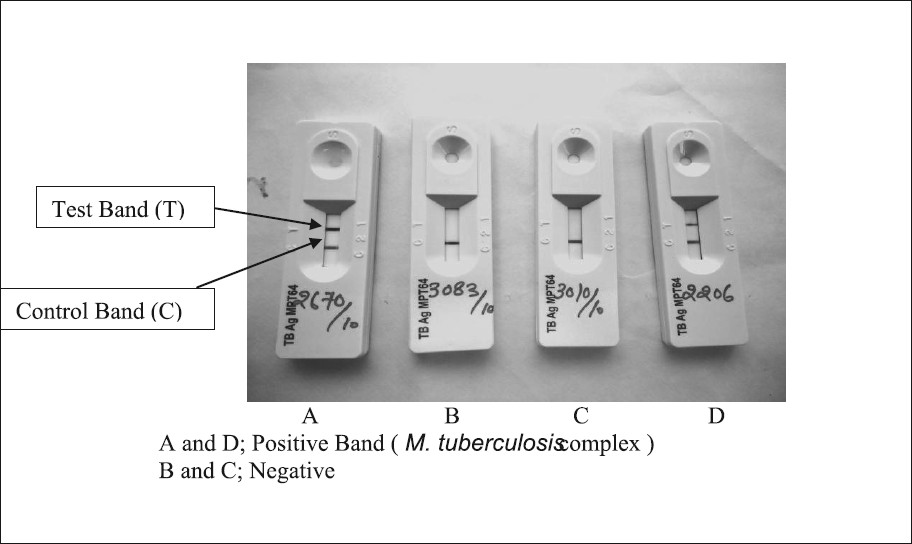
- Identification M. tuberculosis complex by MPT64 Rapid ICT kit.
Statistical analysis: Data were analyzed using SPSS 15.0 (Statistical Package for the Social Sciences, Chicago, IL, USA) for Windows. Validity of ICT test was calculated by sensitivity and specificity. Sensitivity was calculated as [Tp/(Tp +Fn)] × 100; specificity was calculated as [Tn/(Tn + Fp)] × 100; Tp =total number of positives; Tn =total number of negatives; Fp= total number of false positive , Fn = total number of false negative, respectively.
Results
Of the 800 samples tested, 150 (18.7%) were found to be positive by BACTEC culture method. Of these 150 BACTEC culture positives, 20 (13.2%) were found smear positive for AFB. All BACTEC culture positive cases were examined by NAP test for differentiation between MTBC and NTM, and 102 (68%) were positive for MTBC by NAP test, remaining 48 (32%) were considered as NTM. Final confirmation of MTBC in BACTEC positive isolates was done by IS6110 PCR. All the 102 NAP positive isolates were found positive as MTBC and remaining 48 were negative by IS6110 PCR (Fig. 3). ICT test was performed on 150 BACTEC positive isolates on 1st and 5th day of BACTEC culture positive vials. In the ICT test, the 5th day BACTEC culture positive vials were able to give visibly more intense band as compared to the 1st day BACTEC culture positive vials that could be attributed to low antigen concentration on initial day of inoculation. Control band in the ‘C’ region of ICT test cassette was seen in all the 150 samples tested (Fig. 2) and no test was reported as invalid. H37Rv control strain showed the appearance of band in the test region (‘T’) confirming the ability of ICT test to detect the MPT64 antigen. A total of 101 of 150 (67.3%) isolates tested showed dark band in the test region (‘T’) confirming the presence of MPT 64 antigen and thus presence of MTBC. One sample which was found positive for MTBC by NAP test but was negative by the ICT might be related to the low-level expression of the antigen. The remaining 49 (32.7%) isolates which were identified as NTM by NAP test, showed no band formation, indicating the absence of MPT64 antigen in these isolates. The sensitivity and specificity of the ICT kit was found to be 99.1 and 100 per cent respectively (Table).
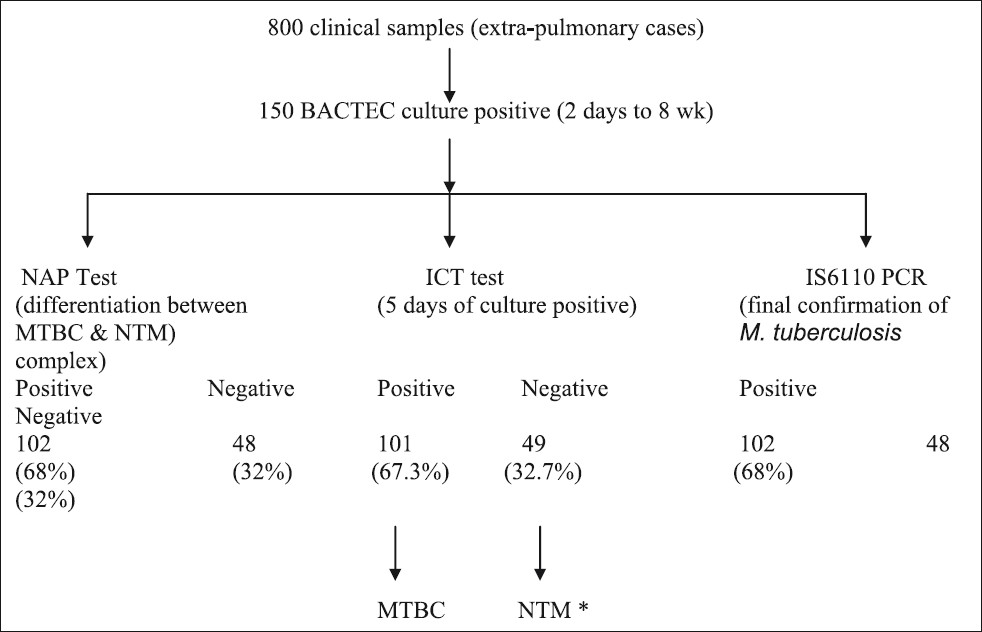
- Comparison of methods for detection of M. tuberculosis complex in extra-pulmonary tuberculosis cases.*NAP test and IS6110 PCR negative isolates were included in non tuberculosis mycobacteria. MTBC, Mycobacterium tuberculosis complex; NTM, non tuberculous mycobacteria.

Discussion
M. tuberculosis poses diagnostic and therapeutic problems due to low sensitivity of the diagnostic tools available for its identification and discrimination with NTM. Conventional culture is time consuming and lacks sensitivity; smear for AFB is rapid but the sensitivity has not been yet evaluated and does not differentiate between MTBC and NTM17. The diagnostic delay can affect treatment18. Rapid identification of mycobacteria is important and a simple, sensitive, and specific identification method is required. Conventional methods like direct staining of a colony is simple and fast but does not discriminate between M. tuberculosis and NTM, whereas traditional biochemical tests take a long time. Newer techniques like chemiluminescent DNA probes, nucleic acid amplification, high-performance liquid chromatography and sequencing of 16S rRNA genes are more sophisticated methods but are not cost-effective and require expensive equipment19–21. Attorri et al22 showed that M. tuberculosis often exhibits serpentine cording when grown in liquid medium, NTM can form true cords in liquid culture but do so rarely, despite the fact that many species contain the cell wall glycolipid that mediates cord formation. Previous studies23–25 utilized cord formation for the cost-effective employment of DNA probes for the identification of Mycobacterium species. Chihota et al5 reported the cost of organism identification per positive culture on BACTEC as US$35.94 using standard biochemical tests, US$15.49 for anti-MPB64 assay and US$2.28 for cording. Cost-effective analytical studies26 of SD MPT64 TB Ag ICT test, other rapid molecular methods and culture combined with conventional biochemical tests have shown SD MPT 64 TB Ag ICT as more economical than the other two methods. Further, ICT requires only 20 min of analysis as compared to five days for NAP test. Ismail et al27 reported sensitivity, specificity, positive and negative predictive values of the SD AgMPT64 kit to be 97, 100, 100 and 92 per cent, respectively. Using the same kit, Chihota et al5 reported sensitivity and specificity of 100 per cent in a total of 108 broth cultures. In the present study, the sensitivity and specificity of ICT kit were 99.1 and 100 per cent, respectively. MTBC isolates showed same band similar to H37Rv control strain.
In conclusion, ICT test can be used on direct culture positive specimens, it does not require any special equipment. It can discriminate between MTBC and NTM. The low cost, simplicity, rapidity, high sensitivity and high specificity for the MPT 64 antigen detection make the ICT as a useful diagnostic tool for diffentiation between MTBC and NTM diagnosis and can help in appropriate management of tuberculosis.
Acknowledgment
This work was supported by research grant from Indian Council of Medical Research, New Delhi. Authors thank Shri Hariom Verma and Ms. Jyoti Umaro for technical support during the research work.
Conflict of interest: The authors declare that they have no conflict of interest.
References
- RNTCP. Status TB Report, 2010. New Delhi: Central TB Division. Directorate General of Health Services, Ministry of Health and Family Welfare; Available from: www.tbcindia.org
- New simple and rapid test for culture confirmation of Mycobacterium tuberculosis complex: a multicenter study. J Clin Microbiol. 2002;40:908-12.
- [Google Scholar]
- Evaluation of an immunochromatographic assay kit for rapid identification of Mycobacterium tuberculosis complex in clinical isolates. J Clin Microbiol. 2009;47:481-4.
- [Google Scholar]
- World Health Organization. Use of liquid TB culture and drug susceptibility testing (DST) in low and medium income settings. Summary report of the expert group meeting on the use of liquid culture media. 2007.
- [Google Scholar]
- Liquid vs. solid culture for tuberculosis: performance and cost in a resource-constrained setting. Int J Tuberc Lung Dis. 2010;14:1024-31.
- [Google Scholar]
- Current situations on identification of nontuberculous mycobacteria. J Biomed Lab Sci. 2009;21:1-6.
- [Google Scholar]
- Utility of immunochromatographic assay for detecting Mycobacterium tuberculosis from positive BACTEC MGIT 960 cultures. J Biomed Lab Sci. 2010;22:64-8.
- [Google Scholar]
- Simple and rapid identification of the Mycobacterium tuberculosis complex by immunochromatographic assay using anti-MPB64 monoclonal antibodies. J Clin Microbiol. 1999;37:3693-7.
- [Google Scholar]
- Properties of proteins MPB64, MPB70, and MPB80 of Mycobacterium bovis BCG. Infect Immun. 1986;52:293-302.
- [Google Scholar]
- Evidence for absence of the MPB64 gene in some substrains of Mycobacterium bovis BCG. Infect Immun. 1993;61:1730-4.
- [Google Scholar]
- Isolation and partial characterization of major protein antigens in the culture fluid of Mycobacterium tuberculosis. Infect Immun. 1991;59:372-82.
- [Google Scholar]
- Nontuberculous mycobacterial infections: a clinical review. Infection. 2004;32:257-70.
- [Google Scholar]
- Comparison of C(18)-carboxypropylbetaine and standard N-acetyl-L-cysteine-NaOH processing of respiratory specimens for increasing tuberculosis smear sensitivity in Brazil. J Clin Microbiol. 2002;40:3219-22.
- [Google Scholar]
- BACTEC 460 TB system. Products and procedure manual. Sparks, MD, USA: Becton Dickinson Microbiology System; 1996.
- Extraction of Mycobacterium tuberculosis DNA: a question of containment. J Clin Microbiol. 2005;43:2996-7.
- [Google Scholar]
- Polymerase chain reaction amplification of a repetitive DNA sequence specific for Mycobacterium tuberculosis. J Infect Dis. 1990;161:977-81.
- [Google Scholar]
- Improved detection of Mycobacterium tuberculosis in Peruvian children by use of a heminested IS6110 polymerase chain reaction assay. Clin Infect Dis. 2003;36:16-23.
- [Google Scholar]
- Mycobacterium growth indicator tube testing in conjunction with the AccuProbe or the AMPLICOR-PCR assay for detecting and identifying mycobacteria from sputum samples. J Clin Microbiol. 1997;35:2022-5.
- [Google Scholar]
- Assessment of morphology for rapid presumptive identification of Mycobacterium tuberculosis and Mycobacterium kansasii. J Clin Microbiol. 2000;38:1426-9.
- [Google Scholar]
- Can cord formation in BACTEC MGIT 960 medium be used as a presumptive method for identification of M. tuberculosis complex? Indian J Tuberc. 2010;57:75-9.
- [Google Scholar]
- Cord formation in BACTEC 7H12 medium for rapid, presumptive identification of Mycobacterium tuberculosis complex. J Clin Microbiol. 1990;28:1451-3.
- [Google Scholar]
- Reliability of cord formation in BACTEC media for presumptive identification of mycobacteria. J Clin Microbiol. 1993;31:2533-4.
- [Google Scholar]
- MPT 64 antigen detection for rapid confirmation of M. tuberculosis isolates. BMC Res Notes. 2011;4:79.
- [Google Scholar]
- Use of an immunochromatographic kit for the rapid detection of Mycobacterium tuberculosis from broth cultures. Int J Tuberc Lung Dis. 2009;13:1045-7.
- [Google Scholar]




