
Translate this page into:
Epidemiology & attributing factors for chronic kidney disease: Finding from a case–control study in Odisha, India
For correspondence: Dr Subrata Kumar Palo, ICMR-RMRC, Nalco Square, Bhubaneswar, Odisha 751 023, India e-mail: drpalsubrat@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Chronic kidney disease (CKD) is one of the leading causes of mortality in developing countries, however, evidence from some geographical areas of India is scantly available on its risk factors. Other than diabetes and hypertension, several personal and environmental factors are also associated with CKD.
Methods:
A population-based case–control study was conducted over a period of 12 months in two high CKD reporting districts of Odisha, India. A total of 236 participants, 1:2 age- and sex-matched cases (83):controls (153), were included. Various factors were modelled with univariate and multivariable conditional logistic regression and analyzed using the Bayesian method in STATA SE v.12.
Results:
Among the study cases, about 81 per cent were male and about 25 per cent were aged <40 yr. CKD-associated risk factors were hypertension for more than five years [adjusted odds ratio (aOR)=4.24; 95% credible interval: 1.23-10.05], scheduled tribe/caste (aOR=2.81; 1.09-5.95), use of tube well/bore well water for drinking (aOR=1.21; 1.02-1.43), consumption of locally made alcohol (aOR=1.09; 1.02-1.17) and eating red meat and vegetarian diet with (aOR=1.24; 1.12-1.39) and (aOR=1.09; 1.04-1.14), respectively.
Interpretation & conclusions:
The presence of CKD among younger age groups and association of multiple factors including personal and environmental suggest for more research to establish the cause and effect relation of these factors.
Keywords
Case–control
chronic kidney disease
India
Odisha
risk factor

Over the years, chronic kidney disease (CKD) has emerged as a major public health problem and a significant contributor to the overall non-communicable disease burden globally12. Worldwide, the prevalence of CKD varies from eight to 16 per cent representing over 750 million cases, of which 78 per cent (387.5 million) are from low-middle-income countries (LMICs)13. According to a systematic analysis study for global burden of disease, CKD contributes significantly to global morbidity and also as a risk factor to cardiovascular disease4. Limited awareness on CKD in most LMICs has caused a large proportion of patients seeking medical care at a later stage, thereby creating a major burden on health system. The true magnitude of CKD/end-stage renal disease (ESRD) in India is largely unknown.
Other than diabetes and hypertension, factors such as occupational stress, exposure to heat and chemicals and medicinal side effects have also been found to contribute to CKD [called CKD of unknown aetiology (CKDu)]5. Over the years, there have been increasing reports of CKD cases from the State of Odisha6, however, limited research exploring the contributing factors from this region is available. Hence, the present study aimed to explore various contributing factors for CKD, particularly in the State of Odisha, eastern India.
Material & Methods
A population-based case–control study was carried out over a period of 12 months (from May 2016 to April 2017) in two districts (Jajpur and Keonjhar) of Odisha, India. Both the districts were purposively selected considering the increased reporting of CKD cases and concern by the State health system. The study was approved by the Institutional Ethics Committee of Indian Institute of Public Health, Bhubaneswar, and State Research and Ethics Committee, Department of Health and Family Welfare, Government of Odisha, India. Written informed consent was also obtained from each participant before recruiting them for study.
A total of 496 CKD cases from both the districts were line listed based on the patient information collected from hospital records of each of the district headquarter hospitals, magistrate office, and four major tertiary referral hospitals (one government and three private). Cases were geographically mapped to understand their distribution in both the study districts. Block- and village-wise list of cases was prepared (case villages) and their adjacent villages having no reported cases were enlisted as control villages. Due to limited literature available from the study region, previously published CKD prevalence data from other parts of India were used to compute the sample size. Considering diabetes as one of the leading factors for CKD in India [odds ratio (OR)=2.5]7, anticipated proportion of controls with diabetes was 40 per cent and CKD cases with diabetes was 62.5 per cent. The sample size of cases was determined to be 64 (assuming 80 per cent power of the study, 95 per cent two-sided confidence level and the ratio of controls to cases was 2:1). Considering 20 per cent non-response rate, the minimum sample size for cases was estimated to be 80. In this study, 83 cases from 13 villages were selected randomly among the total line listed cases. Out of the total 166 controls contacted, collect complete information could be collected from 153 participants from 12 villages. For two case villages, only one control village could be identified after following the selection criteria.
For study purpose, ‘CKD case’ was defined as a person already diagnosed as having CKD or ESRD from a hospital with kidney damage and a glomerular filtration rate (GFR) of <60 ml/min/1.73 m2 for three months or more irrespective of the cause8. To ascertain their case status, prescriptions were reviewed during data collection. Controls were selected after age (±3 yr) and sex matching. Matched persons with no evidence of CKD and tested negative for urine albumin testing (done during the study) were included as controls. Participants having symptoms of weight loss, poor appetite, swollen ankles or feet, shortness of breath, blood in urine, increased frequency in voiding, difficulty in sleeping, skin itching, muscle cramps and other known illnesses were excluded as controls.
Data collection: Primary data were collected from the cases and controls using a standardized pre-designed, pre-tested and validated schedule in the local vernacular language (Odia). Experts including nephrologists, public health and environmental scientists were consulted while finalizing the tools. Tools were validated using Cronbach alpha value of 0.78 before data collection by trained researchers. The schedule had three major constructs, namely (i) sociodemographic information: age, gender, religion, marital status, education, dietary habits, present occupation, poverty level and insurance status; (ii) exposure assessment: agriculture, radiation, industry and heat, and (iii) disease history: a history of past illnesses, present health conditions and health facilities visited.
Data analysis: For analysis purpose, the duration of exposure to various factors was used as a covariate than only the presence or absence of it. Exposure to smoking and alcohol was calculated as cumulative exposure (amount consumed each time×frequency in months), consumption of vegetable and meat as servings per month (number of servings per day×30 days) and exposure to sun at workplace was estimated as ‘hours per day’. Recordings of hypertension, diabetes and acid peptic disease were done as present or absent through clinical history, prescription and medication history and were categorized as ‘never’, ‘<five years’ and ‘>=five years’ for analysis.
Categorical variables were expressed as proportion and frequencies, while quantitative variables were expressed as mean and standard deviation (SD). The risk factors were modelled with univariate and multivariable conditional logistic regression using the Bayesian method9. A normal prior distribution [N(m,s)] was used to estimate the log (OR) in the conditional logistic regressions. The results from previous studies were used to provide informative Bayesian priors and define the values of m and s in the prior log-odds distribution for hypertension, diabetes1011 and educational status12. For the univariate analysis, the priors were less informative [normal distribution N (mean±SD) for the log-OR ¼ N(0; 10)]. In the multivariable analysis, prior distributions were derived from the OR confidence interval of the references. For other variables, non-informative prior method was used.
For each potential predictor the study results were presented as OR with a 95 per cent credible interval. Statistical analysis was carried out using the Bayesian method in STATA SE 12 (STATA Corp., Texas, USA). The estimations were made using Markov chain Monte Carlo with Gibbs sampling. For each model, 100,000 iterations were drawn after a burn-in of 5,000 updates, and convergence was checked using trace plots of the sampled values for each iteration (Fig. 1). The results of conditional logistic regression model using ‘frequentist’ method are provided in Supplementary Table I. Both the models were compared based on their Bayesian information criteria, which indicates smaller the value, better is the fitting of the model. A Directed Acyclic Graph (DAG) to depict the possible linkage between the risk factors using ‘ggdag’ package was created from R v 3.5.2 (R Software, Vienna).
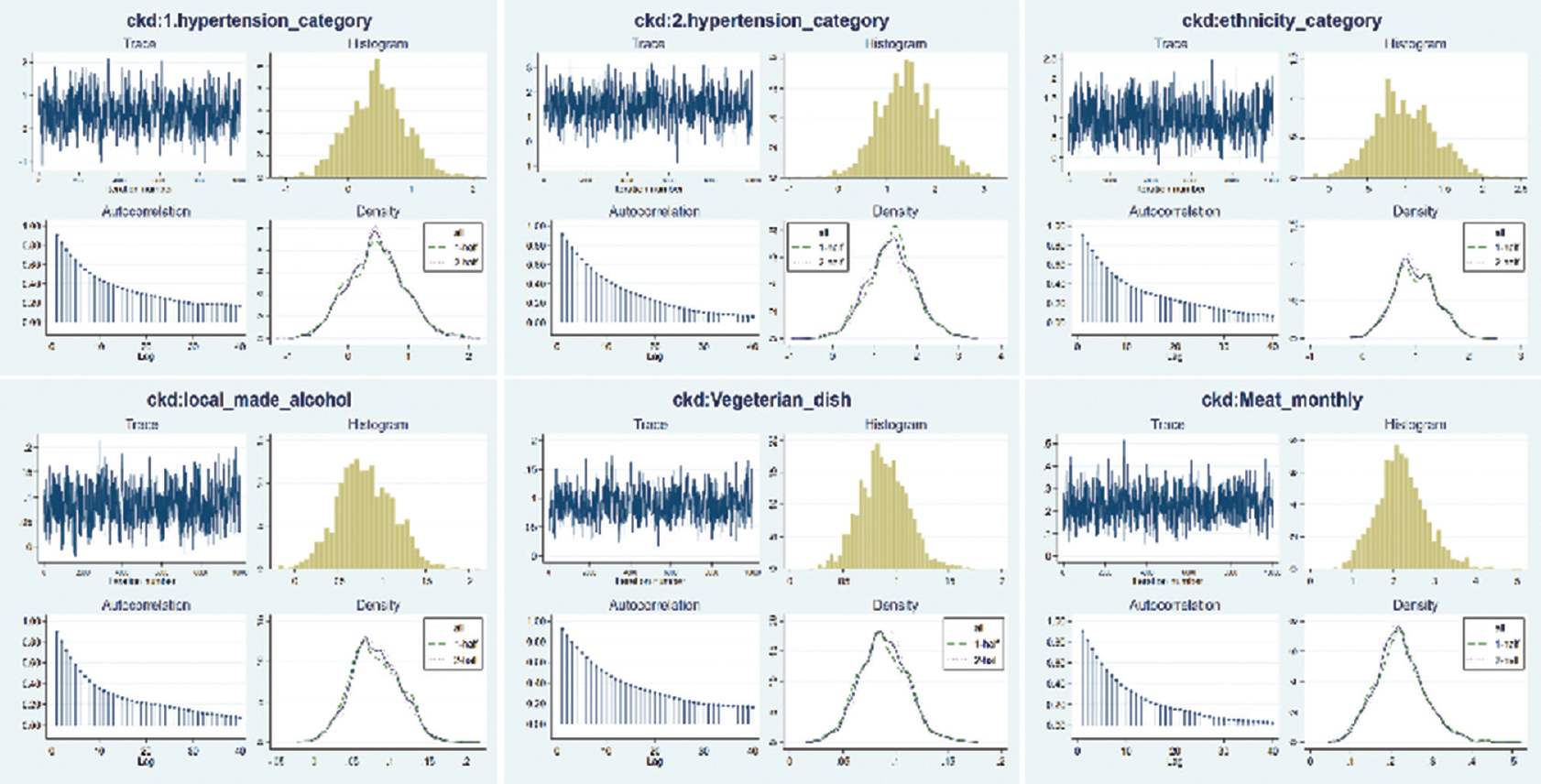
- Posterior distribution of the Bayesian model.
| Variables | Unadjusted OR | 95% CI | Adjusted OR | 95% CI |
|---|---|---|---|---|
| Education | ||||
| Illiterate | Reference | |||
| Primary | 0.48 | 0.24-0.97 | ||
| Secondary and above | 0.52 | 0.24-1.12 | ||
| Socioeconomic status | ||||
| Above poverty line | Reference | |||
| Below poverty line | 0.77 | 0.45-1.31 | ||
| Ethnicity | ||||
| Others | Reference | Reference | ||
| Schedule Caste/Tribe | 2.21 | 1.24-3.97 | 2.55 | 1.13-5.75* |
| Joint pain | ||||
| Never | Reference | |||
| Since last 5 yr | ||||
| Since last 5-10 yr | ||||
| Diabetes | ||||
| Never | Reference | |||
| Since last 5 yr | 1.96 | 0.8-4.76 | ||
| Since last 5-10 yr | 0.96 | 0.36-2.52 | ||
| Hypertension | ||||
| Never | Reference | Reference | ||
| Since last 5 yr | 1.53 | 0.79-2.98 | 1.53 | 0.61-3.82 |
| Since last 5-10 yr | 2.92 | 1.34-6.36 | 3.78 | 1.27-11.26* |
| Acid peptic disease | ||||
| Never | Reference | |||
| Since last 5 yr | 0.79 | 0.39-1.59 | ||
| Since last 5-10 yr | 1.69 | 0.79-3.59 | ||
| Family history of diabetes | ||||
| No | Reference | |||
| Yes | 0.92 | 0.45-1.66 | ||
| Family history of hypertension | ||||
| No | Reference | |||
| Yes | 0.62 | 0.32-1.19 | ||
| Chewing tobacco (Numbers per week) | 0.99 | 0.99-1.00 | ||
| Smoking (Since, in yr) | 0.95 | 0.88-1.02 | ||
| Local alcohol (Since, in yr) | 1.04 | 1.01-1.08 | 1.08 | 1.02-1.16* |
| Leafy green vegetables | 0.91 | 0.78-1.06 | ||
| Chicken per month | 0.96 | 0.88-1.04 | ||
| Veg dish per month | 1.07 | 1.04-1.11 | 1.08 | 1.04-1.13* |
| Red meat per month | 1.26 | 1.14-1.39 | 1.21 | 1.09-1.35* |
| Exposure to sun (reference - No) | 1.53 | 0.71-3.27 | ||
| Source of drinking water | ||||
| Well/river | Reference | Ref | ||
| Tube well/boring | 2.28 | 1.19-4.38 | 1.19 | 1.01-1.41* |
P*<0.05; Akaike Information Criteria for the model was 111.16 and Bayesian Information Criteria was 135.26. OR, odds ratio; CI, confidence interval
Results
The mean age of the 83 cases was 49±10.62 yr, and 20 (24.2%) were ≤40 yr. About 81 per cent of cases were male. A significant difference with respect to marital status (P=0.019), ethnicity (P=0.009), current occupation status (P<0.001) and source of drinking water (P=0.003) was observed between case and control groups. Among the cases, 47.4 per cent were unemployed mostly because of their present disease condition. A significant difference was observed with respect to family history of CKD (P=0.001) and medical conditions like joint pain (P=0.023) and hypertension (P=0.011) between cases and control groups. Difference in terms of education, socio-economic status, family history of hypertension and diabetes and personal habits such as smoking, drinking alcohol and disease conditions such as diabetes and acid peptic disease were not found to be significant between the groups. Details of socio-demographic characteristics of the study participants and their medical history are presented in Tables I and II, respectively.
| Variables | Cases (n=83) (%) | Controls (n=153) (%) | Total (n=236) (%) |
|---|---|---|---|
| Age (yr) | |||
| ≤40 | 24.2 | 25.3 | 24.6 |
| 40-60 | 56.9 | 60.2 | 58.1 |
| >60 | 18.9 | 14.5 | 17.4 |
| Gender | |||
| Male | 81.1 | 84.3 | 82.2 |
| Marital status | |||
| Single | 7.2 | 1.3 | 3.4* |
| Married | 85.5 | 95.4 | 91.9 |
| Widow/er | 7.3 | 3.3 | 4.7 |
| Ethnicity | |||
| Schedule caste | 22.9 | 15.1 | 17.8** |
| Schedule tribe | 21.7 | 10.5 | 14.4 |
| Others | 55.4 | 74.4 | 67.8 |
| Highest education | |||
| Illiterate | 47.0 | 34.6 | 39.1 |
| Primary completed | 28.9 | 37.2 | 34.3 |
| Secondary completed | 20.5 | 26.1 | 24.1 |
| Tertiary and above | 3.6 | 2.1 | 2.5 |
| Socio-economic status | |||
| Above poverty line | 50.6 | 44.4 | 46.6 |
| Below poverty line | 49.4 | 55.6 | 53.4 |
| Current occupation | |||
| Paid work | 28.2 | 50.3 | 42.4*** |
| Self-employed | 13.1 | 19.3 | 16.5 |
| Non-paid work | 2.2 | 2.6 | 2.5 |
| Home maker | 9.1 | 17.3 | 13.6 |
| Unemployed (health issue) | 47.4 | 10.5 | 20.8 |
| Current source of drinking water | |||
| Tubewell/borewell | 80.7 | 62.3 | 68.7** |
| Well/river | 19.3 | 32.7 | 31.3 |
| Exposure to sun at work | 69.9 | 75.9 | 72.0 |
P *<0.05, **<0.01, ***<0.001
| Medical history | Cases (n=83) (%) | Controls (n=153) (%) | Total (n=236) (%) |
|---|---|---|---|
| Joint pain | |||
| Never | 42.1 | 43.8 | 43.2 |
| <5 yr | 43.4 | 40.5 | 41.5* |
| ≥5 yr | 14.5 | 15.7 | 15.3 |
| Diabetes | |||
| Never | 77.1 | 81.7 | 80.1 |
| <5 yr | 12.1 | 6.6 | 8.5 |
| ≥5 yr | 10.8 | 11.7 | 11.4 |
| Hypertension | |||
| Never | 55.4 | 71.9 | 66.1 |
| <5 yr | 24.1 | 18.9 | 20.8** |
| ≥5 yr | 20.5 | 9.1 | 13.1** |
| Acid peptic disease | |||
| Never | 28.9 | 28.1 | 28.4 |
| <5 yr | 42.2 | 54.2 | 50.0 |
| ≥5 yr | 28.9 | 17.7 | 21.6 |
| Family history of medical conditions | |||
| Family history of diabetes | 28.4 | 29.5 | 28.4 |
| Family history of hypertension | 23.5 | 33.6 | 29.2 |
| Family history of CKD | 9.9 | 0.01 | 3.8** |
| Personal habits | |||
| Smoking | 63.9 | 82.4 | 75.8 |
| Chewing tobacco | 30.1 | 28.2 | 28.9 |
| Local alcohol | 19.3 | 11.8 | 14.4 |
| Any alcohol | 34.0 | 43.4 | 37.3 |
P *<0.05, **<0.01. CKD, chronic kidney disease
During the preceeding ten years of this study, borewell water as a drinking source among the cases had increased from 14.5 to 24.1 per cent and the same among controls had reduced from 10.5 to 5.2 per cent. CKD was found to be significantly associated among borewell/tubewell water users as compared to well/river water (Armitage trend test, P=0.003). This changing trend on usage of different sources for drinking water over the years (last 20 yr for tubewell and river water and last 10 yr for borewell water) is appended in Fig. 2A-C.
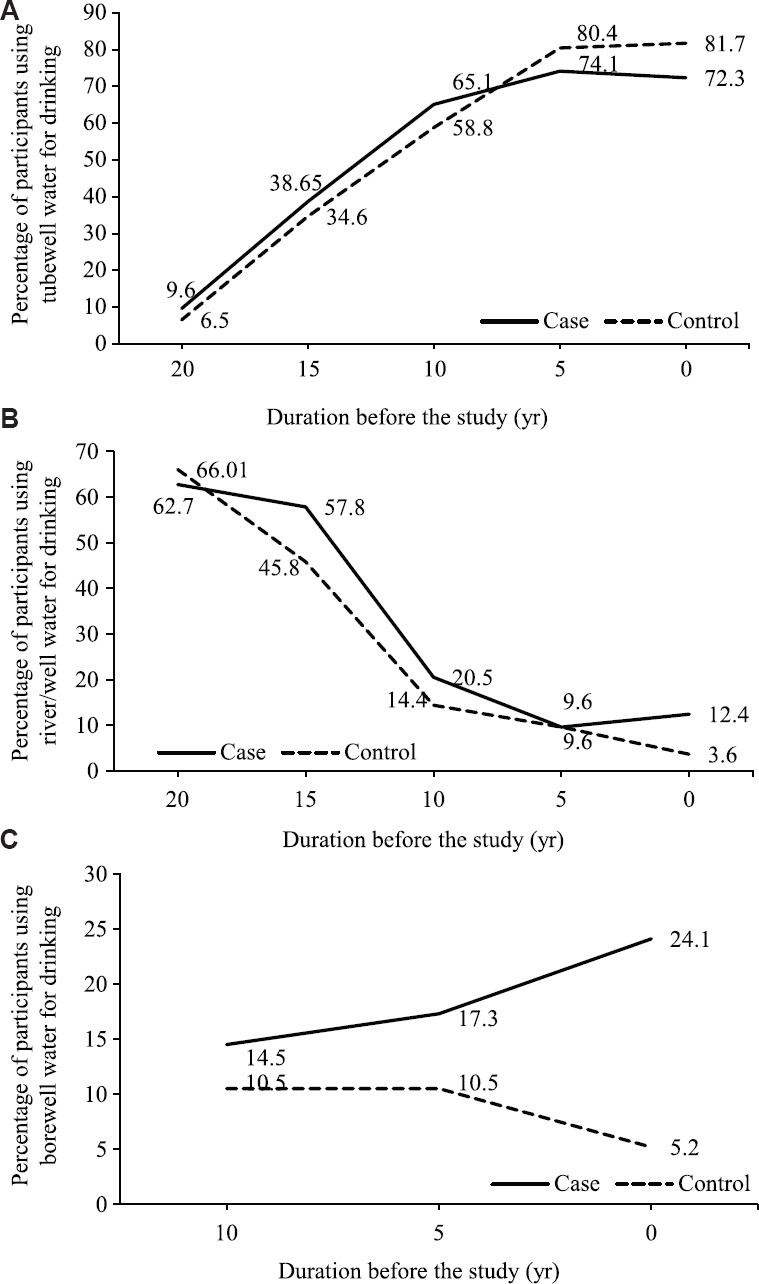
- Percentage of participants using (A) tubewell, (B) well/river, (C) borewell water as the drinking water source at different time points. Some of the participants used multiple sources of water, thus have been counted multiple times in each group.
The variables that were found to be significantly associated among cases through univariate analysis model were further considered for multivariable analysis. According to the adjusted odds ratios (aOR), the statistically significant association of risk factors with CKD were hypertension for more than five years (aOR=4.24; 95% credible interval: 1.23-10.05), scheduled tribe/caste (aOR=2.81; 1.09-5.95), use of tubewell/borewell water for drinking (aOR=1.21; 1.02-1.43), consumption of locally made alcohol (aOR=1.09; 1.02-1.17) and dietary factors such as eating red meat and vegetarian diet with aOR=1.24; 1.12-1.39 and aOR=1.09; 1.04-1.14, respectively. The detailed multivariable analysis (Bayesian conditional logistic regression) findings are presented in Table III and findings from conditional logistic regression using frequentist method are given in Supplementary Table I.
| Variables | Unadjusted OR | 95% credible interval | Adjusted OR | 95% credible interval |
|---|---|---|---|---|
| Education | ||||
| Illiterate | Reference | |||
| Primary | 0.51 | 0.23-0.93 | ||
| Secondary and above | 0.55 | 0.22-1.06 | ||
| Socioeconomic status | ||||
| Above poverty line | Reference | |||
| Below poverty line | 0.79 | 0.44-1.28 | ||
| Ethnicity | ||||
| Others | Reference | Reference | ||
| Schedule Caste/Tribe | 2.34 | 1.28-4.05 | 2.81 | 1.09-5.95 |
| Joint pain | ||||
| Never | Reference | |||
| <5 yr | ||||
| ≥5 yr | ||||
| Diabetes | ||||
| Never | Reference | |||
| <5 yr | 2.23 | 0.82-4.98 | ||
| ≥5 yr | 1.04 | 0.33-2.36 | ||
| Hypertension | ||||
| Never | Reference | Reference | ||
| <5 yr | 1.62 | 0.74-2.95 | 1.76 | 0.60-4.40 |
| ≥5 yr | 3.22 | 1.37-6.76 | 4.24 | 1.23-10.05 |
| Acid peptic disease | ||||
| Never | Reference | |||
| <5 yr | 0.83 | 0.38-1.56 | ||
| ≥5 yr | 1.84 | 0.78-3.72 | ||
| Family history of diabetes | ||||
| No | Reference | |||
| Yes | ||||
| Family history of hypertension | ||||
| No | Reference | |||
| Yes | 0.64 | 0.31-1.17 | ||
| Tobacco/alcohol consumption | ||||
| Chewing tobacco (numbers per wk) | 0.99 | 0.98-1.01 | ||
| Smoking (Since, in yr) | 0.94 | 0.86-1.02 | ||
| Local alcohol (Since, in yr) | 1.04 | 1.01-1.09 | 1.09 | 1.02-1.17 |
| Food consumption | ||||
| Leafy green vegetables | 1.01 | 0.99-1.04 | ||
| Chicken per month | 0.91 | 0.86-0.95 | ||
| Vegetables per month | 1.08 | 1.04-1.12 | 1.09 | 1.04-1.14 |
| Red meat per month | 1.27 | 1.15-1.41 | 1.24 | 1.12-1.39 |
| Exposure to sun (reference - No) | 1.66 | 0.73-3.43 | ||
| Source of drinking water | ||||
| Well/river | Reference | Ref | ||
| Tubewell/borewell | 2.52 | 1.25-4.75 | 1.21 | 1.02-1.43 |
The Bayesian Information Criteria for the model was 110.99 indicating the best fit model. Family history of CKD was dropped from the model because of the collinearity
Discussion
To our knowledge, this is one of the first studies from India analyzing the association of different risk factors for CKD using the Bayesian approach9 rather than the frequentist approach. The mean age among the cases was 49±10.62 yr. A study done among a rural population of Karnataka reported the mean age of CKD cases to be 52.73±17.08 yr7 and another study among farmers in Sri Lanka reported the mean age of patients with CKDu was 45.5 yr in males and 47.4 yr in females13. It is a common notion that increased age escalates the chances of CKD because of associated chronic conditions such as hypertension or diabetes1415. Nearly one-fourth of the cases in the present study were ≤40 yr suggesting that besides the chronic conditions, there are also other personal and environmental factors contributing to CKD. CKDu dominates the research arena in developing countries, including India16. Focal evidences from some parts of the country support the fact that most of the patients diagnosed with CKDu are exposed to the water resources contaminated with heavy metals, heat, various drugs and disease conditions151718.
A significant association between the drinking of borewell or tubewell water and CKD cases along with a gradual shift in drinking source from river/well water to borewell/tubewell water over a decade was observed. This indicates the possibility of contamination of tubewell/borewell water with heavy metals in our study areas.
The male cases were about four times in number compared to females in this study. Research shows gender differences as standard predictors for the decline in renal function, namely proteinuria among males and poor glycaemic control among females1419. High CKD cases among males in our study could be associated to their socio-behavioural and occupational practices such as more exposure to sunlight, working in the agriculture land, exposure to pesticides and habitual consumption of locally made alcohol. In our study areas, 57.1 per cent of alcohol consumers were found to consume the locally prepared alcohol, which is prepared using many herbal ingredients in its processing. No study has been done so far to understand the intrinsic properties of these ingredients. About 47 per cent of our cases were illiterate and 43.4 per cent were unemployed. Manavalan et al20 had observed among the CKD cases, 36.3 per cent as illiterate and 80.9 per cent unemployed.
We found hypertension to be independently associated with CKD, while no such association could be observed for diabetes or acid peptic disease. In India, diabetes and hypertension account for 40-60 per cent cases of CKD21. Singh et al17 reported hypertension to be associated with low estimated GFR. In contrast to our findings, other studies have reported an increased presence of APD or peptic ulcer among CKD patients22, proton-pump inhibitors to increase the risk of CKD23.
A significant association between the consumption of red meat with CKD was observed in this study. Various studies had shown that consumption of processed foods containing high sugar, salt and protein was associated with CKD2425. According to Rebholz et al26, higher plant protein intake was associated with a lower risk of incident of CKD. In contrast to it, we found a significant association between the consumption of green leafy vegetables with CKD. Association with green leafy vegetables is due to increased proportion of CKD cases consuming green leafy vegetables compared to controls. Whether this association is true or a spurious one requires further research.
Family history of CKD and people belonging to SC/ST were significantly associated with CKD. Other research studies have shown that family history of CKD was significantly associated with CKD cases15 and family history of kidney failure or dialysis is associated with an increased incidence of ESRD27. Research studies from other countries suggest that some minor ethnic groups are more susceptible for chronic diseases including CKD28, this information is limited from India. The present study suggests for genetic and molecular studies to test this hypothesis. Rajapurkar et al29 in their study had shown that patients with CKD of unknown aetiology were younger, poorer and more likely to present with advanced CKD which correlates with the present study findings.
In the present study factors such as presence of hypertension for more than five years, consumption of locally made alcohol, consumption of leafy vegetables and/or red meat and drinking water from tubewell/borewell were found to be independently associated with CKD. A comparison of the present study findings with other published reports is presented in Supplementary Table II.
| Our study findings | Other study findings | Authors (Title) |
|---|---|---|
| The mean age among the cases was 49±10.62 yr | A study among rural population of Karnataka had found the mean age of CKD cases to be 52.73±17.08 yr | Anupama YJ, Uma G. (Prevalence of CKD among adults in a rural community in South India) |
| Study among farmers in Sri Lanka had found the mean age of the male patients with CKDu was 45.5 yr while it was 47.4 yr in females | Jayasumana C, Paranagama P, Agampodi S, Wijewardane C, Gunatilake S, Siribaddana S. (Drinking well water and occupational exposure to Herbicides is associated with CKD, in Padavi-Sripura, Sri Lanka) | |
| The male cases were about four times in number compared to females in our study | Gender-wise difference in CKD showed decline in renal function viz. proteinuria among males and poor glycaemic control among females to be associated with CKD | Chang P-Y, Chien L-N, Lin Y-F, Wu M-S, Chiu W-T, Chiou H-Y. (Risk factors of gender for renal progression in patients with early CKD) |
| Iseki K. (Gender differences in CKD) | ||
| A significant association between drinking of borewell or tubewell water and CKD was observed | Most of the CKDu patients are exposed to the water resources contaminated with heavy metals | Orr SE, Bridges CC. (CKD and Exposure to Nephrotoxic Metals) |
| About 47 per cent of our cases were illiterate and 43.4 per cent were unemployed | Among the CKD cases, 36.3 per cent as illiterate and 80.9 per cent unemployed | Manavalan M, Majumdar A, Harichandra Kumar K, Priyamvada P. (Assessment of health-related quality of life and its determinants in patients with CKD) |
| Hypertension to be independently associated with CKD, while no such association was found for diabetes or acid peptic disease | In India diabetes and hypertension account for 40-60 per cent cases of CKD | Varma PP. (Prevalence of CKD in India - Where are we heading?) |
| Hypertension to be associated with low eGFR | Singh NP, Ingle GK, Saini VK, Jami A, Beniwal P, Lal M, et al. (Prevalence of low glomerular filtration rate, proteinuria and associated risk factors in North India using Cockcroft-Gault and Modification of Diet in Renal Disease equation: an observational, cross-sectional study) | |
| Increased presence of APD or peptic ulcer among CKD patients | Liang C-C, Muo C-H, Wang I-K, Chang C-T, Chou C-Y, Liu J-H, et al. (Peptic ulcer disease risk in CKD: 10 yr incidence, ulcer location and ulcerogenic effect of medications) | |
| Family history of CKD was significantly associated with CKD | Other research studies had showed family history of CKD was significantly associated with CKD cases | Kazancioğlu R. (Risk factors for CKD: An update) |
| Family history of kidney failure or dialysis is associated with increased incidence of ESRD | Drawz PE, Sedor JR, Hostetter TH. (Family History and Kidney Disease) | |
| Scheduled caste and Tribe people were significantly associated with CKD | Some minor ethnic groups are more susceptible for chronic diseases including CKD | Harawa NT, Norris KC. (The Role of Ethnic Variation and CKD) |
| Consumption of locally made alcohol was independently associated with CKD | Not available | NA |
| Consumption of leafy vegetables was independently associated with CKD | Higher plant protein intake was associated with lower risk of incident of CKD | Rebholz CM, Coresh J, Grams ME, Steffen LM, Anderson CAM, Appel LJ, et al. (Dietary Acid Load and Incident CKD: Results from the ARIC Study) |
| Consumption of red meat is independently associated with CKD | Consumption of processed foods containing high sugar, salt and protein were associated with CKD | Odermatt A. (The Western-style diet: a major risk factor for impaired kidney function and CKD) |
| Kramer H. (Dietary patterns, calories and kidney disease) |
CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease; APD, acid peptic disorder; NA, not available; CKDu, chronic kidney disease of unknown aetiology; ARIC, atherosclerosis risk in communities
Despite these shortcomings the present study was intended to explore various factors associated with CKD. Some of the limitations of this study include its inability to establish the cause and effect relationship. It limits in understanding the detailed intrinsic properties of the factors such as the locally made alcohol, the tubewell/borewell water, duration and usage of various medicines, etc. The cases were not studied according to their stages of CKD and their clinical details such as the oliguric status, differentiation of cases as glomerular or interstitial nephritis. More hospital and laboratory based studies could address these gaps.
DAG (Fig. 3) was constructed by the authors using R software30 and this explains the relationship of various associated factors with CKD. After adjusting for hypertension and alcohol, drinking water was found to be associated with CKD and also connected to the ethnicity. However, hypertension could be a mediating factor between drinking water and CKD. The direct association of hypertension with CKD could have been because of the presence heavy metals in the drinking water. Based on the findings, the present study suggests to relook into the established risk factors for CKD and carry out more research to establish the causal relationship of such environmental and personal factors for CKD.
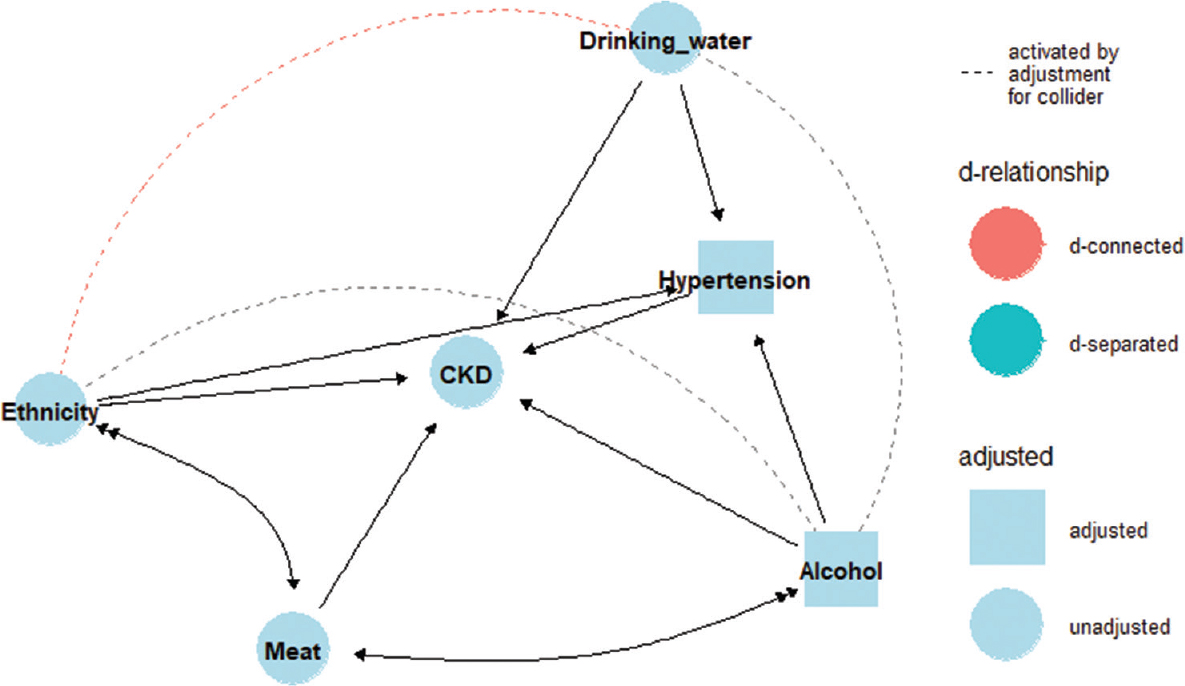
- Direct Acyclic Graph (DAG) explaining the relationship of various factors associated with chronic kidney disease (CKD).
Acknowledgment:
The authors acknowledge doctors of SCB medical college, Cuttack and Dr B. Dwivedi, RMRC, Bhubaneswar, for their valuable suggestions in data collection tool development, all participating government and private hospitals that provided patient information for this study and the State and District health officials, & the staff of District Magistrate office for their cooperation during data collection.
Financial support & sponsorship: This study was funded by TATA Steel, India.
Conflicts of Interest: None.
References
- Chronic kidney disease and the global NCDs agenda. BMJ Glob Health. 2017;2:e000380.
- [Google Scholar]
- Chronic kidney disease in low-income to middle-income countries:The case for increased screening. BMJ Glob Health. 2017;2:e000256.
- [Google Scholar]
- Global, regional, and national burden of chronic kidney disease, 1990–2017:A systematic analysis for the global burden of disease study 2017. The Lancet. 2020;395:709-33.
- [Google Scholar]
- The effects of environmental chemicals on renal function. Nat Rev Nephrol. 2015;11:610-25.
- [Google Scholar]
- Prevalence of Chronic Kidney Disease in Cuttack District of Odisha, India. Int J Environ Res Public Health. 2020;17:456.
- [Google Scholar]
- Prevalence of chronic kidney disease among adults in a rural community in South India:Results from the kidney disease screening (KIDS) project. Indian J Nephrol. 2014;24:214-21.
- [Google Scholar]
- Chapter 1:Definition and classification of CKD. Kidney Int Suppl (2011). 2013;3:19-62.
- [Google Scholar]
- A gentle introduction to bayesian analysis:applications to developmental research. Child Dev. 2014;85:842-60.
- [Google Scholar]
- On Using Bayesian Methods to Address Small Sample Problems. Struct Equ Model Multidiscip J. 2016;23:750-73.
- [Google Scholar]
- Epidemiology and risk factors of chronic kidney disease in India –results from the SEEK (Screening and Early Evaluation of Kidney Disease) study. BMC Nephrol. 2013;14:114.
- [Google Scholar]
- Relationship between educational and occupational levels, and Chronic Kidney Disease in a multi-ethnic sample- The HELIUS study. PLoS One. 2017;12:ne0186460.
- [Google Scholar]
- Drinking well water and occupational exposure to Herbicides is associated with chronic kidney disease, in Padavi-Sripura, Sri Lanka. Environ Health. 2015;14:6.
- [Google Scholar]
- Risk factors of gender for renal progression in patients with early chronic kidney disease. Medicine (Baltimore). 2016;95:e4203.
- [Google Scholar]
- Risk factors for chronic kidney disease:an update. Kidney Int Suppl (2011). 2013;3:368-71.
- [Google Scholar]
- Chronic kidney disease hotspots in developing countries in South Asia. Clin Kidney J. 2016;9:135-41.
- [Google Scholar]
- Prevalence of low glomerular filtration rate, proteinuria and associated risk factors in North India using Cockcroft-Gault and modification of diet in renal disease equation:an observational, cross-sectional study. BMC Nephrol. 2009;10:4.
- [Google Scholar]
- Chronic kidney disease and exposure to nephrotoxic metals. Int J Mol Sci. 2017;18:1039.
- [Google Scholar]
- Assessment of health-related quality of life and its determinants in patients with chronic kidney disease. Indian J Nephrol. 2017;27:37-43.
- [Google Scholar]
- Prevalence of chronic kidney disease in India - Where are we heading? Indian J Nephrol. 2015;25:133-5.
- [Google Scholar]
- Peptic ulcer disease risk in chronic kidney disease:ten-year incidence, ulcer location, and ulcerogenic effect of medications. PLoS One. 2014;9:e87952.
- [Google Scholar]
- Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease. JAMA Intern Med. 2016;176:238-46.
- [Google Scholar]
- The Western-style diet:a major risk factor for impaired kidney function and chronic kidney disease. Am J Physiol Renal Physiol. 2011;301:F919-31.
- [Google Scholar]
- Dietary patterns, calories, and kidney disease. Adv Chronic Kidney Dis. 2013;20:135-40.
- [Google Scholar]
- Dietary Acid Load and Incident Chronic Kidney Disease:Results from the ARIC Study. Am J Nephrol. 2015;42:427-35.
- [Google Scholar]
- What do we know about chronic kidney disease in India:First report of the Indian CKD registry. BMC Nephrol. 2012;13:10.
- [Google Scholar]




