Translate this page into:
Effect of active immunization against angiotensin II type 1 (AT1) receptor on hypertension & arterial remodelling in spontaneously hypertensive rats (SHR)
Liu-Dong Li and Miao Tian are co-first authors.
Reprint requests: Dr Yu-Hua Liao, Laboratory of Cardiovascular Immunology, Institute of Cardiology, Union Hospital Tongji Medical College, Huazhong University of Science & Technology, Wuhan, PR China e-mail: doctorzht@163.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Angiotensin II receptor type 1 (AT1) is known to be involved in the pathogenesis of hypertension. this study was undertaken to explore the effect of active immunization against AT1 receptor on blood pressure and small artery remodelling in spontaneously hypertensive rat (SHR).
Methods:
Male SHR and Wistar rats aged two months were actively immunized with different peptides (ATR12185, ATR10014 and ATR12181) corresponding to particular sequences of rat AT1 receptor, while another SHR group was given losartan (10 mg/kg/day) orally once a day. Anti-AT1 receptor antibodies were detected by ELISA and blood pressure was measured. The effect of the antibodies on the artery and vascular smooth muscle cells (VSMCs) proliferation was studied.
Results:
All immunized animals produced antibodies against the particular peptides. The systolic blood pressure was decreased in the SHR immunized with peptide-ATR12181 compared with the control. However, no changes were observed in the SHR immunized with other two peptides. The Wistar rats immunized with the three peptides did not show any changes in blood pressure. The media/lumen area ratio of the mesenteric artery was reduced in SHR immunized with ATR12181 and similar to that of the SHR treated with losartan. The antibody from SHR immunized with ATR12181 had no effect on the proliferation of VSMC. But it could inhibit the proliferation caused by angiotensin II and its effect at the titre of 1:40 was similar to that of 1µmol/l losartan.
Interpretation & conclusions:
Our findings demonstrated that the antibody from SHR immunized with ATR12181 had the effect of reducing blood pressure and target organ protection similar to losartan. Active immunization against AT1 receptor may be a promising strategy in future for the treatment of hypertension.
Keywords
Antibody
AT1 receptor
proliferation
SHR
vascular smooth muscle cell

Hypertension is a major risk factor in many cardiovascular pathophysiological states, including arteriosclerosis, stroke, heart failure, coronary artery disease and progressive renal damage123. The involvement of the renin-angiotensin system (RAS) in the occurrence and development of hypertension has been addressed. Interruption of the RAS pathway, either by preventing the formation of angiotensin II (i.e., angiotensin converting enzyme inhibitor) or by blocking its actions at the level of the peptide receptor [i.e., angiotensin II type 1 (AT1) receptor antagonists], has been proved to be highly successful in the treatment and management of hypertension4.
Angiotensin II is the principle effector molecular of the RAS. It can regulate blood pressure, modulate arterial wall growth, increase DNA synthesis and protein synthesis in vascular smooth muscle cells (VSMCs). The major actions of angiotensin II have been reported to be mediated by the AT1receptor5678. The AT1 receptor belongs to the superfamily of seven transmembrane receptors. The three extracellular loops and the N-terminal part of it are involved in angiotensin II binding as well as binding of other antibodies9. the blockade of AT1 receptor by active immunization against the sequence 14-23 of AT1 receptor peptide has been shown to attenuate hypertension10. Fu et al11 immunized rats with the synthetic peptide corresponding to the second loop of human AT1 receptor (residues 165-191) as antigen for 3 months, and then produced antibodies from the immunized serum. these antibodies also had an agonist-like activity11. Another study findings indicated that the active immunization against angiotensin I might be a useful approach for treating cardiovascular disorders involving the renin-angiotensin system12.
We, therefore, established active immunization with the peptides corresponding to the different sequences of AT1 receptor, coded as ATR12181, ATR12185 and ATR10014. The influence of antibodies induced by the above peptides on the blood pressure and vascular remodelling in SHR was studied.
Material & Methods
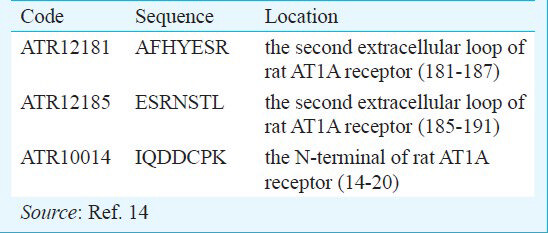
Preparation of peptides: Peptides corresponding to different sequences of extracellular parts of the AT1 receptor named as ATR12185, ATR10014 and ATR12181 were prepared by solid phase method13. These were synthesized with PSSM-8 peptide synthesizer (Shimadzu, Tokyo, Japan). The peptides were purified by HPLC analysis using a Sepharon SG×C18 column. The purity of all peptides prepared was higher than 95 per cent. The appropriate amount of each peptide (10 mg) was weighed out, dissolved in phosphate buffered saline (PBS, pH-9.0) and mixed with tetanus toxoid (TTX, The institute of biological products of Wuhan, China) (100 ml). Following this, 0.3 per cent glutaraldehyde solution (3 ml) was added and incubated for two hours at room temperature. glycerine (1 mol/l, 0.25 ml) was added into the solution and incubated for 30 min at room temperature for blocking. The mixture was dialyzed against PBS (pH 8.5) at 4°C overnight, and 100 µl of the conjugate containing 0.1 mg of peptide was used as a dose for the immunization of animal. Table I shows the sequences and locations of the peptides.
Immunization: The experiments were conducted in the laboratory of Cardiovascular Immunology, Institute of Cardiology, Tongii Medical College, Huazhong University of Science and Technology, Wuhan, PR China. The study protocol was approved by the Ethics Committee of Tongji Medical College of Huazhong University of Science and Technology. Male SHR and Wistar rats (The Experiment Animal Centre of Chinese Academy of Medical Science) aged two months were immunized repeatedly by subcutaneous injection respectively with the synthesized peptides including ATR12185, ATR10014 and ATR12181 at 0, 2th, 4th, 8th, 12th, 16th and 20th week (n=7 per group). The peptide-TT conjugate was coupled with the same volume of Freund's adjuvant (Wuhan Yafa Biological Technology Ltd., PR China). Complete Freund's adjuvant was used in the initial injection and incomplete for subsequent procedures. The homo-age male SHRs received complete or incomplete Freund's adjuvant only in the same schedule as control and another group was given losartan (10 mg/kg/day) orally by gastric gavage once a day every morning. The immunized Wistar rats were used as negative controls.
Blood pressure measurement and anti-AT1 receptor antibody detection of ELISA: Systolic blood pressure (SBP) was measured with a standard tail-cuff technique using Powerlab system (AD Instruments, Australia) before immunization and every month after immunization. Blood samples were collected every 4 wk to detect the anti-AT1 receptor antibodies by ELISA as described previously15. Briefly, peptides (10 µg/ml) in a 100 mM Na2CO3 solution (pH 9.6) were used to coat individual wells of a 96-well microtitre plates and left overnight. Blocking was performed with phosphate buffered saline (PBS pH7.4, supplemented with Tween-20). Then serially diluted serum samples were applied at 37°C for 1 h. The second antibody, goat anti-rat IgG antibodies conjugated with horseradish peroxidase (Huarui Biotech Co. Ltd., Zhuhai, PR China) diluted 1:2000, was added and incubated for 30 min at 37°C. Bound peroxidase activity was detected using H2O2 and 3’-3’-5’-5’-tetramethyl benzidine as substrate. Optical density (OD) was measured at 450 nm in a microplate reader (Bio-tek type EX 2800, USA). The negative control was the serum taken from the same rat prior to immunization. Cases with P/N > 2.1 were considered positive.

Histological analysis: The rats were sacrificed at the end of the experiment. The third-order branch of mesenteric artery was excised, embedded in paraffin, cut into 5-μm cross sections and stained with collagen-specific van Gieson or hematoxylin-eosin. The media thickness and lumen diameter of arteries were measured with a microscope (Olympus, Japan) and HPIAS scanning and image analysis system and the media/lumen area ratio was calculated. The media area was expressed as CSA (cross sectional area) CSA = (CSAtot-CSA1um) × (IDshort/IDlong) (ID: internal diameter). The lumen area was calculated according to the measured internal diameter of the lumen.
Preparation of the immunoglobulin: The immunoglobulin fractions were prepared from the serum of SHRs immunized with ATR12181 by precipitation in 50 per cent (NH4)2SO4 and dialyzed extensively against PBS (pH7.4). The immunoglobulin fractions prepared were purified by immune affinity chromatography16. In brief, immunoglobulin fractions (IgG) were loaded on a Sepharose 4B CNBr-activated gel (Pharmacia, USA) to which the peptides corresponding to the sequences of the AT1 receptor were covalently linked. The antibodies were eluted with 3 mol/l potassium thiocyanate (pH 7.4) followed by immediate super-filtration by millipore Centriplus 50000 (Millipore, USA), changed and concentrated the buffer with PBS. Immunoglobulin fractions from normal Wistar rats were used as negative control.
Cell culture and proliferation assays: Aortic vascular smooth muscle cells (VSMCs) were obtained by the method of Karas et al17. Cells were characterized by immunohistochemical assay with anti-α-actin mAbs (Sigma Chemical Co., USA). Ninety per cent of the cells expressed α-actin. Cells between passages 5 and 8 were used in these experiments.
The proliferation of VSMCs was determined by DNA synthesis and cell cycle analysis. VSMCs were plated into 96-well plates at a density of 5×103 cells/well in complete DMEM growth medium until they reached 70 per cent confluence. The proliferation of VSMCs was analyzed using a Cell Proliferation ELISA Kit (Exalpha Biologicals Inc, USA) according to the manufacturer's instruction. In brief, the cells were exposed to 10 mol/l 5-bromo-2′-deoxyuridine (BrdU) solution for 2 h, followed by cell fixation, DNA denaturation and blocking. After incubation with peroxidase-labelled anti-BrdU, the wells were rinsed and 3,3′,5,5′-tetramethylbenzidine (TMB) in 15 per cent dimethylsulphoxide (DMSO) was added. The samples were mixed for 10 min, after which 1 M sulphuric acid was added to stop the reaction, and the absorbance was measured at 450 nm using a microplate reader (Model 550, Bio-Rad Laboratories, USA). The cell proliferation activity values are expressed as the means of at least three independent experiments each performed in five replicates.
Statistical analysis: Values are expressed as mean ± SE. The statistical significance of differences among groups was determined by one-way analysis of variance with Holm's post hoc test. P< 0.05 was considered significant.
Results
Antibodies against the peptides of AT1 receptor: The antibodies appeared in one month in all SHRs after actively immunized by the three peptides. The titre reached the highest level at the 4th month and then fell slowly after the 5th month. In normal control SHRs, the antibodies were not detected. The titres of the antibody against ATR12181 and ATR10014 reached at higher levels than that of ATR12185 (Fig. 1). Similar results were found in the immunized Wistar rats (Data not shown).
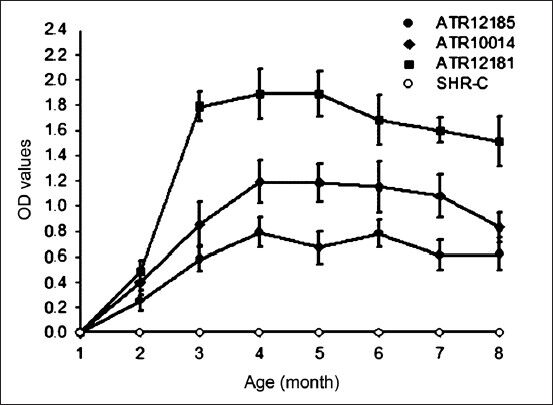
- Titres of antibodies against peptide-ATR12181, ATR10014 and ATR 12185 in SHRs after immunization. SHR-C represents SHR control. SHR-ATR12181, ATR10014 and ATR12185 represent immunized group with ATR12181, ATR10014 and ATR12185, respectively. Values are mean ± SD (n=7).
Blood pressure after active immunization: The SHR developed high blood pressure after two months of immunization. After three months of immunization the SBP of the SHR immunized with ATR12181 were markedly lower than that of the control group. ATR12181 immunization decreased the SBP to a similar extent to losartan. However, no changes of SBP were observed in SHR immunized with ATR12185 or ATR10014. The changes of SBP were not found in the Wistar rats immunized with the above three peptides in comparison with non-immunized Wistar controls (Data not shown). Statistics for the data are shown in Table II.

Morphological changes of mesenteric artery in immunized rats: Compared to the Wistar rats, the media of the mesenteric artery was thicker and the lumen was smaller in the SHR. In the SHR immunized with ATR12181, the media became thinner and the lumen larger. The media/lumen area ratio of the mesenteric artery was smaller in the immunized SHR than that of the control group and similar to that of the losartan group (Fig. 2). Statistics for the data are shown in Table III.

- Morphological changes of mesenteric artery in Wistar rats and SHRs immunized with different peptides. Photomicrographs of sections of mesenteric artery from Wistar rats, SHR of control and three peptide group. (Stained with hematoxylin-eosin, X 100). In the SHR immunized with ATR12181, the media became thinner and the lumen larger and the media/lumen area ratio of the mesenteric artery was smaller than that of control and similar to that of Losartan group.

Proliferation of VSMC induced by antibodies against ATR12181: It had been identified that angiotensin II can stimulate the proliferation of VSMC, which can be attenuated by losartan. The antibody purified from the SHR immunized with ATR12181 had no effect in proliferation of VSMC, but it could inhibit the increased effect of proliferation caused by Ang II (Fig. 3). The antibody (1:40) had a similar effect to 1µmol/l losartan.

- Effects of active immunization on proliferation of vascular smooth muscle cells (VSMC). Values are mean ± SE (n=7). *P<0.05 vs. Ang II.
Discussion
It was demonstrated in our experiment that repeated immunization of SHR against rat angiotensin II receptor type I (AT1) attenuated the development of hypertension. The similar reduction of systolic blood pressure was observed in the losartan treatment group. At the same time, there was reduction in the media thickness and media/lumen area ratio of mesenteric arterioles in the ATR12181 immunization as that of losartan treatment group. Finally, these antibodies displayed antagonist-like activity shown as inhibition of VSMCs proliferation.
The peptide ATR12181 contains the 181-187 amino acid sequence of the second extracellular AT1 receptor loops. Wallukat et al18 first described the same sequence of human AT1 receptor. They found that immune mechanism and the renin-angiotensin system were implicated in pre-eclampsia. Immunoglobulin from pre-eclampsia patients stimulated the AT1 receptor. When the immunoglobulin was pre-exposed to peptides containing the amino acid sequence of the first, second and third extracellular AT1 receptor loops, only peptides from the second extracellular loop abolished the stimulatory effect. They used the affinity column-purified material to examine possible epitopes on the second extracellular loop of the AT1 receptor. Their findings suggest that only the amino acid sequence AFHYESQ contains the binding epitopes of the antibody. In our study, three peptides were used corresponding to different sequences of the second extracellular loop and the N-terminal of rat AT1 receptor (Table I). All the immunized rats produced antibodies against the particular peptides. But only the antibodies against the peptide ATR12181 attenuated the development of hypertension of SHRs. Further, Wistar rats immunized with peptide ATR12181 did not develop hypertension or morphological changes of mesenteric artery, indicating that the antibody against ATR12181 did not show agonist activity.
The AT1 receptor is composed of 359 amino acids, with approximately 40-41kDa molecular weight. It belongs to the superfamily of G-protein-coupled receptors. It contains seven hydrophobic transmembrane segments forming αhelics in the lipid bilayer of the cell membrane. The extracellular regions are composed of the N-terminal part and three extracellular loops. Each of the extracellular parts can be an antigen and produce an antibody11, and every antibody against different peptides of AT1 receptor may have different biological effects19. Zelezna B et al10 demonstrated that repeated immunization of young SHRs against sequence 14-23 of angiotensin AT1 receptor attenuated the development of hypertension. But no difference in heart and kidney hypertrophy was observed compared to sham-immunized SHR. It has been identified that angiotensin II can stimulate migration, proliferation and hypertrophy of VSMCs, leading to cadiac hypertrophy, remodelling, restenosis and atherosclerosis2021. In our study, in the SHR immunized with ATR12181, the media of the mesenteric artery became thinner and the lumen larger. The media/lumen area ratio was smaller than that of controls. The antibody purified from the SHR immunized with ATR12181 had no effect in proliferation of VSMC, but it could inhibit the increased effect of proliferation caused by Ang II. From these results one can infer that the antibody against AT1 receptor from SHR immunized with ATR12181 may bind to the corresponding site of extracellular part of the receptor and block or weaken the function of angiotensin II. This effect may be independent of the SBP lowering.
In conclusion, our results confirmed the role of AT1 receptor in the development of hypertension and the secondary organ lesion. Active immunization with ATR12181 against angiotensin AT1 receptor lowered the blood pressure and ameliorated the remodelling of small arteries of SHR. This might offer an exciting head in the treatment of diseases involving RAS system such as hypertension and chronic heart failure.
References
- Coronary endothelial dysfunction in the hypertensive patient: from myocardial ischemia to heart failure. J Hum Hypertens. 1997;11:45-9.
- [Google Scholar]
- The renin-angiotensin system and its receptors. J Cardiovasc Pharmacol. 1999;33(Suppl 1):S21.
- [Google Scholar]
- Diabetes, hypertension and atherosclerosis: pathophysiological role of intracellular ions. Int Angiol. 1993;12:365-70.
- [Google Scholar]
- Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359:995-1003.
- [Google Scholar]
- Renin-angiotensin-aldosterone system blockade for cardiovascular diseases: current status. Br J Pharmacol. 2010;160:1273-92.
- [Google Scholar]
- RAAS inhibitors and cardiovascular protection in large scale trials. Cardiovasc Drug Ther. 2013;27:171-9.
- [Google Scholar]
- Identification of peptide binding residues in the extracellular domains of the AT1 receptor. J Biol Chem. 1994;269:30953-9.
- [Google Scholar]
- Influence of active immunization against angiotensin AT1 or AT2 receptor on hypertension development in young and adult SHR. Physiol Res. 1999;48:259-65.
- [Google Scholar]
- Immunohistochemical localization of angiotensin II receptors (AT1) in the heart with anti-peptide antibodies showing a positive chronotropic effect. Receptors Channels. 1998;6:99-111.
- [Google Scholar]
- Active immunization with angiotensin I peptide analogue vaccines selectively reduces the pressor effects of exogenous angiotensin I in conscious rats. Br J Pharmacol. 2000;129:1178-82.
- [Google Scholar]
- Solid phase peptide synthesis. I. The synthesis of a tetrapeptide. J Am Chem Soc. 1963;85:2149-54.
- [Google Scholar]
- Target organ protection from a novel angiotensin II receptor (AT1) vaccine ATR12181 in spontaneously hypertensive rats. Cell Mol Immunol. 2006;3:107-14.
- [Google Scholar]
- Autoantibodies against AT1-receptor and alpha1-adrenergic receptor in patients with hypertension. Hypertens Res. 2002;25:641-6.
- [Google Scholar]
- Inhibition of central angiotensin responses by angiotensin type-1 receptor antibody. Hypertension. 1993;21:1062-5.
- [Google Scholar]
- Human vascular smooth muscle cells contain functional estrogen receptor. Circulation. 1994;89:1943-50.
- [Google Scholar]
- Patients with preeclampsia develop agonistic autoantibodies against the angiotensin AT1 receptor. J Clin Invest. 1999;103:945-52.
- [Google Scholar]
- Angiotensin II induces hypertrophy, not hyperplasia, of cultured rat aortic smooth muscle cells. Circ Res. 1988;62:749-56.
- [Google Scholar]
- Angiotensin II induces smooth muscle cell proliferation in the normal and injured rat arterial wall. Circ Res. 1991;68:450-6.
- [Google Scholar]
- Pathophysiological role of tissue renin-angiotensin-aldosterone system (RAAS) in human atherosclerosis. Nihon Rinsho. 2012;70:1556-61.
- [Google Scholar]




