
Translate this page into:
Does endoscopic thoracic sympathectomy through clipping procedure have early effects on electrocardiographic parameters?
Reprint requests: Dr. Fatih Candas, Department of Thoracic Surgery, GATA Haydarpasa Training Hospital, 34668 Istanbul, Turkey e-mail: fhcandas@yahoo.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Hyperhidrosis is a pathologic condition of excessive sweating in amounts greater than physiologic needs. Endoscopic thoracic sympathectomy (ETS) is a globally accepted treatment modality for primary palmar and axillary hyperhidrosis. ETS also has distinctive effects on the heart, circulatory and respiratory systems. In this study early effects of ETS on electrocardiographic (ECG) parameters of hyperhidrosis patients were evaluated.
Methods:
Twelve-lead ECGs were performed on 72 patients who were free from cardiovascular, metabolic, neurological and pulmonary diseases and underwent planned ETS because of hyperhidrosis, before and after the procedure within the first 24 h. Heart rate (HR), PR, QT, corrected QT (QTc), QTc/Tpeak-Tend (TpTe) intervals, P-wave and QTc/TpTe dispersions were compared by ECG.
Results:
A total of 72 patients (24.1±6.0 yr, 17 female) were included in the study. The pre-operative HR of patients was significantly higher than post-operative HR of patients (73.8±12.8 vs. 68.1±12.6 beats/ min; P<0.001). The QTc dispersion (QTcd) durations of pre-operative patients were significantly longer than those of post-operative patients (51.5±6.3 vs. 44.9±5.6 msec; P<0.01). The TpTe dispersion value of pre-operative patients was significantly (P<0.001) higher than that of post-operative patients.
Interpretation & conclusions:
Our study showed that ETS through clipping procedure had positive effects on the mechanisms of arrhythmia by reducing HR, QTcd, TpTe and TpTe dispersion parameters of ECG in early periods in hyperhidrosis patients.
Keywords
Clips
corrected QT dispersion durations
electrocardiography
ETS
heart rate
hyperhidrosis
sympathectomy
Tpeak-Tend dispersion

Hyperhidrosis is defined as a pathologic condition of excessive sweating in amounts greater than physiologic needs. It can be primary or secondary. Endoscopic thoracic sympathectomy (ETS) is a globally accepted treatment modality for primary palmar and axillary hyperhidrosis1234. Cardiac electrophysiology is regulated by the autonomic nervous system which is based on two mechanisms called sympathetic and parasympathetic. Activated sympathetic nervous system creates a tendency to arrhythmogenesis, which is counterbalanced by the activated parasympathetic nervous system. T2-T3 ETS, which is used to treat primary hyperhidrosis, reduces sympathetic discharge through bilaterally blockage of sympathetic nervous system, thus causes decreased sweating of hands and armpits13. ETS also has distinctive effects on the heart, circulatory and respiratory systems. The reason for this is that the sympathetic innervation of the heart originates from efferent neurons of spinal ganglions on T1-T4 levels5. Reduced heart rate (HR) at rest and exercise after ETS has been reported in earlier studies56. Repolarizations of myocardial cells on the heart are not synchronized. Ventricular repolarization can be evaluated by QT interval, corrected QT (QTc) interval and QT dispersion (QTd) measurements on standardized superficial 12-lead electrocardiography (ECG). QT and QTc intervals show the period of ventricular repolarization, and QTd shows the heterogeneity of distribution of ventricular repolarization. An increase in heterogeneity raises the tendency for arrhythmia. It has been shown that QTd and ventricular arrhythmia are related67.
Tpeak-Tend (TpTe) interval is the interval between the T wave's ending and peak point. This new interval shows transmural dispersion of ventricular repolarization. TpTe/QT and TpTe/QTc ratios have been examined as a new electrocardiographic index at the risk of ventricular arrhythmia and considered as a practical index8910.
This study was undertaken to evaluate pre- and post-operative ECG findings in hyperhidrosis patients who had T3 ETS performed. The purpose was to determine the effect of minimally destructive sympathetic denervation on resting ECG parameters (HR, QT, QTd, TpTe, TpTe/QT and TpTe/QTc) in patients with palmar hyperhidrosis.
Material & Methods
The study population consisted of 72 consecutive patients with hyperhidrosis (55 men, 17 women; mean age, 24.1±6.0 yr) who were free from any cardiovascular, pulmonary, metabolic or neurological diseases. All patients underwent ETS with clips for palmar and axillary hyperhidrosis between May 2012 and November 2013 at the department of Thoracic Surgery, GATA Haydarpasa Training Hospital, Turkey. Fifty one patients had palmar and 21 had palmar and axillary hyperhidrosis. Informed consent forms were provided to and signed by all participants. The study was approved by the human ethics committee of the hospital, and informed written consent was obtained from all patients.
Thoracoscopic sympathectomy: Bilateral ETS was performed in a single operating session under general anaesthesia with selective bronchial intubation using a double-lumen endotracheal tube. The patient was placed in a semi-sitting position at 90° with both arms in abduction. Two incisions of 5 and 10 mm, respectively, on the anterior and medial axillary lines were made, through which the video endoscope and the endoclips were introduced. After a unilateral lung collapse, the paravertebral sympathetic chain was identified, and the costal arches were localized. ETS was performed at the level of the third costal arch (T3) by 8 mm endoclips (Auto Suture, Norwalk, USA). After manual expansion of the lung, a pleural drain was placed and connected to an aspiration system until air was completely expelled from the pleural cavity. The drain was then withdrawn, and both incisions were closed. A post-operative chest X-ray was routinely performed. The patients were discharged from hospital the day after operation.
Electrocardiography: A standardized 12-lead ECG was performed one day before and after ETS procedure and after 10 min of rest. For analysis of the ECG parameters, lead II was recorded at sampling frequency of 512 Hz; 10 sec length segment ECG during selected episodes of arousal was used. P-wave duration, RR interval, PR interval, QRS duration, QT interval and TpTe interval were measured manually. QTc interval was calculated using Bazett's formula11. TpTe/QT ratio and TpTe/QTc ratio were calculated.
Statistical analysis: Paired samples t test was used to compare continuous variables, and Chi-square test was used for categorical variables. Statistical analyses were performed using SPSS 11.0 (SPSS Inc., Chicago, IL, USA).
Results
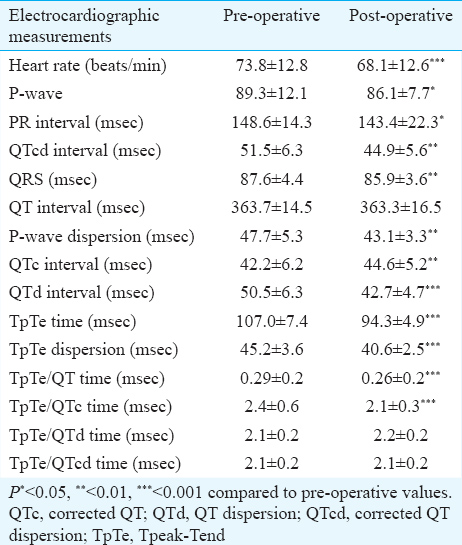
A total of 72 patients (24.1±6.0 yr, 17 female) were included in the study. The pre-operative HR of patients was significantly higher than post-operative HR (73.8±12.8 vs. 68.1±12.6 beats/ min; P<0.001).
Four patients had sinus tachycardia on the ECG records taken at our department in pre-operative patients. The P-wave dispersion of pre-operative patients was found to be higher than that of post-operative patients (pre-operative: 47.7±5.3, post-operative: 43.1±3.3 msec; P<0.01). The QTc dispersion (QTcd) durations of pre-operative patients were significantly longer than of post-operative patients (pre-operative: 51.5±6.3, post-operative: 44.9±5.6 msec; P<0.01). The QTcd value was detected to be above 60 msec in 12 pre-operative patients (16%) and none of the cases in post-operative patients (P<0.001). The TpTe interval of pre-operative patients was significantly longer than that of post-operative patients (P<0.001). The TpTe dispersion value of pre-operative patients was significantly (P<0.001) higher than of post-operative patients (Table). TpTe/QT and TpTe/QTc ratios of pre-operative patients were significantly (P<0.001) higher than that of post-operative patients. TpTe/QTcd ratio was not significantly different in pre-operative and post-operative patients (Table).
Discussion
Sympathectomy is applied traditionally as cardiac sympathetic denervation of the left side, cardiac sympathetic denervation of the right side and bilateral cardiac sympathetic denervation. Bilateral cardiac sympathetic denervation is more advantageous than one-sided denervation in decreasing the tendency of arrhythmia of the ventricle. It has been observed that bilateral denervation decreases the tendency of tachycardia and ventricular fibrillation by shortening QT length on long-QT syndromes that are non-responsive to β-blockers and anti-arrhythmics1213.
Yazbek et al14 have established that level T3 ETS is superior to level T2 ETS by causing less post-operative compensatory hyperhidrosis. We also preferred level T3 bilateral ETS due to the less compensatory hyperhidrosis and similar efficiency. In our study, a distinctive decrease of post-operative rest-HR was observed compared to pre-operative HR. This effect was more explicit at rest and maximal exercise and as vigorous as the β-blocker treatment. Kim et al15 detected a distinctive decrease at rest-HR after ETS in their study, similar to our study. Noppen et al16 detected a decrease at both rest and exercise HR, but Vigil et al17 detected a distinctive decrease at rest-HR, although only a minimal decrease at maximum-HR at exercise. Increasing the sympathetic effect and decreasing the parasympathetic effect during exercise can explain this situation. It has been reported, in rare cases, that permanent cardiac pacemaker implantation is necessary for permanent and symptomatic bradycardia after bilateral ETS1819. Kim et al15 also reported cardiac arrest after bilateral ETS. In our study, bradycardia and arrest did not occur.
QTd is dependent on the regional heterogeneity of ventricular repolarization and it is known to be an indicator of electrical instability of myocardium. QTd is used to indicate the tendency of arrhythmia in disorders such as acute coronary syndromes, hypertension, long-QT syndromes and autonomical disorders2021. Patients with hyperhidrosis in our study were young, had normal range of QT, QTd, TpTe, TpTe/QT and TpTe/QTc in their pre-operative 12-lead ECGs and had no cardiovascular, pulmonary, neurological or metabolic diseases that could have affected these parameters.
Increased sympathetic activity in hyperhidrosis patients may cause increased tendency to arrhythmia of the heart. ETS procedure may decrease the tendency to arrhythmia by modulating the neuronal axle of the heart. In our study, post-operative QTd and QTcd periods were significantly decreased compared to the respective pre-operative values. The QTcd value was detected to be above 60 msec in 16 per cent pre-operative patients and in none of the cases in post-operative patients. This situation shows that bilateral level T3 ETS procedure affects the sympathetic neuron chain that effectively innervates the heart. Further, QTcd value being not over 60 msec in any post-operative patient showed the decrease of heterogeneity of ventricular repolarization. Kim et al15 showed a distinctive decrease at rest-HR after levels T2, T3, T4 ETSs but distinctively increased post-operative QTc value in contrary to our study. Analyses according to levels in this study showed the changes at level T2 ETS on HR and QTC, level T3 ETS on HR and PR interval and level T4 ETS on QTc interval. These results indicate that the ETS procedure may be more effective on level T3 in the hyperhidrosis patients.
TpTe interval is an index that reflects the transmural dispersion of ventricular repolarization22. TpTe interval is a period that is potentially sensitive to re-entrant ventricular arrhythmias, and extending this interval increases the tendency to arrhythmia. Prolonged TpTe interval, studied in long-QT syndromes, hypertrophic cardiomyopathy with troponin-I mutation and acute myocardial infarction, was found to be related to increased mortality rates23. Similar to TpTe interval, TpTe dispersion, TpTe/QT ratio and TpTe/QTc ratio are used in detecting a tendency for ventricular arrhythmia222324. In our study, the TpTe interval of pre-operative patients was significantly longer than that of post-operative patients. The TpTe dispersion value, TpTe/QT and TpTe/QTc ratios of pre-operative patients were significantly higher than of post-operative patients. In our study, bilateral level T3 ETS procedure, when used in the treatment of hyperhidrosis, caused a distinctive modification on sympathetic nervous system. These parameters, which can be easily acquired by a 12-lead ECG applied to hyperhidrosis patients pre- and post-operatively, can reveal useful information on the early effectiveness of the procedure and detection of rare complications yet to emerge. The main limitation of our study was the lack of long-term information of ETS procedure mainly regarding the ECG changes.
In conclusion, our results showed that HR, QTd interval, TpTe time, TpTe dispersion, TpTe/QT time and TpTe/QT decreased after bilaterally T3 ETS. Bilateral T3 ETS improved homogeneity of ventricular repolarization may lead to decreased QTd interval, TpTe time, TpTe dispersion, TpTe/QT time and TpTe/QT. ECG data demonstrated the effectiveness of the operation. Further studies are needed to evaluate the importance of ECG parameters in bilateral T3 ETS.
Conflicts of Interest: None.
References
- Is T3 and T6 sympathetic clipping more effective in primary palmoplantar hyperhydrosis? Thorac Cardiovasc Surg. 2011;59:357-9.
- [Google Scholar]
- Right axillary sweating after left thoracoscopic sypathectomy in two-stage surgery. J Clin Anal Med. 2013;4(Suppl 3):261-2.
- [Google Scholar]
- The effects of clipping on thoracic sympathetic nerve in rabbits: Early and late histopathological findings. Thorac Cardiovasc Surg. 2012;60:280-4.
- [Google Scholar]
- Long-term results of bilateral endoscopic thoracic sympathectomy for palmar and axillary hyperhidrosis: An eight-year experience. Turk Gogus Kalp Dama. 2013;21:990-4.
- [Google Scholar]
- The autonomic nervous system of the human heart with special reference to its origin, course, and peripheral distribution. Anat Embryol (Berl). 2005;209:425-38.
- [Google Scholar]
- Cardiac repolarization analysis using the surface electrocardiogram. Philos Trans A Math Phys Eng Sci. 2009;367:213-33.
- [Google Scholar]
- The meaning of the Tp-Te interval and its diagnostic value. J Electrocardiol. 2008;41:575-80.
- [Google Scholar]
- Tpeak – Tend and Tpeak – Tend /QT ratio as markers of ventricular arrhythmia risk in cardiac resynchronization therapy patients. Pacing Clin Electrophysiol. 2013;36:103-8.
- [Google Scholar]
- Henry Cuthbert Bazett (1885-1950) - the man behind the QT interval correction formula. Pacing Clin Electrophysiol. 2011;34:384-8.
- [Google Scholar]
- Endoscopic transthoracic limited sympathotomy for palmar-plantar hyperhidrosis: Outcomes and complications during a 10-year period. Mayo Clin Proc. 2011;86:721-9.
- [Google Scholar]
- Endoscopic thoracic sympathectomy for primary hyperhidrosis of the upper limbs. A critical analysis and long-term results of 480 operations. Ann Surg. 1994;220:86-90.
- [Google Scholar]
- Palmar hyperhidrosis – Which is the best level of denervation using video-assisted thoracoscopic sympathectomy: T2 or T3 ganglion? J Vasc Surg. 2005;42:281-5.
- [Google Scholar]
- The heart rate and ECG changes after endoscopic thoracic sympathectomy in patients with primary hyperhidrosis. Korean J Thorac Cardiovasc Surg. 2009;42:214-9.
- [Google Scholar]
- Cardiopulmonary exercise testing following bilateral thoracoscopic sympathicolysis in patients with essential hyperhidrosis. Thorax. 1995;50:1097-100.
- [Google Scholar]
- Video-assisted sympathectomy for essential hyperhidrosis: Effects on cardiopulmonary function. Chest. 2005;128:2702-5.
- [Google Scholar]
- Bradycardia and permanent pacing after bilateral thoracoscopic T2-sympathectomy for primary hyperhidrosis. Pacing Clin Electrophysiol. 2001;24(4 Pt 1):524-5.
- [Google Scholar]
- Cardiac arrest as a major complication of bilateral cervico-dorsal sympathectomy. Interact Cardiovasc Thorac Surg. 2009;8:238-9.
- [Google Scholar]
- Endoscopic thoracic sympathectomy – Its effect in the treatment of refractory angina pectoris. Interact Cardiovasc Thorac Surg. 2006;5:464-8.
- [Google Scholar]
- Left cardiac sympathetic denervation as the first-line therapy for congenital long QT syndrome. Med Hypotheses. 2004;63:438-41.
- [Google Scholar]
- Cellular basis for the normal T wave and the electrocardiographic manifestations of the long-QT syndrome. Circulation. 1998;98:1928-36.
- [Google Scholar]
- The terminal portion of the T wave: A new electrocardiographic marker of risk of ventricular arrhythmias. Pacing Clin Electrophysiol. 2000;23(11 Pt 2):1957-9.
- [Google Scholar]
- Cellular basis for complex T waves and arrhythmic activity following combined I(Kr) and I(Ks) block. J Cardiovasc Electrophysiol. 2001;12:1369-78.
- [Google Scholar]




