Translate this page into:
Disability adjusted working life years (DAWLYs) of leprosy affected persons in India
Reprint requests: Dr P.S.S. Sundar Rao, Head, Research Resource Centre, TLM Media Centre, B-13 A, Institutional Area, Sector 62, NOIDA, UP 201307, India e-mail: sundarraopss@rocketmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Disability-adjusted life years (DALYs) have been accepted as a useful method to estimate the burden of disease, and can be adapted to determine the number of productive years lost due to the disability. DALY has been reported for many studies but not for leprosy. Hence this study was carried out in three States of India. In view of the fact that in this study, productive working years are used, the term is modified as DAWLY.
Methods:
A representative random sample of 150 leprosy affected persons, 50 from each States of Uttar Pradesh, West Bengal and Chhattisgarh, was chosen, and data were collected on detailed work-life history, occupation, time when leprosy was discovered, reported and treatment started, break of job/loss of income due to leprosy. The loss of wages and durations were used to compute the life-years lost due to leprosy, and summarized over the average total duration of 42 years of productive work-life from 18 to 60 years. The percentage losses were determined and differences tested for statistical significance.
Results:
The overall mean (± SE) disability adjusted working life years was 28.6 (±0.67), a reduction of 13.4 yr from the ideal productive working life period of 42 yr. The youngest patients with disability had a reduction of 41.4 per cent, as compared to the oldest patients. There was a significant increase in loss based on year for those whose disability started earlier (P=0.0024).
Interpretation & conclusions:
On an average, 30 per cent of the leprosy affected person's work life is lost due to disability.
Keywords
DALY
DAWLY
India
leprosy
working life

Leprosy is a chronic mycobacterial disease with primarily skin and nerve manifestations1. The leprosy leads to anaesthetic and paralysed limbs and eyes, disables the person and interferes seriously with the work life2. Recurrent episodes of plantar ulcers and reactions requiring hospital admission and prolonged medical care result in unemployment, loss of wages and social status of the affected person3. With prevailing misconceptions and stigma, these events disable a person physically, socially and economically4. The extent of such economic loss that impacts the livelihood of the affected person has not been reported.
Murray & Lopez5 brought the concept of calculating the burden of disease through disability adjusted life years (DALY)6, to facilitate comparisons of all types of health outcomes. A DALY is a health outcome measure with two main components: quality of life reduced due to a disability, and lifetime lost due to premature mortality. In the process of calculating the DALYs, some weightage is given for specific disability and age discounting also has to be made. The calculation of DALY of a woman who has been deaf since she was 5 and dies when she is 50, with the disability weight of deafness set at 0.33 will be: number of healthy life years × the disability weight of full health (0) + life years with disability (45) × disability weight for deafness (0.33) + life years lost (30) × weighting of death(1) = 5 × 0 + 45 × 0.33 + 30 × 1 = 47.35 DALYs. This estimate will change if the age at which disability occurs and the age of mortality varies.
This idea can be expanded to compute the loss due to both premature disability and mortality or other socio-economic disability67. Thus, the DALY concept can be adapted to estimate the number of productive years lost due to the disability, and can be termed as disability adjusted productive work years lost or disability adjusted working life years (DAWLY). Such ideas have been reported for many studies but not for leprosy589101112. The disability caused by leprosy can be insidious in onset, and the repercussions are seen gradually, and increasing in severity. Unlike in computation of DALY for some diseases, the data for use in the context of leprosy can be subjective, based on recall and many responses biases. However, the concept is a useful one in the context of India's National Leprosy Eradication Programme (NLEP)13, and its application would help in planning and evaluating disability prevention programmes14. Hence, it was proposed to investigate the methodology of computing DAWLY in leprosy affected persons as part of a major research on assessment of post-elimination status of leprosy in India. In this paper, a brief description of the findings is presented with discussion on future research and applications.
Material & Methods
The Indian Council of Medical Research (ICMR), New Delhi, India, sponsored a multicentric study in 2007 in the States of Uttar Pradesh, West Bengal and Chhattisgarh states, to determine the feasibility of establishing a population-based leprosy registry(PBLR), estimate the actual incidence and prevalence through a sample household screening survey, and computation of DALY on a subsample of patients. The superintendents of Leprosy Mission Hospital in Faizabad, U.P., Purulia, West Bengal and Champa, Chhatisgarh along with the Research Resource Centre of the Leprosy Mission planned and implemented the study. The PBLR and the household surveys were successfully completed in three representative rural blocks during the period, June 2007 to September 2010. A total 1281 leprosy affected persons with visible (grade 2) disability were identified in these studies. In order to detect a 40 per cent loss of productive years on an average, with alpha of 0.05, and an error rate of 20 per cent, the minimum sample size was calculated as 150. Therefore, representative stratified random samples of 50 patients from each of the three States were selected for an in-depth interview by a qualified, trained field investigator, using a specially prepared check-list during 2009-10.
Most of the affected persons were unskilled labourers, whose economically productive average age begins at 18 years and continues till 60 years. The interview sought to collect a detailed work-life history from 18 years, chronologically identifying the occupation, income earned, interruptions and changes of jobs, time when leprosy was discovered, reported and treatment started, break of job/loss of income since leprosy was detected and treated, reduction of wages/income from similar employees of the same job, duration of work-loss, re-entry into the work force after any medical/surgical intervention, revised wage and proportionate losses with durations, recording all such details till 60 years of age.
From these data, the loss of wages and durations were computed in life-years lost due to leprosy, and summarized over the total duration of 42 years of productive work-life from 18 to 60 years. The DAWLY was then computed to indicate the reduction from 42 years, and expressed as percentage losses.
Means and standard errors (SE) were computed overall and in relation to specific factors such as age at which disability started, year at which disability started, occupation, etc. Data were entered into Excel sheet and analysed using SPSS 15.0 Windows Evaluation Version. Differences were tested for statistical significances using z, t and ANOVA distributions.
Results
The overall mean DAWLY (± SE) of the disability adjusted life years was 28.6 (±0.67) which indicated a significant (P<0.05) reduction of 13.4 years or 31.9 per cent from the ideal productive period of 42 years. The 95 per cent of DAWLY confidence interval was 27.22 to 29.88.
The mean (± SE) of DAWLY, the 95 per cent confidence interval as well as the per cent reduction in life years according to the age when disability started, are depicted in Table I.
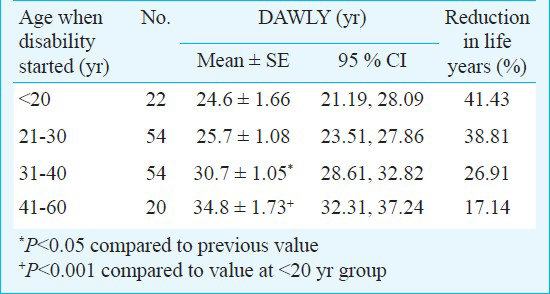
The patients in <20 yr age group when disability started had a DAWLY of 24.6 years, a reduction of 41.43 per cent, as compared to the patients in 41-60 yr age group, who had a DAWLY of 34.8 yr, only a reduction of 17.14 per cent in the life years. This difference was significant (P<0.001). The mean DAWLY, the 95 per cent confidence interval as well as the per cent reduction in life years according to the year when disability started, is given in Table II.
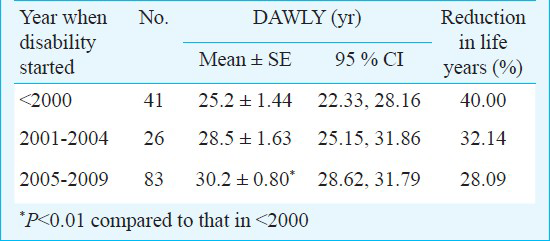
The patients who were affected by leprosy before the year 2000 had a DAWLY of 25.2 yr, a reduction of 40 per cent, as compared to the patients affected with leprosy after 2005 having a DAWLY of 30.2 yr, a reduction of 28.09 per cent in the life years. This change in loss was significant (P<0.01).
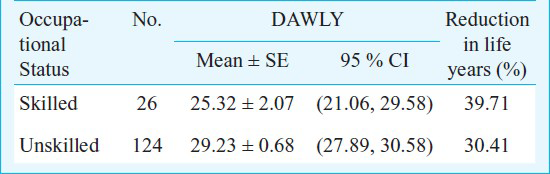
Among 150 leprosy patients, 124 (82.67%) were unskilled labourers. Most of the leprosy patients were farmers, or labourers, and a few were beggars.
The mean of DAWLY, the 95 per cent confidence interval as well as the per cent reduction in life years according to the occupational status, is given in Table III. The patients in skilled occupations had a DAWLY of 25.32 yr, a reduction of 39.71 per cent, as compared to the unskilled patients, who had a DAWLY of 29.23 yr, a reduction of 30.41 per cent in the life years. This difference was not significant.
Discussion
Between 5 to 10 per cent of Indians have some impairment or disabling condition, which means that India has a huge population of disabled people (GOI, Census 2001). India needs to make a shift from the medical model of intervention to community-based rehabilitation of the disabled15. The computation of DAWLY provides an indicator that can be used to assess current status and impact of interventions. Despite all the limitations, DAWLY, as computed seems simple, easily understood, and a useful parameter.
One of the tasks undertaken by personnel working with leprosy patients is the socio-economic rehabilitation (SER) of leprosy patients with disability. This has been listed as a priority area for leprosy programme planners16. In a situation where economic resources are limited and the numbers of people with disability are large17 the process of rehabilitation needs to be targeted to those most in need.
The DALY, as originally conceived, has become increasingly useful in the field of public health and health impact assessment (HIA) because it integrates the years of life loss (YLL) with the years lived with disability (YLD). In the case of leprosy both the terms are relevant since patients may either absent by themselves or loss the jobs as well as continue to work at lower that optimal performance due to the disability. Findings from this research indicate that leprosy reduces the productive working life time period by at least 30 per cent, and therefore, highlights the need for some action to increase productivity.
Unlike calculation of traditional DALY based on evidence of mortality and severe morbidity, the DAWLY used in this study relies on subjective information on absents and irregularity in economically productive or remunerative work. There might be considerable reduction in reliability of data depending on the skills of the interviewer as well as the commitment and co-operation of the respondent. Both these conditions can be handled through proper training of the investigator and suitable undisturbed environment to carry out the interview.
Despite the availability of suitable therapy, many patients still delay treatment till visible disabilities occur and the affected person is unable to perform his normal work181920. The findings of the study showed that on an average one third of the patients work life is lost due to leprosy.
The operational definition of DAWLY as used in this research may need further refinements to make it more sensitive in measuring the leprosy burden. A prospective cohort study rather a retrospective one may be more reliable and valid to indicate not only the time lost due to a disability but also the time regained after reconstructive surgery and other therapeutic intervention. More studies are needed to make DAWLY a better tool.
Acknowledgment
Authors acknowledge the Indian Council of Medical Research, New Delhi and The Leprosy Mission International, UK, for financial support. Authors thank the private practitioners, medical officers of PHC/CHCs, for cooperation, the TLM staff for providing necessary data, and the State and District Leprosy Officers for guideline. Authors also thank all the field investigators and the data entry operators for their hard and sincere work.
References
- Disability index of hands and feet in patients attending an urban leprosy clinic. Indian J Lepr. 1990;62:328-37.
- [Google Scholar]
- Measuring stigma – a preliminary review of the leprosy literature. Int J Lepr Other Mycobact Dis. 2003;71:190-7.
- [Google Scholar]
- Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997;349:1436-42.
- [Google Scholar]
- The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990 and projected to 2020. In: Murray CJL, Lopez AD, eds. Global burden of disease and injury series. Vol 1. Cambridge MA: Harvard University Press; 1996.
- [Google Scholar]
- Burden of chikungunya in India: estimates of disability adjusted life years (DALY) lost in 2006 epidemic. J Vector Borne Dis. 2009;46:26-35.
- [Google Scholar]
- Measuring the burden of disease using disability-adjusted life years in Shilin County of Yunnan Province, China. Environ Health Prev Med. 2011;16:148-54.
- [Google Scholar]
- The contribution of reproductive ill-health to the overall burden of perceived illness among women in southern India. Bull World Health Organ. 2001;79:1065-9.
- [Google Scholar]
- Calculating and presenting disability adjusted life years (DALYs) in cost-effectiveness analysis. Health Policy Plan. 2001;16:326-31.
- [Google Scholar]
- WHO. Global leprosy situation, beginning of 2008. Wkly Epidemiol Rec. 2008;83:293-300.
- [Google Scholar]
- WHO. Report of the global forum on elimination of leprosy as a public health problem. In: WHO/CDS/NTD/2006.4. 2007.
- [Google Scholar]
- Government of India, Registrar General. In: Census 2001. New Delhi: Govt. of India; 2001.
- [Google Scholar]
- WHO. Death and DALY estimates for 2004 by cause for WHO Member States : Persons, all ages. 2002. Available from: http://www.who.int/entity/healthinfo/global_burden_disease/gbddeathdalycountryestimates2004.xls
- [Google Scholar]
- Methodological choices for calculating the disease burden and cost-of-illness of foodborne zoonoses in European countries. 2007. Available from: http://ctsu.nottingham.ac.uk/idea2008/docs/Report_07-002%20Cost%20of%20Illness.pdf
- [Google Scholar]
- Trends in detection of new leprosy cases at two centers in Himachal Pradesh, India: A ten year study. Indian J Lepr. 2003;75:17-24.
- [Google Scholar]
- Delay in presentation and start of treatment in leprosy patients: a case-control study of disabled and non disabled patients in three different settings in Ethiopia. Int J Lepr other Mycobact Dis. 1998;66:1-9.
- [Google Scholar]




