
Translate this page into:
Diffuse large B-cell lymphoma presenting as shoulder swelling
*For correspondence: manne.sappu@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 53 yr old male† diabetic patient presented to the Oncology division of Medicine department of GSL Medical College and General Hospital, Rajahmundry, India, in June 2017 with a swelling of three months duration over the posterior aspect of the right shoulder (Fig. 1A). The swelling was associated with pain and limitation of shoulder movements. His general physical examination was normal, except for right axillary and supraclavicular lymphadenopathy. On clinical examination, the diagnosis was soft-tissue sarcoma/osteosarcoma/Ewing's sarcoma. Radiograph of the right shoulder revealed a large swelling on the posterior aspect obscuring the lateral border of the scapula. Computed tomography (CT) imaging of the right shoulder revealed a large soft-tissue mass with permeative destruction of the right scapula and enlarged axillary and pectoral lymph nodes (Fig. 2A). Peripheral smear examination and bone marrow study were normal. CT imaging of the abdomen and chest revealed no lymphadenopathy. Histopathological examination of the lymphoid tissue revealed diffuse proliferation of large lymphoid cells which are round to polygonal with single prominent eosinophilic nucleolus and ample amphophilic cytoplasm suggestive of diffuse large B-cell lymphoma (DLBCL). Immunostaining of sections of the axillary lymph node for CD45 and CD20 was positive, suggesting non-Hodgkin's lymphoma (NHL) of diffuse large B-cell subtype (Fig. 3A and B). Hence, the final diagnosis of NHL diffuse large B-cell subtype stage IIAX was made. Six cycles of immunochemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone regimen were given followed by involved-field radiotherapy with 6 MV (megavoltage) photon beams at a dose of 39.5 Gy in 22 fractions. There was a significant reduction in the size of the tumour mass (Fig. 1B and 2B) with improvement in shoulder pain and movements at 18 months of follow up.
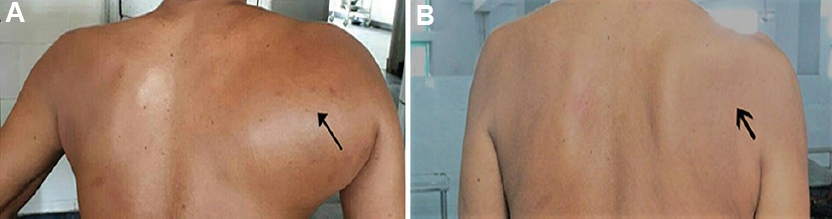
- (A) Arrow shows swelling on the posterior aspect of the right shoulder. (B) Arrow shows reduction in the size of swelling after six cycles of chemotherapy and involved-field radiotherapy.
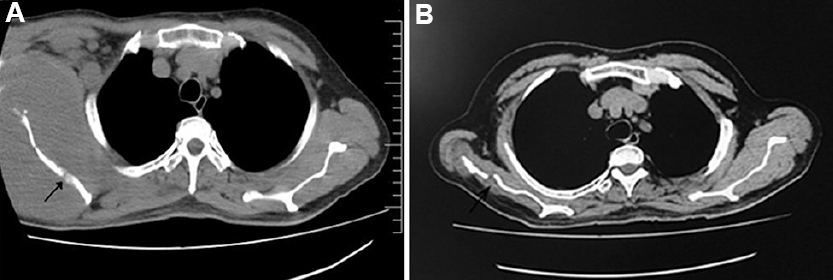
- (A) Arrow in the axial section of the computed tomography image of the right shoulder shows a large soft-tissue mass with permeative destruction of the right scapula and enlarged axillary and pectoral lymph nodes. (B) Arrow in the axial section of the computed tomography image of the right shoulder shows regression of the soft-tissue mass with immunochemotherapy and radiotherapy.
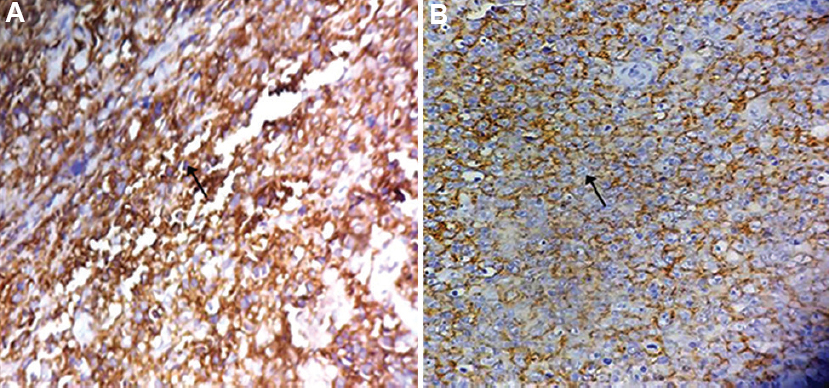
- (A) Immunostaining of the tissue section shows positive membrane staining of CD45 in 85 per cent cells as shown in brown colour suggestive of non-Hodgkin's lymphoma as pointed by the arrow mark. (B) Immunostaining of the tissue section shows positive membrane staining of CD20 in 65 per cent cells as shown in brown colour suggestive of diffuse large B-cell lymphoma as pointed by the arrow mark.
Conflicts of Interest: None.




