Translate this page into:
Deworming conundrum - Are we missing an undesirable dimension?
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Parasitic helminths include soil transmitted helminth (STH) parasites such as Ascaris, Trichuris, hookworms and tissue invasive-systemic helminths like filarial and Schistosome parasites. They cause severe morbidity in both humans and animals and continue to pose serious challenges to the economic welfare and public health in most of the developing countries in the world. The global burden of infections caused by these STH parasites is estimated to be responsible for loss of 39 million life years of disability adjusted life years (DALYS)1, comparable to the burden of all other major diseases afflicting the human communities. In children, STH are reported to adversely affect appetite, nutritional status, healthy growth, cognitive development, physical fitness, and clinical outcome of malaria, tuberculosis, or AIDS and are reported to affect adversely their immunological responses to vaccines23.
Current deworming policies of global agencies for STH infections
The WHO has been advocating deworming the population at risk, particularly school age children (SAC) to meet the Millennium Development Goals (MDG). Currently, only about 10 per cent of SAC and 20 per cent of preschool children who are at risk of acquiring intestinal helminth infections are dewormed4 against the target set by WHO to regularly treat at least 75 per cent of SAC at risk of morbidity5. Despite the arguably limited hard evidence in favour of deworming and its benefits to the community, population based mass drug administration (MDA) has been promoted as a cost-effective measure to reduce the disease burden of STH infections. Since increasing the coverage to large populations and its sustainability requires large global investment, evaluating the benefits of deworming has become critical. Based on a meta-analysis of 41 double-blind clinical trials covering 65,168 participants on the outcomes viz., haemoglobin status, growth, cognitive abilities and school attendance67, the wisdom of deworming several million children has been questioned because there was a mismatch between the state of reliable direct evidence of benefit and the benefit claimed by the advocates of deworming. Bundy et al8, however, raised methodological issues on the Cochrane review and conclusions drawn from it and have argued in favour of continuing the currently practiced deworming strategy. Engels and Savioli9 while strongly recommending deworming, have commented that public health policy setting has to go beyond the issue of whether a sacrosanct level of statistical significance is reached on a limited number of (multifactoral) outcomes in a series of carefully selected studies. Hotez et al4 recommended inclusion of deworming programmes in the national health plans and constitutional provisions to declare deworming mandatory at least in STH endemic countries.
What is ignored in the ongoing debate on deworming in STH infections?
The issue of nematode egg load in soil/environment as a result of large scale deworming in human communities does not appear to be a factor seriously being debated although rapid re-infection in dewormed population has been shown to be a factor standing contamination of worms in the environment10. The proposal here is that “Deworming one segment of people in a community could predispose the untreated population to enhanced worm infections and its adverse consequences”. The reasoning is that the net viable and infective nematode egg pool in soil and environment would increase many fold following deworming and this could lead to previously uninfected subjects acquiring infections and/or could increase worm load in subjects already harbouring infections amongst the untreated population in the community. Deworming leads to expulsion of adult worms which harbour large number of viable eggs and is also known to enhance egg output in stool samples11. Eggs expelled by dewormed subjects and by untreated population are equally infective12 and find their way into the environment through untreated or improperly treated sewage and also through open defecation by people in many developing countries with poor sanitation. Use of digested sludge and human excreta as a fertilizer to replenish agricultural soil has been a common practice of waste disposal even in developed countries13 and treatment of raw sewage including human excreta by mesothermic anaerobic or aerobic digestion eliminates other parasites but many nematode eggs retain their viability and infectivity after digestion14. Ascaris eggs which have a four layered shell are resistant to adverse climatic conditions, potentially survive in soil for up to 7-10 years1415 and are being used as a conservative biological indicator organism for monitoring and evaluation of sludge treatment efficiency and sanitation processes15. Not surprisingly dewormed subjects rapidly get re-infected in endemic countries. The magnitude of reinfection is very high as shown by a meta-analysis of 24 studies, even after deworming the whole community16 which is attributable to standing contamination of worms in the environment10.
Evidence for the flip side of deworming to STH infections in untreated subjects
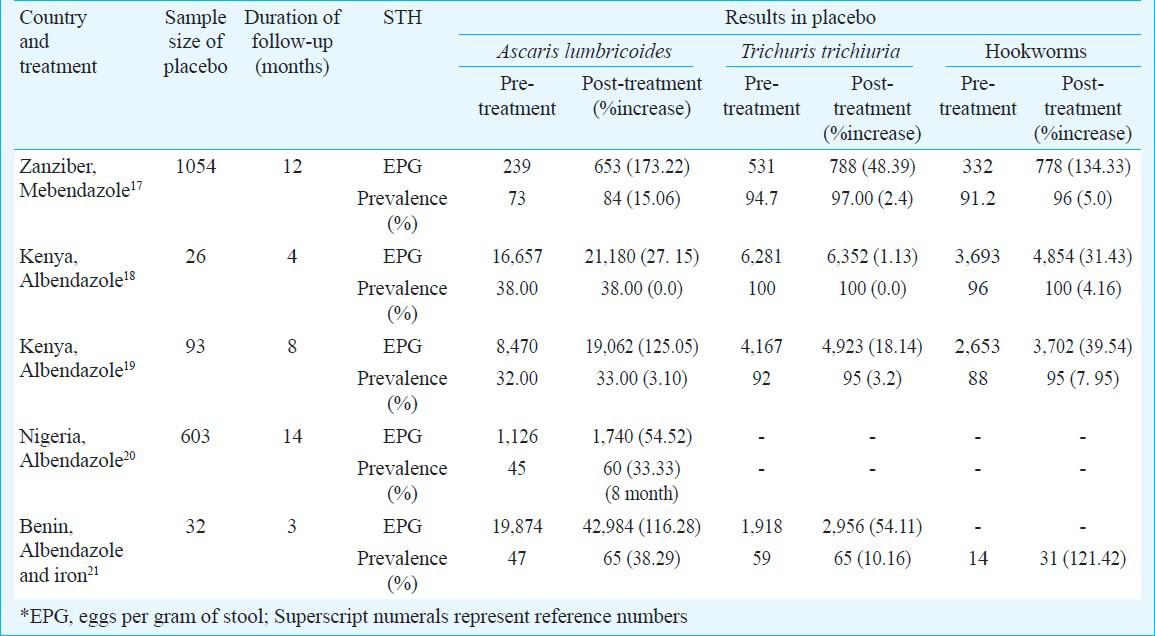
In the absence of evidence in literature to establish enhanced nematode egg load levels in environment following treatment with anti-helminth drugs, proof was sought by examining some of the published reports of randomized controlled trials (RCTs) on deworming. Unlike the original authors who evaluated the effect of deworming in drug treated subjects, outcome indicators in placebo groups were analysed for writing this ‘viewpoint’. Studies conducted in areas with high intensity of infection in which treated and untreated groups were followed up for a longer duration (three months or more) were included for this analysis. The assumption was that the excreted nematode eggs expelled by dewormed subjects in rural communities would be available to infect and establish new infections in the placebo group. The analysis summarized in the Table reveals that the treatment of one cohort with anti-helminth drugs results in increased worm infections (as shown by eggs per gram of stool) in the untreated cohort and in some instances leads to increased prevalence of infections amongst placebo treated subjects. The most revealing observations were published by Stephenson et al19 and using the authors’ data the status of egg load and body weight in treated and placebo groups were re-analysed. Loss of hookworm infection in treated group was matched by gain of infection in the placebo group over a period of eight months after administration of two doses of albendazole to the treated group; similarly gain in body weight in the dewormed group matched closely with loss of body weight in the untreated group. The combined hookworm egg load in treated and placebo groups put together was comparable before and eight months after deworming – eggs lost by treated subjects were gained by the placebo group. Increase in intensity of STH infection was associated with a decreased appetite in untreated children in one study18. Increased worm infections were also associated with a decrease in anthropometric parameters such as weight for age, weight for height, arm circumference, triceps skinfold in placebo treated subjects1819. These observations can be interpreted to mean that in the absence of deworming, untreated subjects continue to get exposed to fresh infections and consequently acquire more infections leading to an increase in egg load. It can also be interpreted to suggest that as a consequence of deworming, the nematode egg load in the environment increases and the effect of such increase gets reflected as enhanced prevalence and/or egg count and consequent adverse effects in the placebo treated group. To rule out the former interpretation evidence for no significant change in intensity or prevalence in longitudinal data from these or similar populations will be required. Such studies are needed while designing RCTs for deworming. Further, all RCT studies listed in the Table have been carried out in Africa which raises questions on their applicability at the global level. Well designed long-term studies need to be conducted in different geographical areas covering different climatic zones, including India to authenticate the observations made in African children. It is also important to note that adverse effects in placebo treated subjects were not observed when deworming was undertaken in areas of low infection prevalence or intensity2223 or when a very large proportion of the population (>90%) received frequent doses of treatment23 or when deworming by MDA was undertaken in an area with low intensity of infection24. Similarly, when the duration of follow up was short (21 days), there was no increase in intensity of infection in placebo treated subjects2225 - this is expected since the average time required for ingested eggs of enteric parasites to transform into gravid females, ready to lay eggs inside an infected host, is about 8-12 wk.
Concluding remarks
Interpretation of published reports summarized in the Table suggests that many of the reported and possibly ongoing RCTs on deworming suffer from a flawed study design since outcome indicators such as infection prevalence, infection intensity, anthropometric indices, appetite, haemoglobin level, etc., tend to get worse in placebo treated groups in comparison to pretreatment baseline levels. This observation needs to be validated by re-designing RCTs under field conditions in drug and placebo treated cohorts along with other appropriate controls to avoid possible confounders.
In 2001, the World Health Assembly passed a resolution urging Member States to control the morbidity of STH infections through large scale use of anti-helminthic drugs for school aged children26. The current approach of targeting a restricted group with high prevalence and intensity of infection may not yield desired results since it has the risk of shifting the burden of intestinal helminths from treated to untreated subjects in the community. Further, successful deworming programmes in human communities need to consider the issue of nematode egg survival in soil. However, existing drugs could still be used effectively to control STH in areas of high intensity infections by enhancing treatment frequency and mass coverage of the population for durations much longer than nematode egg viability in soil/environment. Considering the emergence of helminth strains resistant to available drugs2728 and the imminent selection pressure of MDA programmes on the life history of parasitic worms leading to their increased per capita fecundity2930, there is an urgent need to explore alternative approaches for development of novel chemotherapeutic drugs against parasitic helminths. One approach is to develop drugs that block embryogenesis in pathogenic nematodes which could inhibit transmission and re-infection with STH in human communities31.
References
- Rescuing the bottom billion through control of neglected tropical diseases. Lancet. 2009;373:1570-5.
- [Google Scholar]
- Controlling soil transmitted helminthiasis in pre school age children through preventive chemotherapy. PLoS Negl Trop Dis. 2008;2:e126.
- [Google Scholar]
- Intestinal nematodes: disease burden, deworming and the potential importance of co-infection. Curr Opin Infect Dis. 2008;21:516-22.
- [Google Scholar]
- Does deworming improve growth and school performance in children. PLoS Negl Trop Dis. 2009;3:e358.
- [Google Scholar]
- Deworming drugs for soil-trasmitted intestinal worms in children: effects on nutritionnel indicators, haemoglobin and school performance. Cochrane Library (7) No. 000371
- [Google Scholar]
- Deworming and development: asking the right questions, asking the questions right. PLoS Negl Trop Dis. 2009;3:e362.
- [Google Scholar]
- The epidemiology and control of intestinal helminthes in the Pulicat Lake region of Southern India. I. Study design and pre- and post treatment observations on Ascaris lumbricoides infection. Trans R Soc Trop Med Hyg. 1986;80:774-92.
- [Google Scholar]
- Evaluation of marked rise in fecal egg output after Bithionol administration to horse and its application as a diagnostic marker for equine Anocephalaperfoliata infection. J Vet Med Sci. 2009;71:617-20.
- [Google Scholar]
- Embryonation and infectivity of Ascarissuum eggs isolated from worms expelled by pigs treated with albendazole, pyrantel pamoate, ivermectin or piperazine dihydrochloride. Vet Parasitol. 1998;75:181-90.
- [Google Scholar]
- Inactivation of Ascaris eggs in source separated urine and feces by ammonia at ambient temperatures. Appl Env Microbiol. 2009;75:662-7.
- [Google Scholar]
- Survival of parasite eggs upon storage insludge. Appl Env Microbiol. 1984;48:618-25.
- [Google Scholar]
- Survival rates of parasite eggs in sludge during aerobic and anaerobic digestion. Appl Env Microbiol. 1982;44:1138-43.
- [Google Scholar]
- Soil-transmitted helminth reinfection after drug : A systematic review and meta-analysis. PLoS Negl Trop Dis. 2012;6:e 1621.
- [Google Scholar]
- School based deworming program yields small improvement in growth of zanzibari school children after one year. J Nutr. 1997;127:2187-93.
- [Google Scholar]
- Physical fitness, growth and appetite of Kenyan school boys with hook worm, Trichuris trichiura and Ascaris lumbricoides infections are improved four months after a single dose of albendazole. J Nutr. 1993;123:1036-46.
- [Google Scholar]
- Weight gain of Kenyan school children infected with hook worm, Trichuris trichiura and Ascaris lumbricoides is improved following once or twice yearly treatment with albendazole. J Nutr. 1993;123:656-65.
- [Google Scholar]
- Patterns of soil transmitted helminth infection and impact of four monthly albendazole treatments in preschool children from semi urban communities in Nigeria: a double blind placebo controlled randomized trial. BMC Infect Dis. 2009;9:20.
- [Google Scholar]
- Impact of iron supplementation and deworming on growth performance in preschool Beninese children. Eur J Clin Nutr. 2001;55:223-8.
- [Google Scholar]
- Low efficacy of mebendazole against hookworms in Vietnam: two randomized control trials. Am J Trop Med Hyg. 2007;76:732-6.
- [Google Scholar]
- Control of geo-helminths by delivery of targeted chemotherapy through schools. Trans R Soc Trop Med Hyg. 1990;84:115-20.
- [Google Scholar]
- Parasitological impact of 2- year preventive chemotherapy on schistosomiasis and soil transmitted helminthiasis in Uganda. BMC Med. 2007;5:27.
- [Google Scholar]
- Efficacy of mebendazole and levamisole alone or in combination against intestinal nematode infections after repeated targeted mebendazole treatment in Zanzibar. Bull World Health Organ. 2003;81:343-52.
- [Google Scholar]
- Drug resistance mechanisms in helminths: is it survival of the fittest? Trends Parasitol. 2009;25:328-35.
- [Google Scholar]
- Drug resistance in human helminthes: current situations and lesions from livestock. Clin Microbiol Rev. 2009;13:207-22.
- [Google Scholar]
- Experimental evolution of parasite life history traits in Strongyloides ratti (Nematoda) Proc R Soc B. 2007;274:1467-74.
- [Google Scholar]
- Caspase dependent programmed cell death in developing embryos: A potential target for therapeutic intervention against Pathogenic Nematodes. PLoS Negl Trop Dis. 2011;5:e1306.
- [Google Scholar]




