Translate this page into:
Determinants of Indian physicians’ satisfaction & dissatisfaction from their job
Reprint requests: Dr Pramod K. Gupta, Assistant Professor, Department of Biostatistics, Postgraduate Institute of Medical Education & Research, Chandigarh 160 012, India e-mail: pk_guptain@yahoo.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Physicians’ satisfaction/dissatisfaction from their job is an important factor associated with health service that deals with human life. This study was conducted to ascertain overall level and proportion of physicians’ satisfaction from their job as well as to identify those components that influenced it.
Method:
A comprehensive customized questionnaire was used with Section A to assess demographic profile of physicians and Section B to assess satisfaction. Response to each question was devised using Likert scale. Likert scale responses were converted to normal scale so that statistical procedures could be naturally developed. A total of 170 physicians were selected using multistage sampling. Questionnaire was administered on one to one basis to avoid non-response. Precise and contextualized descriptive and inferential statistical procedures were used for analysis.
Result:
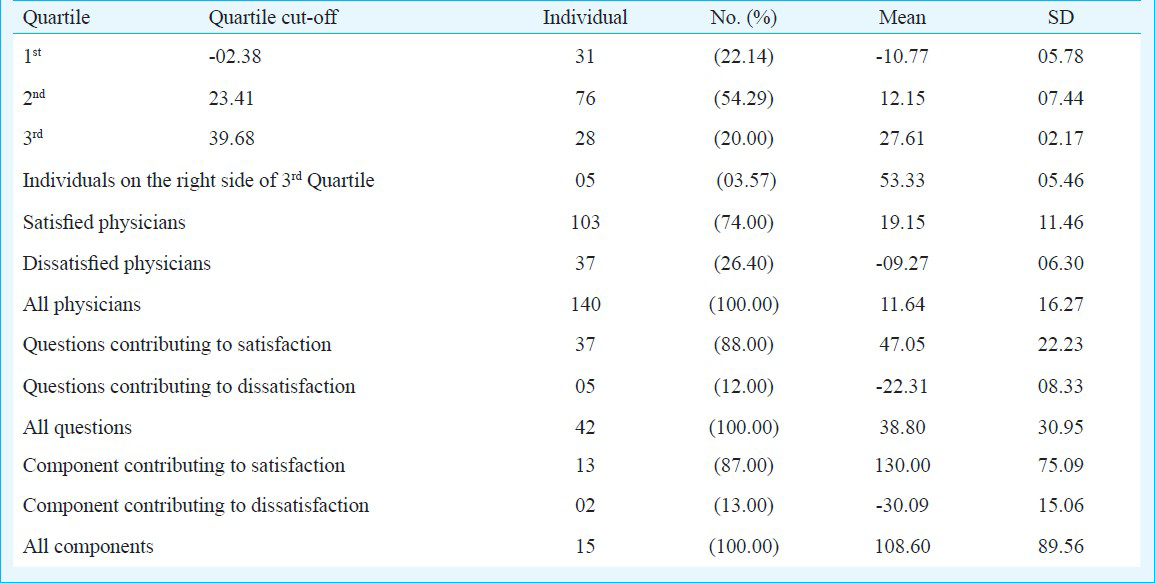
Of the 140 physicians, 103 (74%) were satisfied from their job with average score of 19.15 ± 11.46 while 37 (26%) were dissatisfied with average score -09.27 ± 06.30. Nine out of 15 components were found significant (P<0.05).
Conclusion:
Comparative assessment of the present results with those of other studies revealed that satisfaction percentage of Indian physicians and those of the developed countries were almost the same. Perhaps, magnitude of satisfaction level (average score) of the Indian physicians were towards the lower side. Nine determinants, identified in this study can be used safely to assess any professionals’ satisfaction.
Keywords
Factor analysis
Likert Scale
multistage sampling
satisfaction
variable selection

Satisfaction/dissatisfaction of professionals from their job is an important issue that influences their health, progress, performance, and development and it may also affect their serving institution/employer/organization. In this context, the physicians’ satisfaction/dissatisfaction from their job becomes more decisive because it directly affects health care system of any country, which is associated with vital issues of its people. Hence, disclosures of physicians’ condition is also important and of utmost interest for every institution. The physiology of individuals’ satisfaction/dissatisfaction is a multi regulatory phenomenon, which depends on various factors like individual's perception, environment, opportunities, etc., and is therefore, complex to understand. Hence, a systematic and scientific procedure was sought that could explain these complexities. Two studies have discussed physicians’ characteristics influencing patient adherence to medical treatment, which leads to reduction in the quality of patient care12. Keeton et al3 focused on the identification of the predictors for satisfaction/dissatisfaction of physicians. Other studies have evaluated reason of strike attempts by Germen physicians and satisfaction and dissatisfaction of Egyptian physicians45. These studies disclose many facts and work as an alarming system. For example, low level of satisfaction (dissatisfaction) from job may cause high level of stress, which could eventually be detrimental to physical/ mental health and quality of life. Hence, dissatisfaction from job may lead to increase in conflict, absenteeism, low patient care rate and reduction in quality and quantity of work67. Physician's job satisfaction is interrelated to patient satisfaction, patient compliance, and continuity of care8. Studies also reveal that dissatisfaction induces lower productivity and increased turn over, which eventually raises costs of the medical services910.
Various studies have been conducted throughout the world under different set-ups11121314. All these studies focus not only to estimate level and proportion of satisfaction/dissatisfaction among physicians but also to identify indicators/predictors that governed its physiology. The present study was conducted among Indian physicians to assess the level of satisfaction from their job as also to identify the factors influencing it.
Material & Methods
A cross-sectional prospective survey was conducted during May-December 2009 in the School of Public Health, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India, using a comprehensive customized questionnaire (Appendix).
Sample size & sampling procedure: Sample size was computed considering that individual physician on average scored 60 ± 15 per cent of total satisfaction score under 95% confidence interval [level of significance (α) =0.05]. Computations showed that approximately 170 physicians were required. Multistage sampling procedure was followed. At the first stage, Chandigarh city of India was selected using non-probability method of sampling, particularly purposive/convenience sampling. At the second stage, two medical institutes [PGIMER and Government Medical College & Hospital (GMCH)] were selected using non-probability method of sampling. At the third stage, proportionate sampling (PPS) method was used to determine proportion of sample that has to be drawn from these two selected institutes to enrol 170 physicians. Comprehensive details of all faculty and resident doctors were obtained from both the institutions after administrative approval. A total of 1474 physicians, comprising 1082 (73%) from PGIMER and 392 (27%) GMCH were available on record at that time.
At the fourth and the last stage, systematic sampling procedure was used to select 124 and 46 names of physicians from their details obtained from PGIMER and GMCH, respectively. Individual list for both the institutions was prepared from the available details and sorted over physicians’ name. Names were selected following the regular interval of 9-names starting from first. In case of non-response and/or non-availability of selected name, next successive name was selected.
Data analysis: Summary-statistics were obtained for socio-economic variables of Part-A as well as for questions/component of Part-B of the questionnaire using appropriate descriptive statistics depending on types of variable for all 170 physicians. However, only 140 observations were used in further analysis. All data analyses were done using R-Gui statistical software version 2.13 on windows (R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/).
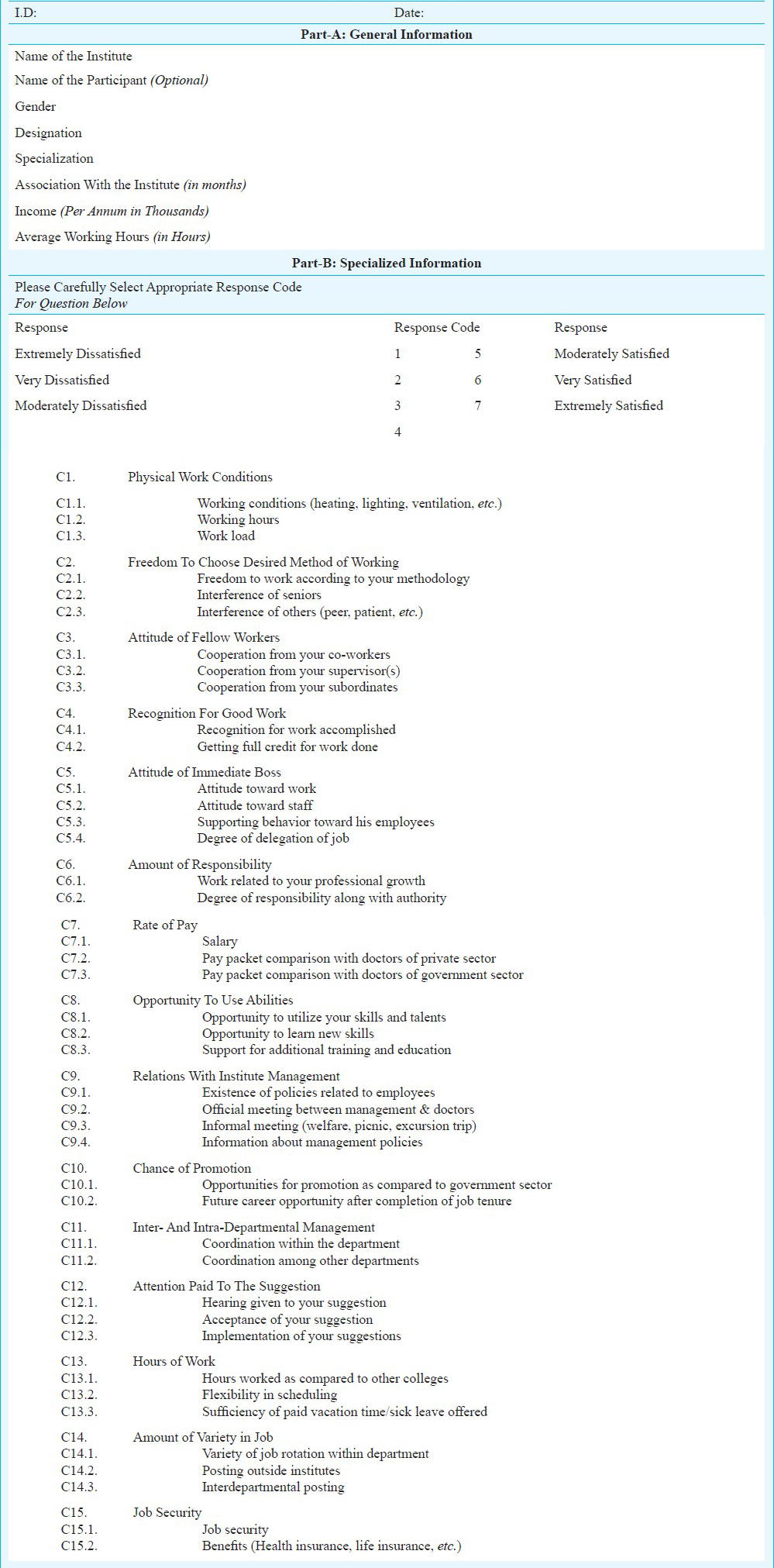
Questionnaire/tool: The questionnaire was divided into two sections. Section-A was meant to assess demographic profile of physicians, and Section-B to assess satisfaction; and 42-questions were developed under 15 distinguished heads15. Each head was developed in such a way that its questions explored extrinsic and intrinsic factors of physicians’ satisfaction/dissatisfaction from their job. Heads like physical work conditions, relationship with fellow workers, boss's attitude, pay, promotion, management relationship, job security, etc. were a few examples that could extract overall information on financial, intellectual, social satisfaction/dissatisfaction (Appendix).
Response to each question in the questionnaire was devised using Likert scale16 that provides 7-options for respondent (1= extremely dissatisfied; 2= very dissatisfied; 3= moderately dissatisfied; 4= not sure; 5= moderately satisfied; 6= very satisfied; 7= extremely satisfied. Likert scale was considered in this study to avoid non response for question, providing sufficient and appropriate option to respondent for almost every question. Hence, data collected for given purpose could be utilized to full extent during outcome analysis.
The study protocol was approved by Institute's Ethics Committee.
Exclusion/inclusion criteria & anonymity: Only those physicians were included in the study who had completed at least six months period at the present institution. Otherwise, successive name from the list was considered. Those who did not return the filled questionnaire even after three visits or within a week, were replaced by successive names from the list. To preserve the anonymity of the participants, first 15 to 20 participants were asked to place the filled questionnaire in the sealed box. The remaining participants placed the questionnaires within randomly selected (15-20) previously filled boxes and reshuffled.
Composite scores for satisfaction and dissatisfaction either for physicians or for question and components were computed after transforming 7-points Likert response into normal scale. The normal scale distinguished satisfaction and dissatisfaction at either (positive & negative) side of zero.
Individual's composite score was computed by sum over corresponding row and satisfaction/dissatisfaction was understood by its positive/negative value. Composite score for each question was computed by sum over corresponding column and positive/negative over score determined its contribution. Similarly, composite score for each component was computed first by adding the score of all corresponding question followed by sum over column.
A novel quartile-statistics based strategy was used to find the number/percentage/proportion of satisfied physicians rather than self decided cut-off. Questions and components significantly associated with satisfaction/dissatisfaction were obtained using Chi square (χ2)-test/Fisher exact test of association at α = 0.05. Association of socio-economic variables in Part-A of questionnaire with satisfaction/dissatisfaction was also studied.
Principal Component Analysis (PCA) and variable selection statistical procedure were used to find significant indicators associated with satisfaction/dissatisfaction. Variable selection was conducted using generalized linear model (GLM) with binomial link function. GLM was performed using individuals’ composite score as dependent variable and 15-components as independent variables and further extended by incorporating variables of Part-A with 15-components.
The best model through GLM was selected on the basis of Akaike information criterion (AIC).
Results
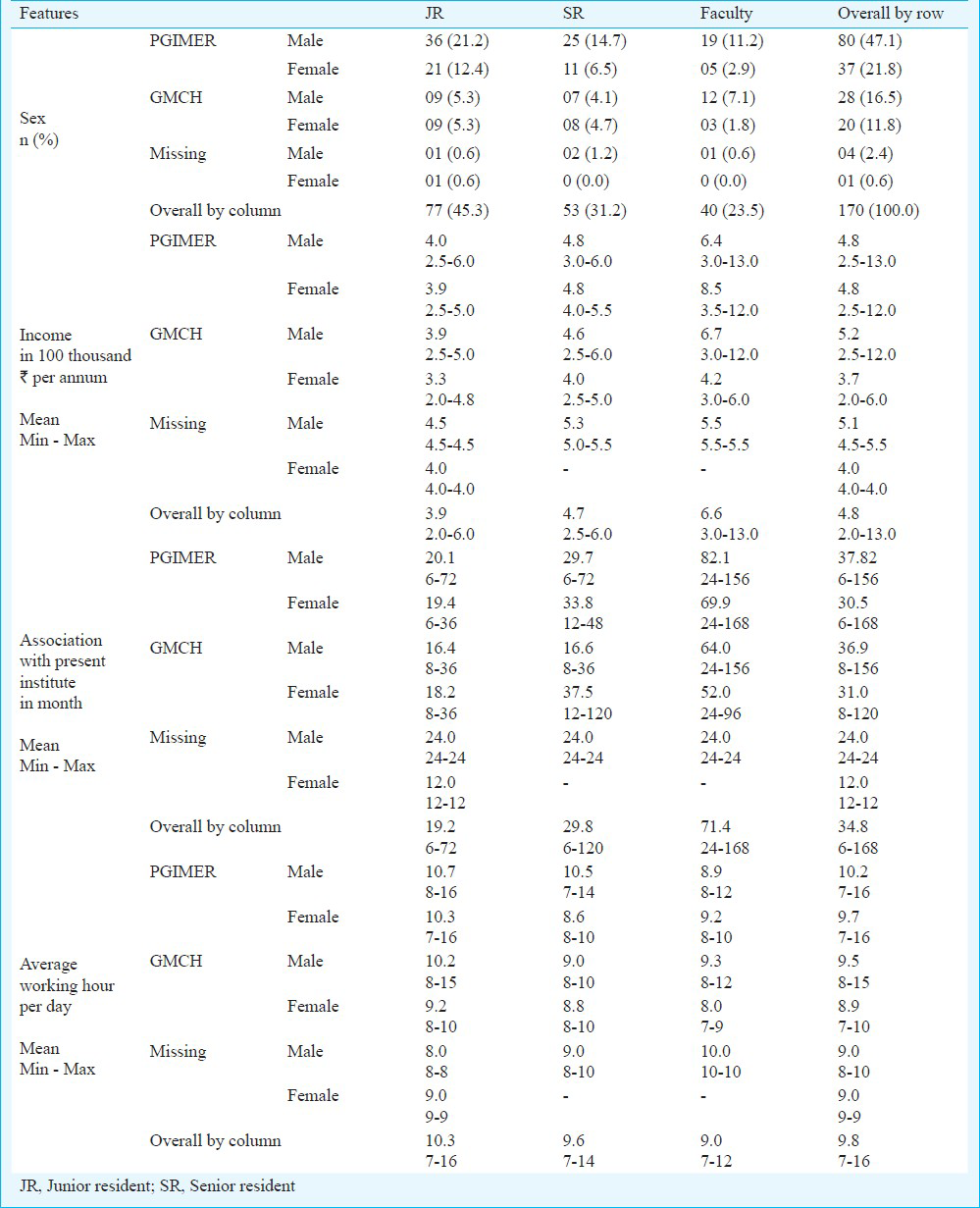
The male physicians 47.1 per cent (80) were almost twice than female physicians 21.8 per cent (37) working at PGIMER (Table I). Composite score of physicians disclosed that 74 per cent (103) physicians were satisfied while 26 per cent (37) physicians were dissatisfied from their jobs. Figs 1 and 2 displayed distribution of composite scores, which clearly depicted that only a few physicians were on extreme side of the distribution. The average scores of satisfied and dissatisfied physicians from their job were recorded as 19.15 ± 11.46 and -09.27 ± 06.30, respectively (Table II). Only five physicians scored more than 40 out of 58.33, while only one physician scored minimal. Fig. 3 shows distribution of grading of physicians’ composite score based on quartile statistics and clearly distinguished the physicians’ group according to their satisfaction level.
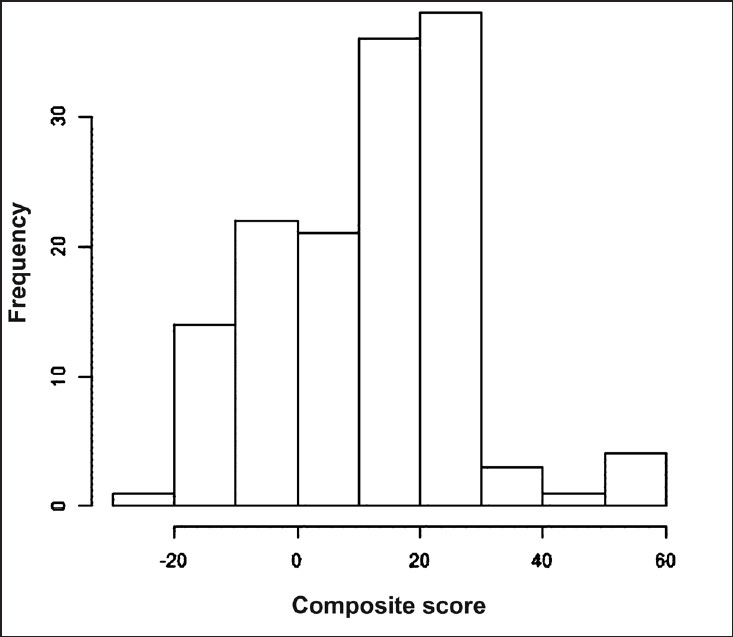
- Composite (average) score of physicians’ satisfaction and dissatisfaction that revealed distribution pattern which is not normally distributed.
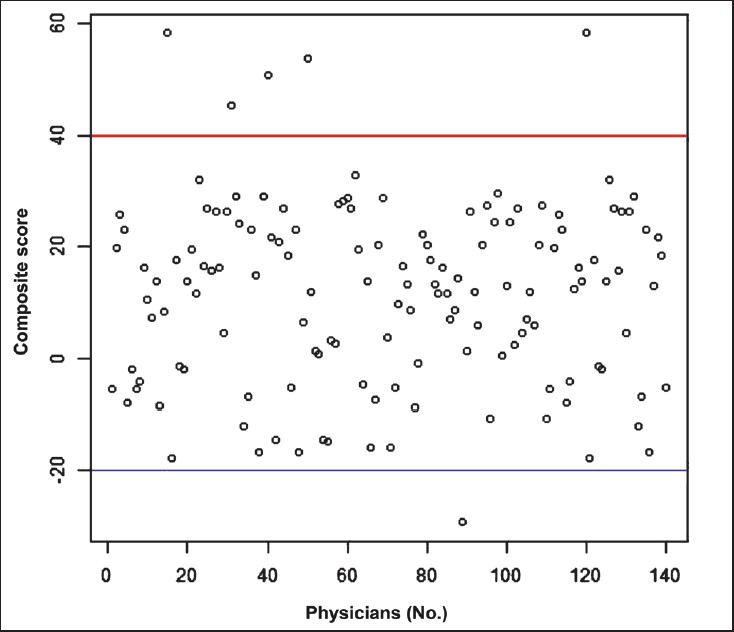
- Composite (average) score of physicians’ satisfaction and dissatisfaction to see the outliers or exceptionally high individual score. Horizontal lines inside the graphs represent those physicians, whose composite scores are exceptionally low or high among all. X-axis represent number of physicians.
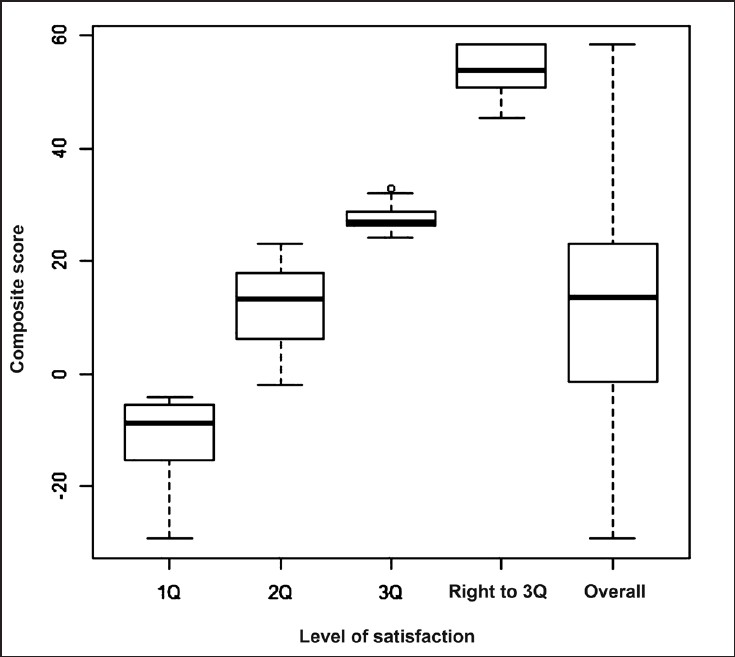
- Box plot to explore whether any individual separate category exists on physicians’ satisfaction. Distribution of composite score of the physician is shown by Boxplot that is divided into four different category on the basis of quartile among with overall distribution of composite score.
Composite score of questions and components showed that 88 per cent (37 of 42) questions and 87 per cent (13 of 15) components were contributing to the satisfaction only, while 12 per cent (5 of 42) questions and 13 per cent (2 of 15) components were contributing to the dissatisfaction (Table II and Fig. 4). Question contributing to satisfaction and dissatisfaction scored on an average 47.05 ± 22.23 and -22.31 ± 08.33, respectively from maximum score of ± 194.42 (Table II).

- Distribution of components to explore which indicator (s) is (are) contributing to physician satisfaction and dissatisfaction.
Univariate statistical test (χ2-test / Fisher exact test) showed that question and components C9, C10, C13, C14 and C15 (Appendix) were not significantly associated with satisfaction/dissatisfaction. Association with the present institute (Median= 24 months, P=0.05) and Working hours (Median=10 h, P=0.01) were significantly associated, while income, sex, institute, discipline, and designation were not.
PCA returned the components C5, C7 and C12 as the leading indicators for estimating satisfaction and dissatisfaction of the physicians. PCA also showed that components created intuitively in the questionnaire were almost similar to PCA-components for almost 10 out of 15. However, questions under the remaining five components appeared as independent components in PCA. Variable selection with and without Part-A variables in the questionnaire found suitable model with the following components for estimation of satisfaction and dissatisfaction. Model [Akaike information criteria (AIC=10)] with Part-A variables incorporated Designation, Discipline, C3, C8, C10, C12 as indicators. Model (AIC=10) without Part-A variables exhibited C3, C7, C11 and C14 as indicators.
Discussion
The results of this study showed that about two-third physicians were satisfied from their job. Similarly, 70 per cent physicians have been reported satisfied in a study conducted at a tertiary care medical institute in Delhi, India10. Similar proportion of satisfaction has also been reported in a study conducted among physicians working at Employee State Insurance (ESI) in India17.
However, some studies reported contradictory findings. About half of the doctors working at a tertiary care hospital at New Delhi, India, were satisfied with their profession, the percentage decreased to 40 per cent for the physicians working at the Armed Forces Medical College in Pune, India918.
Studies conducted in developed countries also support the findings of this study. A study of United Kingdom reported high proportion of physicians’ satisfaction with satisfaction scores 19.9-22.8 out of 256. High proportions of satisfaction have been reported in the studies conducted on Canadian gynaecologic oncologists and Kuwait's physicians819. Other studies have reported 50 per cent satisfaction for Norwegian doctors, 33 per cent for Korean primary care physicians and 32 per cent for physicians of three teaching hospitals of Karachi, Pakistan19202122.
Univariate testing procedure showed that the components C1, C2, C3, C4, C5, C7, C8, C11 and C12 were significantly associated with satisfaction and could be considered as indicators to measure satisfaction/dissatisfaction. However, components C3, C5, C7, C11 and C12 were also identified under PCA and GLM approaches. The component C14 turned out as a predictor in the GLM conducted without Part-A variables and associated with dissatisfaction, however, it could not be identified by other statistical approaches.
Components found significant in this study showed close resemblance with other studies. For example, one study showed that better lifestyle, working environment and higher rate of pay were the main factors of satisfaction22. Another study showed that poor utilization of skills dissatisfied majority (80.8%) of doctors17. Pay has been reported as an important component in different studies101821.
In two different stdies1023, 48 per cent doctors were not satisfied with their working environment, while 49.6 per cent of the doctors were dissatisfied with the average number of working hours per day. Another study reported that long working hours and sleep deprivation were the major causes of dissatisfaction among junior doctors24. Institutes and gender were not found significantly associated with satisfaction and dissatisfaction in this study and similar results have been reported by the studies conducted in developed countries325.
In conclusion, the pattern of high proportion of satisfaction of the Indian physicians reported was similar to the physicians’ satisfaction working particularly in the developed countries. Average physicians’ low satisfaction composite scores indicate that the expectation of Indian physicians from job providers is minimal. Nine components obtained in this study as important indicators for assessment of satisfaction/ dissatisfaction can be used not only by health service system but also by other industries for assessment of their professionals’ job satisfaction.
Acknowledgment
Authors thank all administrative authorities and physicians of both the institutes for their consistent support.
References
- Physicians’ characteristics influence patients’ adherence to medical treatment: results from the medical outcomes study. Health Psychol. 1993;12:93-102.
- [Google Scholar]
- Is the professional satisfaction of general intern ists associated with patient satisfaction? J Gen Intern Med. 2000;15:122-8.
- [Google Scholar]
- Predictors of physician career satisfaction, work-life balance, and burnout. Obstet Gynecol. 2007;109:949-55.
- [Google Scholar]
- German physicians “on strike”-shedding light on the roots of physician dissatisfaction. Health Policy. 2007;82:357-65.
- [Google Scholar]
- UK senior doctors’ career destinations, job satisfaction, and future intentions: questionnaire survey. BMJ. 2002;325:685-6.
- [Google Scholar]
- Job satisfaction in general practice: implications for prescribing. Soc Sci Med Med Psychol Med Sociol. 1980;14A:495-9.
- [Google Scholar]
- Job satisfaction, stress, and burnout among Canadian gynecologic oncologists. Gynecol Oncol. 2004;94:134-9.
- [Google Scholar]
- Correlates of job satisfaction in medical officers. Med J Armed Forces India. 2004;60:329-32.
- [Google Scholar]
- Job satisfaction among doctors in a tertiary care teaching hospital. JK Sci. 2008;10:81-3.
- [Google Scholar]
- Changes in career satisfaction among primary care and specialist physicians, 1997-2001. JAMA. 2003;289:442-9.
- [Google Scholar]
- Physician career satisfaction across specialties. Arch Intern Med. 2002;162:1577-84.
- [Google Scholar]
- Satisfaction of health care providers and quality assurance in Spanish hospitals. Work Stress. 1992;6:229-38.
- [Google Scholar]
- Scales for the measurement of some work attitudes. and aspects of psychological well-being. J Occup Organ Psychol. 1979;52:129-48.
- [Google Scholar]
- A study of job satisfaction among doctors in ESI Corporation, Delhi. Hosp Admin. 1992;29:30-6.
- [Google Scholar]
- A study of job satisfaction and work environment perception among doctors in a tertiary hospital in Delhi. Indian J Med Sci. 2009;63:139-44.
- [Google Scholar]
- Job satisfaction of primary health care physicians at capital health region, Kuwait. 2005. Middle East J Fam Med. 3 Available from: http://www.mejfm.com/journal/july05/job-satisfaction.htm
- [Google Scholar]
- Comparison of job satisfaction and stress among male and female doctors in teaching hospitals of Karachi. J Ayub Med Coll Abbottabad. 2004;16:23-7.
- [Google Scholar]
- Job satisfaction and trust in Health Insurance Review Agency among Korean physicians. Health Policy. 2008;87:249-57.
- [Google Scholar]
- Unhappy doctors. A longitudinal study of life and job satisfaction among Norwegian doctors 1995-2002? BMC Health Serv Res. 2005;5:44.
- [Google Scholar]
- Job satisfaction among doctors working at teaching hospital of Bahawalpur, Pakistan. J Ayub Med Coll Abbottabad. 2007;19:42-5.
- [Google Scholar]
- Satisfactions, dissatisfactions, and causes of stress in medical practice. JAMA. 1979;241:1483-6.
- [Google Scholar]
- Career and parenting satisfaction among medical students, residents and physician teachers at a Canadian medical school. CMAJ. 2000;162:637-40.
- [Google Scholar]
Appendix. Questionnaire