Translate this page into:
Detection of multi-drug resistance & characterization of mutations in Mycobacterium tuberculosis isolates from North- Eastern States of India using GenoType MTBDRplus assay
Reprint requests: Dr Vithal Prasad Myneedu, Head, Department of Microbiology, National Institute of Tuberculosis & Respiratory Diseases, Sri Aurobindo Marg, New Delhi 110 030, India e-mail: tbmicro@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Information on drug resistance tuberculosis is sparse from North-East (N-E) States of India. We undertook this study to detect multi-drug resistant tuberculosis (MDR-TB) among MDR-TB suspects, and common mutations among MDR-TB cases using GenoType MTBDRplus.
Methods:
All MDR suspect patients deposited sputum samples to peripheral designated microscopy centres (DMC) in North-East States. The district TB officers (DTOs) facilitated the transport of samples collected during January 2012 to August 2012 to our laboratory. The line probe assay to detect common mutations in the rpoB gene for rifampicin (RIF) and katG and inhA genes for isoniazid (INH), respectively was performed on 339 samples or cultures.
Results:
A total of 553 sputum samples from MDR suspects were received of which, 181 (32.7%) isolates were found to be multi-drug resistant. Missing WT8 along with mutation in codon S531L was commonest pattern for rifampicin resistant isolates (65.1%) and missing WT along with mutations in codon S315T1 of katG gene was commonest pattern for isoniazid resistant isolates (86.2%). Average turn-around time for dispatch of LPA result to these States from cultures and samples was 23.4 and 5.2 days, respectively.
Interpretations & conclusions:
The MDR-TB among MDR-TB suspects in North-Eastern States of India was found to be 32.7 per cent. The common mutations obtained for RIF and INH in the region were mostly similar to those reported earlier.
Keywords
Drug-resistant
isoniazid
line probe
line probe assay
MDR-TB
rifampicin
tuberculosis

Multi-drug resistant tuberculosis (MDR-TB) poses grave challenge because of prolonged, limited and expensive treatment options with 10 to 30 per cent of cases resulting in failure of treatment and death1. Timely diagnosis and prompt treatment of infectious cases is crucial in curtailing the spread of infection in the community. Conventional drug susceptibility (DST) has been the gold standard but takes upto 4-6 wk after the growth of bacteria. Liquid culture methods, are sensitive and faster but involve prohibitive expenditure2. Commercial line probe assays (LPAs) based on reverse hybridization of amplicons to immobilized membrane based probes covering wild type and mutation sequences have been developed for rapid detection of MDR-TB3. Results of GenoType MTBDRplus for rifampicin (RIF) and isoniazid (INH) resistance are comparable to conventional DST4. Rifampicin resistance is caused by a mis-sense mutation in the beta-subunit of DNA dependent RNA polymerase in 81-bp hotspot region of rpoB gene. Resistance to INH is most frequently associated with mutations in kat G gene and inhA gene5.
The Programmatic Management of Drug Resistant Tuberculosis (PMDT) guidelines in India, identify MDR-TB in suspects using GenoType MTBDRplus (WHO approved) only where it is available6. The National Institute of Tuberculosis and Respiratory Diseases, New Delhi, India is a referral TB hospital and National Reference Laboratory (NRL) for North-Eastern States of India. There are barely any data on MDR-TB from North-East (NE) India. Therefore, this study was aimed at detection of MDR-TB among MDR-TB suspects and common mutations in rpoB, katG and inhA genes using GenoType MTBDRplus in the N-E region.
Material & Methods
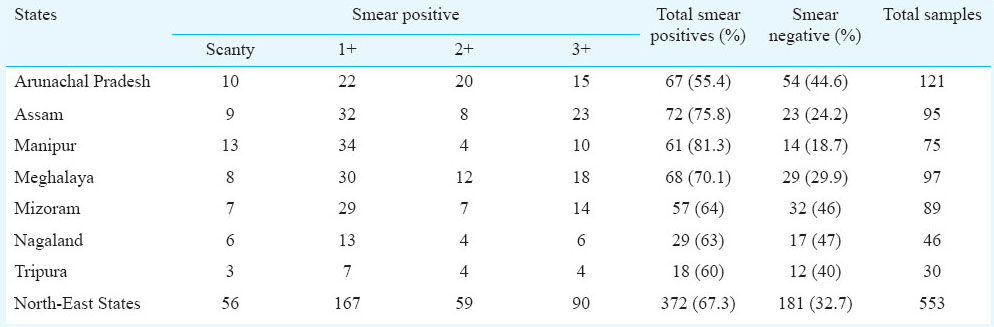
A total of 553 sputum samples from MDR-TB suspect patients from seven North-Eastern States namely Arunachal Pradesh; 121, Assam; 95, Manipur; 75, Meghalaya; 97, Mizoram 89, Nagaland; 46 and Tripura 30 collected during January 2012 to August 2012 were received in the Microbiology Department of the Institute at New Delhi, India. The samples were collected from the patients in each peripheral designated microscopy centres (DMC) in the above States and transported in cold-chain as per PMDT guidelines to this laboratory6. The collection and transport was supervised by the district TB officers (DTOs) in the States. The MDR-suspect patients enrolled under PMDT in these States included TB patients who were either on category I anti-tubercular treatment with fifth month follow up smear positive for acid-fast bacilli (AFB), or category II treatment with four month follow up AFB smear positive or contacts of MDR-TB (Criterion A)6. The study protocol was approved by institute's ethical committee.
Sample processing: All specimens were screened for presence of AFB by Ziehl-Neelsen (ZN) staining7. The samples were processed by N-acetyl-L-cysteine-Sodium hydroxide (NALC-NaOH) method of digestion and decontamination8. All smear positive (> 1+ AFB) sputum samples received within 72 h of sample collection in cold chain were subjected to only LPA after NALC-NaOH processing whereas the remaining samples including smear negative and scanty AFB positive were subjected to culture as per PMDT guidelines36.
Culture: For culture, processed samples were inoculated in MGIT 960 tubes. Tubes flashed positive were identified for Mycobacterium tuberculosis by smear microscopy (serpentine cording) and rapid immuno-chromatographic test (MPT64 TB Ag detection). Cultures positive for M. tuberculosis were subjected to LPA.
Line probe assay: The GenoType MTBDRplus assay (Hain Life Sciences, Nehran, Germany) was carried out as per manufacturer's instructions3. DNA extraction, master-mix preparation, DNA amplification and hybridization were done after thorough cleaning in separate dedicated rooms3. For DNA extraction from NaLC-NaOH processed sample and culture, 500 μl and 1 ml aliquots, respectively were taken. Final DNA obtained was subjected to amplification and the rest was stored at - 20°C3.
Master-mix was prepared using reagents provided in the kit in 45 μl volume to which 5 μl DNA was added3. The PCR products were detected by hybridization using LPA methodology3. The result of DNA strips was interpreted with the help of reporting card as resistant or sensitive for RIF and INH. The presence or absence of all wild type and mutant bands was recorded systematically3.
The reports were communicated electronically to the TB co-ordinators of the respective States. The LPA on any invalid results were repeated using stored processed sample deposits. In each run, M. tuberculosis H37Rv (ATCC 27294) and sterile molecular grade water were included as positive and negative controls, respectively.
Results
Of the 553 patients, 390 were males and 163 were females with a male: female ratio of 2.4: 1. In Tripura, 27 of 30 (90%) of suspects were males. Most patients (424 of 553, 76.7%) belonged to the age group of 15-45 yr which included 224 (40.5%) in the age group 15-29 and 200 (36.2%) in age group 30-45; 113 patients were more than 45 yr whereas 16 were less than 15 years.
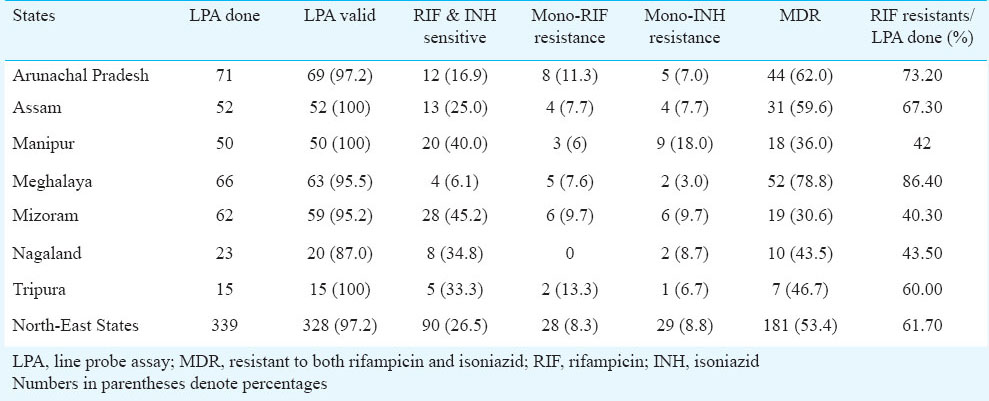
The smear microscopy results are given in Table I. The smear positive and negative patients were 372 (67.3%) and 181 (32.7%), respectively. A total of 339 GenoType MTBDRplus were conducted which included 43 culture isolates obtained from smear negatives/scanty positive cultures. The State-wise data of LPA is detailed in Table II. Valid LPA results were obtained for 328 of 339 (97.8%) strains. Of the 328, 181 (55.2%) tests were found to be resistant to both RIF and INH, 28 (8.5%) were resistant to RIF only, 29 (8.8%) were resistant to INH only and the remaining 90 (27.4%) were sensitive to both RIF and INH. The total RIF resistant cases diagnosed were 209 (63.7%). The LPA result to these states from cultures and samples could be dispatched in an average of 23.4 days and 5.2 days respectively from reviewing of the sample. The TAT of DST using LPA was reduced significantly by 93.5 per cent as compared to solid culture DST (9-12 wk).
The mutations responsible for RIF and INH resistance are displayed in Table III. Among 209 RIF resistant isolates, missing WT (wild type) along with known mutations could be detected in 165 (78.9%). Commonest known RIF mutation was in codon S531L (136/209; 65.1%) followed by D516V mutation (15/209; 7.2%), H526Y mutation (12/209; 5.7%) and H526D mutation (4/209; 1.9%). In 44 (21.1%) RIF resistants, one or more wild type probes were missing with no bands in mutant probes. These 44 included missing WT8 (11; 25 %), missing WT3/ WT4 (9; 20.5%), missing WT2 (7; 15.9%), missing WT7 (5; 11.4%), missing WT1/ WT2 (2; 4.5%), missing WT3 (2; 4.5%), missing WT2/WT3 (1; 2.3%), missing WT2/WT3/W4 (1; 2.3%) missing WT2/WT7 (1; 2.3%), missing WT3/WT4/W8 (1; 2.3%), missing WT4 (1; 2.3%), missing WT4/ WT5 (1; 2.3%), missing WT4/ WT8 (1; 2.3%) and missing WT5/ WT6 (1; 2.3%). Mixed pattern to RIF with all wild type probes present along with presence of one or more mutant bands was found in 7.7 per cent (16/209), commonest being S531L (10; 66.7%).
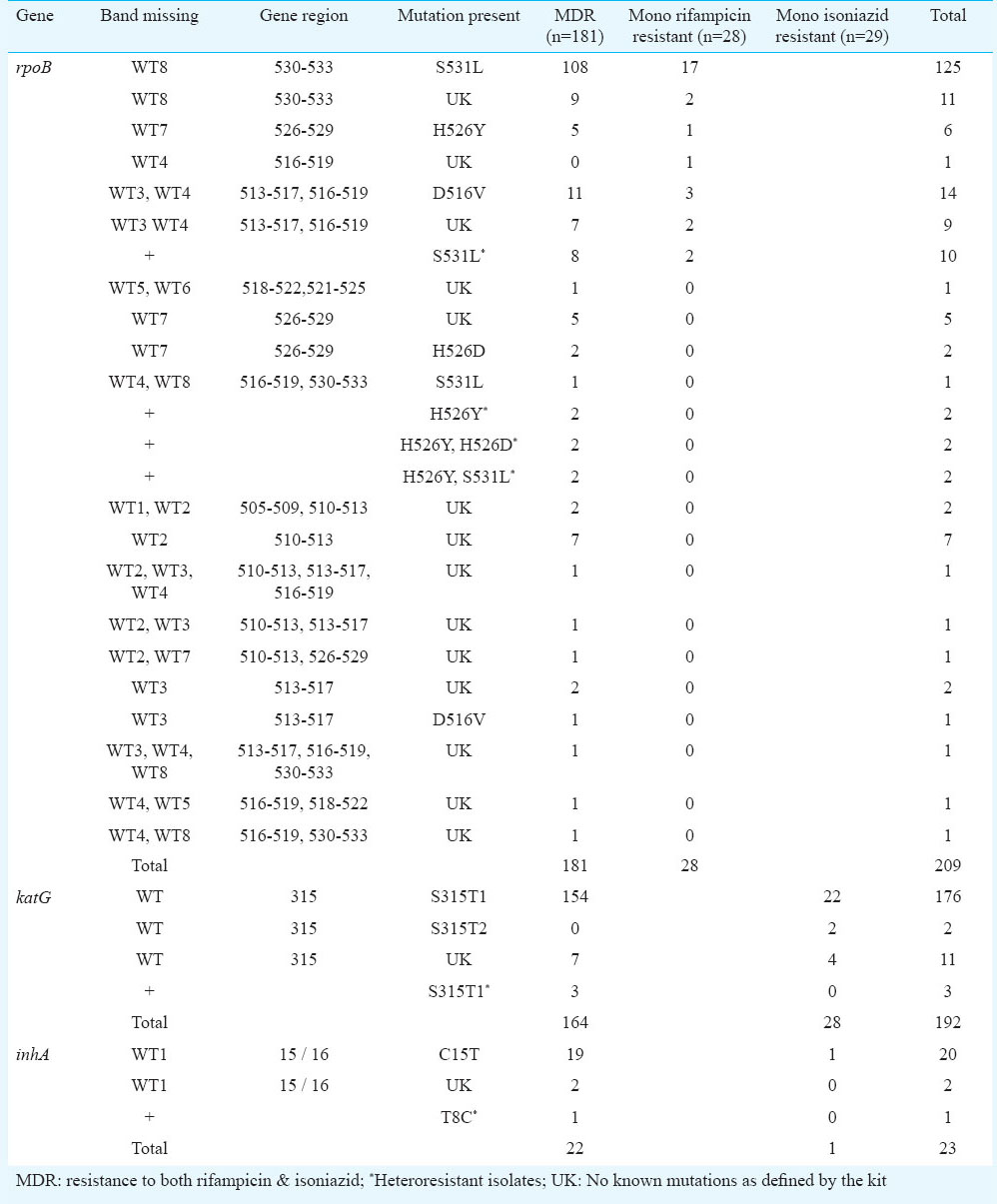
Among 210 INH resistant isolates as detected by MTBDRplus, katG mutations occurred in 192 (91.4%). Mutations in codon S315T1 were detected in 179 (85.2%) of INH resistant or 179 of 192 (93.2%) of katG mutants. Missing wild types with unknown mutant probe among katG were found in 11(5.7%). Mutations in InhA were found in 23 (10.96%) INH resistants, which included 20 (86.95%) C15T and 1 (4.3%) T8C. Both inhA and katG mutations were seen in 5/210 (2.4%) INH resistants. Mixed wild-type and mutant pattern to INH was found in 19 per cent (4/209).
Discussion
Till August 2012, all samples from the region were referred to our institute due to lack of culture and DST or LPA facility. The implementation of TB control in these States is challenging due to poor accessibility, difficult geographical terrains, weak infrastructure and politico-social issues. Males were predominant with 70.5 per cent and majority patients belonged to the young age group of 15-45 yr as is also seen in other studies9. High MDR-TB burden in young adult males have many socio-economic implications. High percentage of MDR-TB of 32.7 per cent among MDR suspects was found in the study. In India, MDR-TB rates have been found to be 17.4 to 53 per cent among previously treated cases who are more likely to develop multi-drug resistance101112.
The average turn-around time (TAT) for LPA was 5.2 days which was slightly higher than that recommended by RNTCP. Theoretically, LPA is completed in less than 72 h but direct microscopy for screening for AFB, NALC-NaOH processing and detailed report typing adds on more days. After amplification, maximum of 20 DNA could be hybridized in one working day on twin-incubator, which added to delay. Other reasons included repeat LPA due to inconclusive results, erratic internet connectivity and holidays.
However, such patients were started on category IV treatment within 1 wk of report communication, thereby curtailing the spread of the diseases.
The GenoType MTBDRplus detects the mutations for RIF and INH, which highly correlate with the sequencing13. In the present study, the test identified RIF resistance by one of four rpoB mutant probes in 78.9 per cent strains, much lesser than in South African study (88.6%)14. Mutation in codon S531L was detected in 65.1 per cent of RIF resistants, whereas other Indian studies found it in 59.8 and 84.6 per cent cases1516. Internationally, S531L mutation has been detected in rates varying from 47 to 70.5 per cent3141718. In some studies S531L mutation occurred more frequently in MDR isolates in comparison to RIF mono-resistants1417. However, we did not find any such difference. The missing wild type probe without any mutant bands was found in 21.1 per cent of RIF resistants as also reported in other studies, New Delhi; 11.1 per cent, Vietnam; 33.3 per cent, France; 29 per cent, Uganda; 42.1 per cent1618317. In GenoType MTBDRplus the entire wild type region is covered by wild type probes whereas only common mutant probes are covered. As per the kit insert provided, absence of any wild type band along with presence or absence of mutant band, accounts for resistance. Such isolates with uncommon mutations could have been identified by sequencing. One limitation of the study was the inability to perform sequencing due to lack of such set up in this facility.
katG mutations account for commonest mechanism of resistance for INH. Specific mutation in codon S315T1 of katG was found in 86.2 per cent of INH resistant isolates, similar to other studies171921. Variations have been reported from France; 62.5 per cent, Uganda; 61.5 per cent and South Africa; 37.6%31714. High prevalence of katG mutations accounts for more INH resistance in high burden countries and high-level INH resistance19.
Mutation in inhA gene accounts for 15-20 per cent of all INH resistant cases and low-level resistance. It was found to be 11.0 per cent, similar to studies elsewhere 5.4 to 21.1 per cent3171820. However, Barnard et al14 reported high prevalence of inhA mutations (41.7%). They also found significant difference in prevalence of mutations in MDR strains as compared to mono-INH resistants14. We did not find any such difference.
Heteroresistance defined as presence of all wild type probes along with presence of one or more mutant bands was found in 7.7 per cent of RIF resistant and in 1.9 per cent of INH resistant isolates unlike a study from Mumbai21. A disadvantage of any genotypic test is a possibility of silent mutation, i.e. mutations which do not lead to change in amino acid hence not leading to phenotypic drug resistance. Resistance originating from mutation of other genes as well as other resistant mechanisms will not be detected by this test. Such mutations could be detected by sequencing.
In conclusion, our study shows the resistance to RIF and INH among M. tuberculosis isolates obtained from MDR-TB suspects of North-Eastern region of India using the GenoType MTBDRplus assay. In addition, information on the common mutations in the rpoB, katG and inhA regions associated with resistance in also provided.
Acknowledgment
Authors acknowledge the FIND, India for technical help and financial support.
References
- Emergence of Mycobacterium tuberculosis with extensive resistance to second line drugs-world-wide, 2000-2004. MMWR Morb Mortal Wkly Rep CDC. 2006;55:301-5.
- [Google Scholar]
- Comparison of recoveries of Mycobacterium tuberculosis using the automated BACTEC MGIT 960 system, the BACTEC 460 TB system, and Löwenstein-Jensen medium. J Clin Microbiol. 2000;38:2395-7.
- [Google Scholar]
- Performance of the GenoType MTBDR line probe assay for detection of resistance to rifampicin and isoniazid in strains of Mycobacterium tuberculosis with low and high level resistance. J Clin Microbiol. 2006;44:3659-64.
- [Google Scholar]
- GenoType MTBDR assays for the diagnosis of multi-drug resistant tuberculosis. Eur Respir J. 2008;32:1165-74.
- [Google Scholar]
- Multi-drug resistant Mycobacterium tuberculosis. Molecular perspectives. Emerg Infect Dis. 1998;4:195-209.
- [Google Scholar]
- Guidelines on programmatic management of drug resistant TB (PMDT) in India, Revised National Tuberculosis Control Programme (RNTCP) New Delhi: Central Tuberculosis Division, Directorate General of Health Services, Ministry of Health & Family Welfare; 2012.
- [Google Scholar]
- Laboratory manual for sputum smear microscopy. Revised National Tuberculosis Control Programme (RNTCP) New Delhi: Central TB Division, Directorate General of Health Services, Ministry of Health and Family Welfare; 2005.
- [Google Scholar]
- Public health mycobacteriology, A guide for level III Laboratory. Atlanta, GA: U.S.A. Department of Health and Human Services, Public health services. Center for Disease Control; 1985.
- [Google Scholar]
- Prevalence of multidrug-resistant tuberculosis among newly diagnosed cases of sputum-positive pulmonary tuberculosis. Indian J Med Res. 2011;133:308-11.
- [Google Scholar]
- Surveillance of drug resistant tuberculosis in the state of Gujarat, India. Int J Tuberc Lung Dis. 2009;134:1154-60.
- [Google Scholar]
- Acquired drug resistance pattern in tuberculosis cases at the State Tuberculosis Centre, Delhi, India. Int J Tuberc Lung Dis. 2009;13:74-8.
- [Google Scholar]
- First and second line drug resistance patterns among previously treated tuberculosis patients in India. Int J Tuberc Lung Dis. 2010;14:243-6.
- [Google Scholar]
- Comparison of two commercially available DNA line probe assays for detection of multi-drug resistant Mycobacterium tuberculosis. J Clin Microbiol. 2006;44:350-2.
- [Google Scholar]
- Rapid molecular screening for multi-drug resistant tuberculosis in a high-volume public health laboratory in South Africa. Am J Respir Crit Care Med. 2008;177:787-92.
- [Google Scholar]
- Utility of GenoType MTBDRplus assay in rapid diagnosis of multidrug resistant tuberculosis at a tertiary care centre in India. Indian J Med Microbiol. 2012;30:58-63.
- [Google Scholar]
- Comparison of line probe assay with liquid culture for rapid detection of multi-drug resistance in Mycobacterium tuberculosis. Indian J Med Res. 2012;136:31-4.
- [Google Scholar]
- Rapid screening of MDR-TB using molecular line probe assay is feasible in Uganda. BMC Infect Dis. 2010;10:41.
- [Google Scholar]
- Validation of the GenoType MTBDRplus assay for diagnosis of multi-drug resistant tuberculosis in South Vietnam. BMC Infect Dis. 2010;10:149.
- [Google Scholar]
- High prevalence of katG Ser315Thr substitution among isoniazid-resistant Mycobacterium tuberculosis clinical isolates from Northwestern Russia 1996-2001. Antimicrob Agents Chemother. 2002;46:1417-24.
- [Google Scholar]
- Validation of the GenoType MTBDRplus assay for detection of MDR-TB in a public health laboratory in Thailand. BMC Infect Dis. 2010;20:123.
- [Google Scholar]
- Drug resistance mutations and heteroresistance detected using the GenoType MTBDRplus assay and their implication for treatment outcomes inpatients from Mumbai, India. BMC Infect Dis. 2012;12:9.
- [Google Scholar]




